Common pathological ecg finding
Reading File
Finding Sources
Searching the Web
common pathological ECG findings clinical medicine
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Searching Images
pathological ECG findings ST elevation STEMI Q wave bundle branch block
Searching Images
left bundle branch block right bundle branch block ECG pattern
Searching Images
atrial fibrillation ECG ventricular hypertrophy PR interval prolonged
I now have comprehensive content from Harrison's Principles of Internal Medicine and supporting ECG images. Let me compile the full answer.
Common Pathological ECG Findings
A systematic ECG review covers: rhythm, rate, PR interval, QRS duration, QT interval, axis, P waves, voltages, R-wave progression, Q waves, ST segments, T waves, and U waves. Below are the major pathological findings organized by category.
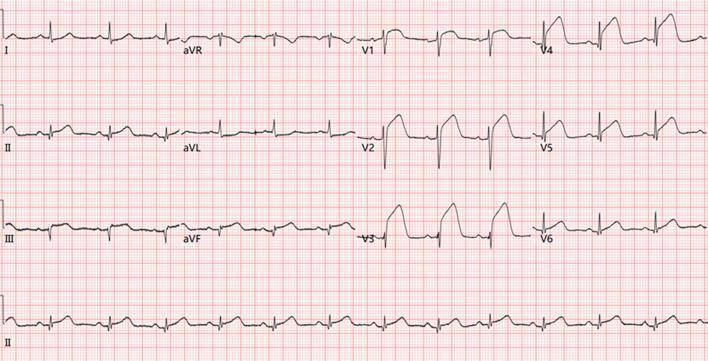
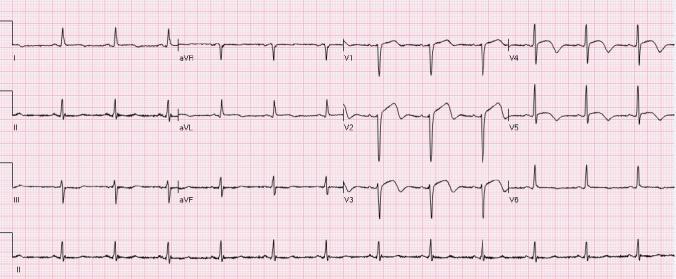
1. Ischemia & Infarction
ST-Segment Elevation (STEMI pattern)
- Transmural (full-thickness) ischemia shifts the ST vector toward the epicardium → ST elevation in leads overlying the ischemic zone
- Earliest sign: tall, broad hyperacute T waves (before ST elevation develops)
- "Tombstoning" / "shark fin" morphology = massive ST elevation merging with T wave → high-risk, often proximal LAD or multi-vessel occlusion
- aVR elevation with diffuse ST depression = left main or proximal LAD occlusion
ST-Segment Depression / Subendocardial Ischemia
- Subendocardial ischemia shifts the ST vector toward the endocardium → ST depression in overlying leads (e.g., anterior precordial leads)
- Typically horizontal or downsloping ≥1 mm
Pathological Q Waves
- Represent myocardial necrosis (transmural scar)
- Criteria: duration ≥40 ms (1 small square) OR depth >25% of the R wave in that lead
- Persist after healed infarction as a permanent marker
- Location indicates infarct territory:
- Q in II, III, aVF = inferior (RCA)
- Q in V1–V4 = anterior (LAD)
- Q in I, aVL, V5–V6 = lateral (LCx)
T-Wave Inversion
- Deep, symmetrical T-wave inversion in anterior leads (V2–V5) = Wellens' syndrome (critical proximal LAD stenosis, reperfused STEMI pattern)
- Diffuse T-wave inversion = may indicate pericarditis (after initial ST elevation), myocarditis, cardiomyopathy, or PE (right precordial leads)
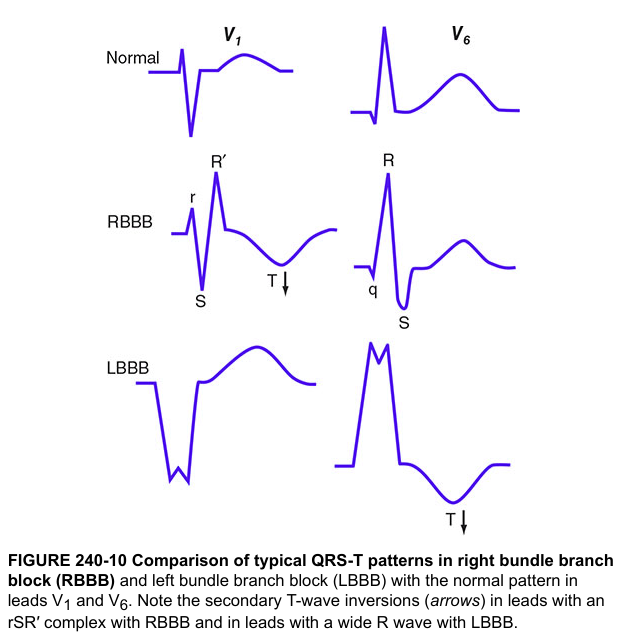
