Which book is best to study surgery from? 
Finding Sources
Searching the Web
best surgery textbook medical students residents 2024 2025
The library has a solid collection of general surgery textbooks. Here's a breakdown to help you pick the right one based on your level and goal:
Surgery Textbooks Available in the Library
For Medical Students (Undergrad / Clinical Years)
Bailey and Love's Short Practice of Surgery (28th Edition)
The most popular surgery textbook worldwide for medical students. It covers general surgery principles and clinical practice in a readable, well-organized way. Strong on clinical presentations, operative principles, and exam-relevant content. This is the go-to for most students globally.
S Das - A Manual on Clinical Surgery (13th Edition)
Extremely popular in South Asian medical schools. Concise, clinically focused, and packed with examination-style content. Great for bedside clinical surgery and viva/OSCE prep.
For Postgraduates / Residents
Schwartz's Principles of Surgery (11th Edition)
The gold standard reference for surgery residents. Two-volume set covering scientific principles and clinical practice in depth. Used widely in North American residency programs. Best for in-depth understanding and board exam prep.
Sabiston Textbook of Surgery - The Biological Basis of Modern Surgical Practice
The other major "bible" of surgery alongside Schwartz. Extremely comprehensive, evidence-based, and widely used in US programs. Strong on pathophysiology underpinning surgical decisions.
Mulholland and Greenfield's Surgery - Scientific Principles and Practice (7th Edition)
Excellent for residents wanting strong scientific grounding alongside clinical content.
Current Surgical Therapy (14th Edition)
Problem-oriented, question-and-answer format. Best used as a companion book during residency - not a primary text, but great for case-based learning and exam prep.
Fischer's Mastery of Surgery (8th Edition)
Focused on operative technique. Ideal when you want to understand "how to do" a procedure, not just the principles behind it.
The Niche Pick
Pye's Surgical Handicraft (22nd Edition)
A classic older text with a unique focus on surgical technique and dressing/wound management. More of a historical/supplementary read.
Quick Recommendation by Level
| Level | Best Choice |
|---|---|
| Medical student (global) | Bailey & Love |
| Medical student (South Asia) | S Das Manual |
| Resident / PG (comprehensive) | Schwartz or Sabiston |
| Resident (operative technique) | Fischer's Mastery |
| Resident (quick case review) | Current Surgical Therapy |
Bottom line: Bailey & Love for students, Schwartz or Sabiston for residents. Both Schwartz and Sabiston are equally respected - Schwartz tends to be slightly more concise, while Sabiston leans more toward the biological/pathophysiologic reasoning. Pick whichever style suits you.
Appendicitis surgery step-by-step treatment plan.
Reading File
Finding Sources
Searching PubMed
"appendicitis" AND "appendectomy" AND "treatment"
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
I now have all the content needed for a comprehensive, step-by-step treatment plan. Here is the full answer:
Appendicitis: Step-by-Step Treatment Plan
Step 1 - Diagnosis & Workup
Clinical Assessment
- Classic triad: periumbilical pain migrating to right lower quadrant (RLQ), nausea/vomiting, low-grade fever
- Tenderness at McBurney's point, guarding, rebound tenderness
- Positive Rovsing's, Psoas, and Obturator signs depending on appendix position
Labs
- CBC: leukocytosis (WBC >10,000), left shift
- CRP elevated
- Urinalysis to rule out urinary pathology
- Pregnancy test (beta-hCG) in women of childbearing age
Imaging
- Children & pregnant women: Ultrasound first (avoids radiation); a normal appendix diameter is <6 mm - if visualized as >6 mm with periappendiceal change, appendicitis is confirmed
- Adults: CT abdomen/pelvis with contrast is the most reliable - look for appendix >7 mm diameter, periappendiceal fat stranding, free fluid, thickening of the caecal pole
- Retrocaecal appendicitis can escape ultrasound detection; CT is then the next step
- MRI is used where available, particularly for pregnant patients, with high sensitivity and specificity while avoiding radiation
(Bailey and Love's Short Practice of Surgery, 28th Ed.)
