

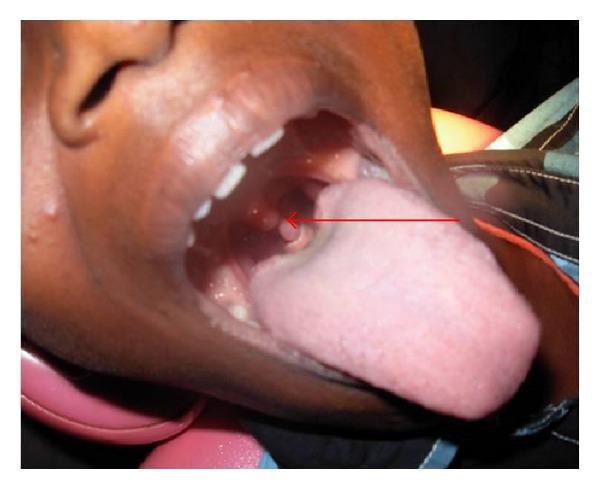
31-year-old male presented with left-sided pain in the upper aspect of his upper lateral aspect of posterior aspect of his hard palate. There is pain when he scrapes his tongue in that region and slight discomfort on the left side when he swallows his saliva. No fever, no swellings, no palpable masses in his neck, no rhinitis. And these are the pictures taken with a torch and the phone's camera of his throat.
unilateral soft palate hard palate lesion pain odynophagia papilloma squamous
Harrison's Principles of Internal Medicine, Twenty First Edition
Page 2309
soft palate papilloma uvula lesion oral cavity

Hugging Face pmc clinical VQA raw
Page 0
Clinical Assessment
Most Likely Diagnosis: Squamous Cell Papilloma of the Soft Palate (HPV-associated)
- Small, smooth, whitish-pink, exophytic nodular lesion(s) on the left soft palate / junction with the posterior hard palate
- No surrounding mucosal breakdown or ulceration visible
- No significant tonsillar enlargement or erythema to suggest acute tonsillitis
- No peritonsillar asymmetry to suggest abscess
Differential Diagnoses
| Diagnosis | For | Against |
|---|---|---|
| Squamous papilloma (HPV 6/11) | Morphology, location, unilateral, benign appearance, no fever | — |
| Fibroma / irritation fibroma | Smooth nodular lesion | Usually firmer, no HPV association, less likely at this site |
| Minor salivary gland tumor (e.g., pleomorphic adenoma) | Hard palate location | Usually submucosal, not exophytic like this |
| Tonsillitis / peritonsillar abscess | Odynophagia, unilateral | No fever, no bulging, no trismus, no erythema of tonsil |
| Oral squamous cell carcinoma | Unilateral lesion with pain | 31 years old, no ulceration, no induration, no cervical lymphadenopathy, benign morphology |
| Lymphoepithelial cyst | Soft palate location | Typically yellowish, cystic, not papillomatous |
Recommended Management
- ENT/Oral medicine referral for formal examination with proper lighting and indirect laryngoscopy
- Surgical excision — this is the treatment of choice for symptomatic oral squamous papillomas. CO₂ laser excision or cold-knife excision with a small margin of normal tissue is standard. Recurrence rate is low.
- Histopathological examination of the excised specimen is mandatory to confirm the diagnosis and exclude any dysplasia (though malignant transformation of HPV 6/11 papillomas is extremely rare).
- No specific antiviral therapy is required.
- HPV status workup is not routinely necessary for isolated oral papillomas in a young immunocompetent adult, but HPV typing of the specimen can be done.
Key Points
- The clinical picture (unilateral soft palate pain, pain with tongue scraping over the area, mild odynophagia without fever or lymphadenopathy) fits a small exophytic benign lesion causing local mechanical irritation.
- The absence of systemic symptoms, cervical lymphadenopathy, and ulceration makes aggressive malignancy very unlikely at this age and presentation.