2. Bundle Branch Blocks
Right Bundle Branch Block (RBBB)
- QRS ≥120 ms
- rSR' ("rabbit ears") in V1 — M-shaped wide complex
- Wide, slurred S wave in I and V6
- Secondary T-wave inversions in V1–V3 (discordant with last QRS deflection)
- Causes: PE (acute), RV pressure overload, CAD, congenital heart disease, normal variant
Left Bundle Branch Block (LBBB)
- QRS ≥120 ms
- Broad, notched R wave in V5–V6, I, aVL (no preceding Q)
- Deep, wide S wave in V1
- Secondary T-wave inversions in lateral leads
- Always pathological — associated with CAD, hypertensive heart disease, aortic valve disease, cardiomyopathy
- New LBBB + chest pain = treat as STEMI equivalent
Fascicular Blocks
- Left Anterior Fascicular Block (LAFB): QRS axis more negative than −45° (marked left axis deviation); most common cause of left axis deviation in adults
- Left Posterior Fascicular Block (LPFB): axis >+110°; rare, must exclude other causes
- Bifascicular block (RBBB + LAFB): broad S wave in I/V6 + left axis deviation
3. Arrhythmias
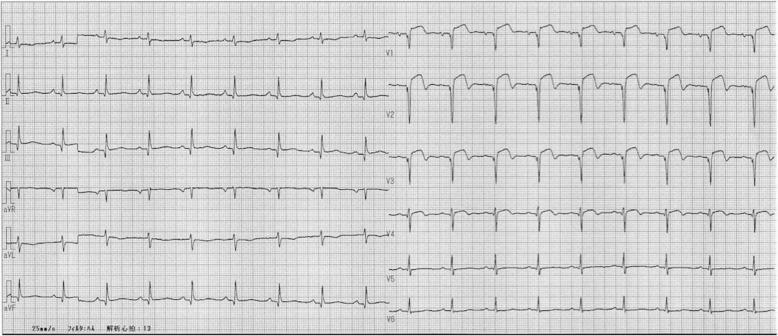
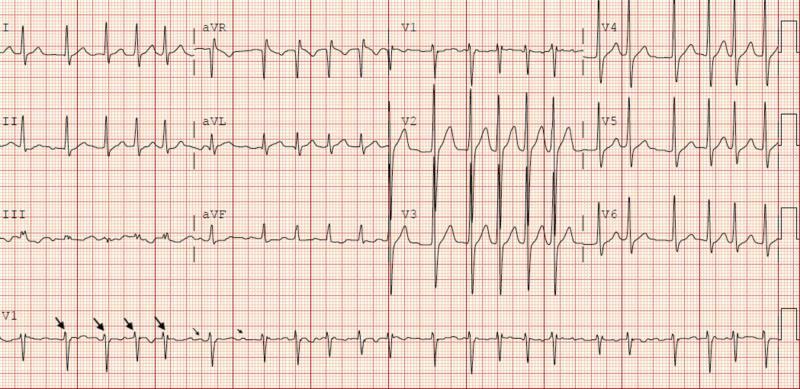
Atrial Fibrillation (AF)
- Irregularly irregular R-R intervals
- Absent P waves replaced by chaotic fibrillatory baseline (best seen in V1)
- Narrow QRS (unless aberrant conduction)
- Associated with LVH, structural heart disease, thyrotoxicosis, alcohol
AV Blocks
| Degree | ECG Feature |
|---|---|
| 1st degree | PR interval >200 ms; every P conducts |
| 2nd degree Mobitz I (Wenckebach) | Progressive PR lengthening → dropped QRS |
| 2nd degree Mobitz II | Fixed PR, sudden dropped QRS (no warning) — higher risk |
| 3rd degree (Complete) | P waves and QRS dissociated; junctional or ventricular escape rhythm |
Pre-excitation (Wolff-Parkinson-White)
- Short PR (<120 ms) + delta wave (slurred upstroke of QRS) + wide QRS
- Due to accessory pathway bypassing AV node
4. Ventricular Hypertrophy
Left Ventricular Hypertrophy (LVH)
- Sokolow-Lyon criteria: S in V1 + R in V5 or V6 ≥35 mm
- Cornell criteria: R in aVL + S in V3 ≥28 mm (men) / ≥20 mm (women)
- Associated strain pattern: ST depression + T-wave inversion in lateral leads (I, aVL, V5–V6)
- Causes: hypertension (most common), aortic stenosis, HCM
Right Ventricular Hypertrophy (RVH)
- Right axis deviation (>+90°)
- Dominant R wave in V1 (R > S in V1)
- Deep S waves in V5–V6