Step 2 - Preoperative Resuscitation & Preparation
- IV access - insert two large-bore cannulas
- IV fluid resuscitation - correct dehydration from fever, vomiting, and poor oral intake
- Make patient NPO immediately
- IV antibiotics - administer preoperatively:
- Monotherapy: piperacillin-tazobactam (preferred for simple and complicated appendicitis)
- Alternatives: second-generation cephalosporin + metronidazole
- For simple appendicitis: a single preoperative dose is sufficient; no postoperative continuation needed
- Analgesia - opioid-sparing multimodal approach; withholding analgesia pending diagnosis is no longer supported
- Foley catheter - placed after induction of general anesthesia to decompress the bladder and avoid port-placement injury
- Nasogastric tube - consider if patient was not fasting (to decompress stomach)
- Consent & marking - discuss laparoscopic approach, possibility of conversion to open, and risks (wound infection, intra-abdominal abscess, bleeding, bowel injury)
(Sabiston Textbook of Surgery; Fischer's Mastery of Surgery, 8th Ed.)
Step 3 - Decision: Operative vs. Nonoperative Management
Uncomplicated Appendicitis
| Approach | Notes |
|---|---|
| Operative (standard) | Laparoscopic appendectomy within 12-24 hours - preferred by most surgeons |
| Nonoperative (antibiotics alone) | Acceptable in carefully selected adults without fecalith; ~80-90% initial success but ~40% recurrence at medium-term follow-up; nonoperative management is increasingly accepted but is not yet the default standard |
Key update (2025): The World Society of Emergency Surgery Jerusalem Guidelines (2025) and a 2025 Lancet meta-analysis (PMID: 39827891) confirm that nonoperative antibiotic treatment is a valid option for uncomplicated appendicitis in adults, though recurrence and eventual appendectomy rates remain significant.
Complicated (Perforated/Gangrenous) Appendicitis
- Appendectomy + continue postoperative antibiotics for 4 days after source control
- Periappendiceal abscess (presenting >5 days): percutaneous image-guided drainage first, then interval appendectomy at 6-8 weeks
- Immunosuppressed patients or those with inadequate source control: extend antibiotic course
(Sabiston; Current Surgical Therapy 14e; Schwartz's 11th Ed.)
Step 4 - Laparoscopic Appendectomy (Standard Procedure)
Laparoscopic appendectomy is now the universally accepted standard of care - associated with fewer wound complications, less postoperative pain, shorter hospital stay, and better cosmesis vs. open.
4a. Operating Room Setup
- General anesthesia induced
- Patient positioned supine, left arm tucked
- Surgeon and assistant stand on the patient's left side
- Monitor positioned on the patient's right side at the level of the ASIS
- Standard sterile prep and drape of the abdomen
4b. Port Placement
Three ports are placed as shown:
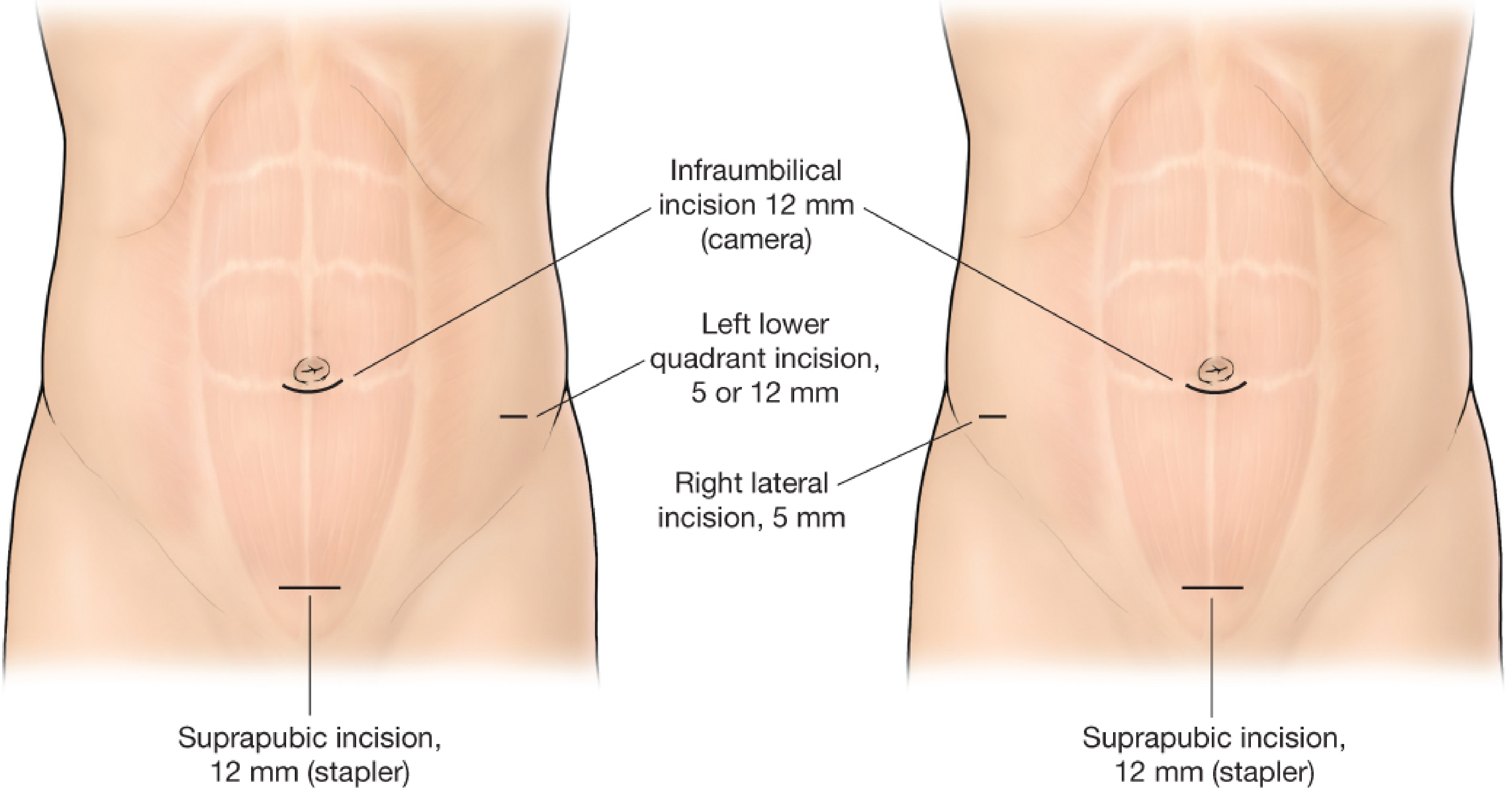
- 12 mm infraumbilical port - camera port (primary access)
- 12 mm suprapubic port - stapler port
- 5 mm left lower quadrant port - working port (or right lateral 5 mm)
Abdominal access technique (surgeon's choice):