- However, all oral lesions should be biopsied/excised and sent for histopathology — a clinical diagnosis alone is never sufficient to rule out malignancy, regardless of how benign the appearance.
Continue
oral squamous papilloma soft palate treatment excision recurrence HPV
Urological Infections
Page 54
hard palate soft palate junction benign lesion differential diagnosis minor salivary gland
Bailey and Love's Short Practice of Surgery 28th Edition
Page 860
Continuing: Detailed Management & Follow-Up Plan
Re-examining the Images
- The lesion(s) are situated at the left posterolateral hard palate transitioning into the soft palate — precisely where the patient localizes his pain
- There appear to be 2–3 small, smooth, dome-shaped whitish-pink nodules clustered together, rather than a single large mass
- The texture appears smooth and glistening, not verrucous or cauliflower-like — which can fit either a papilloma or small minor salivary gland benign tumors (e.g., pleomorphic adenoma)
- The surrounding mucosa shows mild vascular prominence/erythema but no frank ulceration
- The uvula appears intact and midline
- There is no visible peritonsillar asymmetry
Refined Differential with Probability Ranking
| Rank | Diagnosis | Reasoning |
|---|---|---|
| 1 | Squamous cell papilloma (HPV 6/11) | Exophytic, smooth-to-nodular, soft palate location, young male, mild mechanical symptoms |
| 2 | Minor salivary gland tumor (pleomorphic adenoma or mucocele) | The hard palate/soft palate junction is a classic site; minor salivary glands are dense here; painless initially but can become symptomatic |
| 3 | Lymphoid hyperplasia / ectopic tonsillar tissue | Nodular pink tissue near palatine arch region; can cause local discomfort |
| 4 | Irritation fibroma | Post-traumatic reactive lesion; smooth, firm |
| 5 | Oral SCC | Must always be on list; effectively excluded clinically here but only histology rules it out |
Step-by-Step Management Plan
- Refer to ENT surgeon or Oral & Maxillofacial surgeon for proper examination under good lighting with a tongue depressor and head mirror/nasopharyngoscope
- Palpation of the lesion is critical — soft and compressible favors papilloma/lymphoid tissue; firm and rubbery favors minor salivary gland tumor
- MRI soft tissue neck (preferred over CT for soft tissue characterization) if any submucosal component is suspected
- Plain imaging is not useful for superficial mucosal lesions
- Surgical excision under local anesthesia — the procedure of choice for both papilloma and benign minor salivary gland tumors at this site
- For papilloma: excise with a thin margin of normal mucosa; CO₂ laser is elegant here to minimize bleeding and provide simultaneous ablation of any subclinical HPV-infected surrounding mucosa
- For minor salivary gland tumor: excise with a cuff of normal tissue down to periosteum if on hard palate
- Mandatory for ALL excised specimens
- Request: routine H&E, and if papilloma — HPV typing is optional but informative
- Review at 2–4 weeks post-excision for wound healing
- If histology confirms benign papilloma: annual oral examination for recurrence or new lesions (recurrence rate with surgical excision is the lowest among treatment modalities, but not zero — HPV remains latent in surrounding tissue)
- If minor salivary gland tumor: longer follow-up per histological subtype
Symptomatic Relief While Awaiting Referral
- Benzydamine hydrochloride (Difflam) oropharyngeal rinse — topical NSAID/local anesthetic; helps with the discomfort on swallowing