- Open Hassan technique (safest, most common): vertical incision just above umbilicus, fascia grasped with Kocher clamps, elevated, and incised; blunt 12-mm trocar inserted, pneumoperitoneum established with CO₂
- Alternatives: Veress needle or optiview technique
Inspect the entry site immediately for inadvertent visceral injury.
4c. Patient Positioning After Ports
Once ports are placed, tilt the table to reverse Trendelenburg, left side down - this shifts bowel away from the RLQ and improves appendix visualization. Move the camera to the LLQ port for proper triangulation.
4d. Identifying the Appendix
- Sweep small bowel out of the RLQ to expose the caecum and terminal ileum
- Anatomical landmarks to locate the appendix:
- Teniae coli of the right colon all converge at the caecal base - the appendix arises here
- Ileal sail (antimesenteric fat on terminal ileum) guides you toward the appendix
- Ligament of Treves attaches from terminal ileum to the appendix base
- Mobilize the appendix as needed; a retrocaecal appendix requires mobilization of the caecum and ascending colon (identify and protect the ureter)
4e. Dissection of the Mesoappendix
- Retract the appendix toward the anterior abdominal wall with the left-hand instrument
- Use a Maryland dissector in the right hand to create a window between the appendix base and the mesoappendix - do this carefully under direct vision to avoid caecal injury
- Vary tension and angle as needed to see all sides during dissection
4f. Transection of the Appendix
- Once the window is established at the base:
- Linear cutting stapler (endo-GIA, 3.5-mm staple height) introduced through the 12-mm port; smaller jaw passed through the window; ensure distal jaw tips are visible before firing
- If the caecum is inflamed/perforated/gangrenous: transect above the area of involvement to include a normal rim of caecum on the proximal stump
- Alternative: endoloop ligation (two loops distal, one proximal) and divide with laparoscopic scissors - requires mesoappendix division first
4g. Division of the Mesoappendix
- Divide along the length of the appendix using vascular load endo-GIA (2.5-mm staple height) - may need multiple loads
- Alternatives: laparoscopic clips on the appendicular artery, or energy device (LigaSure, Harmonic scalpel)
4h. Specimen Removal & Field Check
- Place the appendix in a laparoscopic retrieval bag
- Inspect for hemostasis; inspect the appendiceal stump for secure closure
- Remove the bag via the 12-mm port
- Irrigate the RLQ if contaminated; evacuate any purulent fluid (benefit of copious saline irrigation is unproven but commonly practiced)
4i. Closure
- Remove ports under direct vision
- Close the fascia at the 12-mm port site with absorbable suture (interrupted or figure-of-eight)
- Close all skin incisions subcuticularly with absorbable suture
(Fischer's Mastery of Surgery, 8th Ed.; Sabiston Textbook of Surgery)
Step 5 - Open Appendectomy (Grid-Iron / McBurney Incision)
When laparoscopy is unavailable or conversion is required:
- Lanz/McBurney incision in the RLQ (over McBurney's point)
- Grid-iron muscle-splitting approach through external oblique, internal oblique, and transversus abdominis