- Avoid mechanical trauma to the area (tongue scraping against it, hard foods)
- Saline gargles for mucosal comfort
- No antibiotics are indicated — this is not an infectious/bacterial process
Red Flags to Watch For (Return Immediately)
- Rapid increase in size of the lesion
- Development of ulceration or bleeding
- New cervical lymphadenopathy
- Trismus, worsening dysphagia, or referred otalgia intensifying
- Fever (would shift the differential toward abscess)

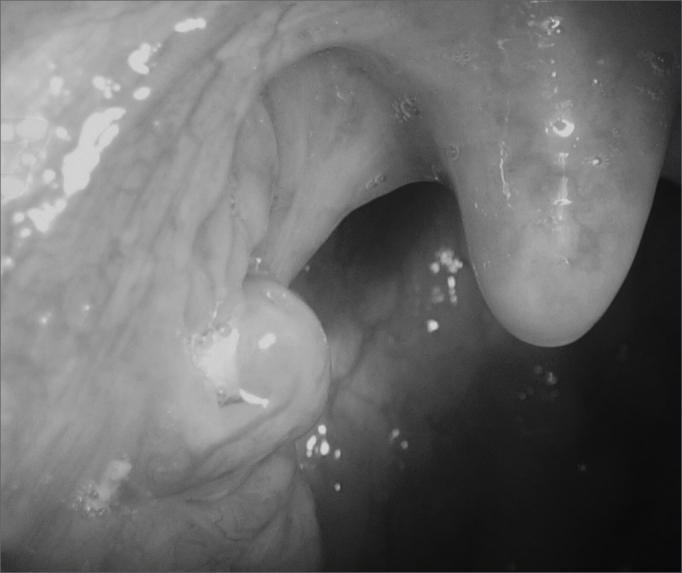
This is the lesion i am referring to
palatine tonsil superior pole tonsillolith cryptic tonsil white lesion pain
Bailey and Love's Short Practice of Surgery 28th Edition
Page 795
tonsil crypt debris unilateral odynophagia no fever treatment
tonsillolith tonsil stone caseous debris cryptic tonsillitis symptoms management
tonsillolith tonsil crypt white plug superior pole palatine tonsil

Hugging Face pmc clinical VQA raw
Page 0
Revised Assessment
What the Lesion Actually Is
- Smooth-surfaced, not verrucous or ulcerated
- Pale white to cream-colored, discrete
- Small (estimated 3–5mm based on image proportions)
- Surrounded by mildly erythematous tonsillar/pillar tissue
Revised Differential Diagnosis
| Rank | Diagnosis | Key Features Supporting It |
|---|---|---|
| 1 | Tonsillolith / cryptic tonsillitis | White/cream nodule at superior tonsil pole, unilateral discomfort, pain on scraping/swallowing, no fever, no systemic illness |
| 2 | Tonsillar retention cyst (lymphoepithelial cyst) | Smooth, dome-shaped, whitish, superficial — clinically very similar; typically asymptomatic but can cause local irritation |
| 3 | Squamous papilloma of the anterior pillar/tonsil | Exophytic pale lesion; less likely given smooth (not papillary) surface |
| 4 | Focal chronic tonsillitis | Persistent crypt plugging with inflammatory changes |
| 5 | Tonsillar SCC | Must not be missed; however the smooth, non-ulcerated, non-indurated appearance and young age make this very unlikely |
Why a Tonsillolith Fits Best
- Location: Superior tonsillar crypt — tonsilloliths commonly form in the upper poles where crypts are deepest
- Color/texture: Off-white, smooth, consistent with calcified/caseous debris
- Symptoms: The pain specifically on scraping the tongue against that spot is characteristic — the stone creates focal mucosal irritation and pressure in the crypt
- Mild odynophagia on the left without fever — classic for a symptomatic tonsillolith causing local inflammation without active infection
- No cervical lymphadenopathy, no fever — argues strongly against acute bacterial tonsillitis or peritonsillar abscess
Management
- Gentle manual dislodgement — using a soft cotton bud or the water jet from a WaterFlosser/oral irrigator aimed at the crypt opening; this often dislodges the stone painlessly
- Saline gargles (warm, isotonic) — help flush crypts and reduce local bacterial load
- Gargling with dilute hydrogen peroxide (1.5%) — loosens debris in crypts
- Avoid aggressive poking with hard instruments — risk of mucosal trauma and bleeding
- ENT referral for incision and marsupialisation or simple needle aspiration under local anaesthesia (for cysts)
- Alternatively, CO₂ laser or coblation of the crypt
- Tonsillectomy is the definitive solution — removes the crypts entirely
- Criteria: recurrent symptomatic tonsilloliths, chronic cryptic tonsillitis, significant halitosis not responding to conservative measures
Key Takeaway
Why not a traumatic ulcer
- The location at the superior tonsil pole / anterior pillar is reachable by a fingernail, toothbrush, or sharp food bolus