- Identify caecum, deliver appendix into wound
- Ligate and divide the mesoappendix (clamp - divide - ligate the appendicular artery)
- Crush the appendix base with a clamp, ligate with absorbable suture (e.g., 2-0 Vicryl), and divide
- Optional: invaginate the stump into the caecum with a purse-string or Z-suture (not universally practiced)
- Close in layers
(Schwartz's Principles of Surgery, 11th Ed.)
Step 6 - Postoperative Care
Uncomplicated Appendicitis
- Remove Foley and NG tube before waking from anaesthesia
- No postoperative antibiotics needed
- Resume oral diet as tolerated upon waking
- Advance to solid food the next day
- Same-day discharge is possible in many patients with early disease
- Oral multimodal analgesia (NSAIDs + paracetamol); minimize opioids
Complicated Appendicitis
- Continue IV antibiotics for 4 days after source control; extend if febrile, leukocytotic, ileus persists, or immunosuppressed
- VTE prophylaxis based on risk stratification (LMWH + compression stockings)
- Pain control with opioid-sparing strategies + regional blocks as needed
- Monitor for clinical deterioration or failure to improve
(Fischer's Mastery of Surgery, 8th Ed.)
Step 7 - Complications & Their Management
| Complication | Incidence | Management |
|---|---|---|
| Superficial surgical site infection | Most common | Open wound, dress; add antibiotics if systemic signs |
| Intra-abdominal/pelvic abscess | Up to 40% in perforated cases | Percutaneous CT-guided drainage + antibiotics |
| Stump appendicitis | 0.002-0.15% | Re-exploration and resection of remnant |
| Bowel injury / bleeding | Rare | Intraoperative recognition and repair |
| Fascial dehiscence | Very rare | Surgical re-exploration |
(Fischer's Mastery of Surgery, 8th Ed.; Sabiston Textbook of Surgery)
Special Populations
- Children: Laparoscopic appendectomy is standard; nonoperative management accepted in selected simple cases but 40% recurrence rate; children <5 years often present already perforated
- Pregnant patients: MRI or US preferred over CT; laparoscopic approach is safe throughout pregnancy and is still the preferred approach; highest risk of fetal mortality is in perforated/delayed cases
- Perforated appendicitis with phlegmon (>5 days symptoms): Drain first, interval appendectomy at 6-8 weeks
Recent Evidence Update
Three high-quality publications are relevant to current practice:
- SAGES 2024 Guideline (PMID: 38740595) - systematic review supporting laparoscopic appendectomy as standard and addressing indications for nonoperative management
- WSES Jerusalem Guidelines 2025 (PMID: 41604201) - the most current international guidelines on diagnosis and treatment
- Lancet Meta-Analysis 2025 (PMID: 39827891) - individual patient data meta-analysis confirming antibiotics are a viable alternative to appendectomy for uncomplicated appendicitis, but with meaningful recurrence rates
These do not overturn surgical treatment as the primary approach but solidify antibiotics as a legitimate shared-decision option for uncomplicated cases in appropriate patients.
This is a shared conversation. Sign in to Orris to start your own chat.