- Pain on tongue scraping over the area — consistent with an ulcer surface being mechanically stimulated
- Mild odynophagia — ulcers in this region cause exactly this
- Unilateral, no fever, no lymphadenopathy — fits a simple traumatic/aphthous ulcer
- The lesion appears raised and dome-shaped, with a smooth, convex white surface — traumatic ulcers are characteristically depressed/excavated with a fibrinous white-yellow floor and an erythematous halo around a central crater
- There is no visible surrounding erythematous ring around the white area, which is almost always present in traumatic ulcers
- The image does not show the loss of surface epithelium you would expect — the surface looks intact and smooth, not raw or fibrin-covered
- Traumatic ulcers are typically painful at rest and exquisitely tender on palpation; the patient describes pain specifically when scraping his tongue over it, which suggests more of a mechanical irritation from a raised lesion rather than an exposed ulcer bed
| Feature to Assess | Traumatic Ulcer | Tonsillolith / Cyst |
|---|---|---|
| Surface on palpation | Depressed, raw, tender | Raised, firm or fluctuant |
| Surrounding erythema | Prominent halo | Minimal or absent |
| Can it be dislodged? | No — it is the tissue itself | Yes (tonsillolith pops out) |
| Duration | Heals in 7–14 days spontaneously | Persists unchanged |
| Response to topical steroid | Resolves faster | No change |
Suppose it's a traumatic ulcer and is managed with saline water gargle alone, what is the duration of healing?
- The causative trauma is not repeated (this is the most important factor — if the patient keeps scraping his tongue over it, he is re-traumatising the ulcer bed and resetting the healing clock)
- There is no secondary bacterial infection
Why Saline Works
- Mechanically debride debris and bacteria from the ulcer surface
- Maintain a clean, isotonic environment conducive to re-epithelialisation
- Reduce local bacterial load, preventing secondary infection that would prolong healing
Healing Timeline with Saline Alone
| Day | Expected Change |
|---|---|
| 1–3 | Fibrinous slough stabilises, acute pain begins to reduce |
| 4–7 | Erythematous halo shrinks, ulcer floor starts granulating |
| 7–14 | Re-epithelialisation complete, lesion no longer visible |
Important Caveat — The 2-Week / 3-Week Rule
- If the ulcer has not healed by day 14 with conservative management, the diagnosis must be reconsidered
- If still present at 3 weeks, ENT/oral medicine referral and biopsy are mandatory regardless of how benign it appears — a non-healing ulcer at this site in a 31-year-old must have malignancy actively excluded
- A traumatic ulcer that is truly traumatic and not re-traumatised will always heal within 14 days — persistence beyond this is a red flag
One Practical Instruction for the Patient
How much teaspoons of salt and how much ml of water will give an isotonic preparation of saline water gargle?
The Calculation
- Standard glass of water = 240 ml
- Salt needed = 240 × 0.009 = 2.16 g of NaCl
- 1 level teaspoon of table salt ≈ 5–6 g
¼ teaspoon (approximately 1.5 g) of table salt in 240 ml (one standard glass) of warm water
Practical Instructions
| Parameter | Amount |
|---|---|
| Water | 240 ml (one standard glass) |
| Salt | ¼ level teaspoon |
| Temperature | Warm (not hot) — body temperature ideally |
| Frequency | 3–4 times daily |
| Technique | Gargle for 30–60 seconds, tilt head back to reach the posterior oropharynx, then spit out |