- ST depression + T-wave inversion in right precordial leads (V1–V3)
- Causes: pulmonary hypertension, mitral stenosis, tetralogy of Fallot
5. Electrolyte & Drug Effects
| Cause | ECG Finding |
|---|---|
| Hyperkalemia | Peaked T waves → widened QRS → sine-wave → VF |
| Hypokalemia | Flattened T waves, prominent U waves, QTc prolongation |
| Hypercalcemia | Short QT interval |
| Hypocalcemia | Prolonged QT interval |
| Digoxin | "Reverse tick" ST depression (scooping), PR prolongation |
| Class I antiarrhythmics / TCAs | Wide QRS (sodium channel blockade) |
| Class III agents / QT-prolonging drugs | Prolonged QTc → risk of Torsades de Pointes |
6. QT Prolongation
- QTc >440 ms (men) / >460 ms (women) = pathological
- Predisposes to Torsades de Pointes (polymorphic VT) → VF → sudden death
- Causes: congenital long QT syndrome, drugs (antiarrhythmics, antipsychotics, antibiotics), hypokalemia, hypomagnesemia, hypothyroidism
7. Pericarditis
- Saddle-shaped ST elevation in multiple leads (diffuse, not territory-specific)
- PR segment depression (pathognomonic early finding)
- T-wave inversions develop after ST elevation resolves
- No pathological Q waves
8. Right Heart Strain (Acute PE — "S1Q3T3")
- S wave in lead I + Q wave in III + T-wave inversion in III
- Sinus tachycardia (most common ECG finding in PE)
- New right bundle branch block
- T-wave inversions V1–V4
9. Brugada Pattern
- RBBB morphology + ST elevation in V1–V3 (coved or saddle-back pattern)
- Predisposes to sudden cardiac death from polymorphic VT/VF
- Exacerbated by fever, sodium-channel blocking drugs
Summary Table
| Finding | Key Feature | Key Causes |
|---|---|---|
| ST elevation | Coved ≥1mm in ≥2 contiguous leads | STEMI, pericarditis, Brugada, vasospasm |
| ST depression | Horizontal/downsloping ≥1mm | Subendocardial ischemia, digoxin, LVH strain |
| Pathological Q wave | ≥40ms wide or >25% R wave depth | Old MI, LBBB, HCM |
| LBBB | Wide QRS + notched R in V5–V6 | CAD, HTN, cardiomyopathy |
| RBBB | rSR' in V1 + slurred S in V6 | PE, CAD, normal variant |
| AF | Irregularly irregular, no P waves | Valvular disease, HTN, alcohol |
| LVH | High voltage + strain pattern | Hypertension, aortic stenosis |
| Long QT | QTc >440/460 ms | Drugs, electrolytes, congenital |
| AV block | Progressive/dropped P-R | Ischemia, drugs, fibrosis |
| Pre-excitation | Short PR + delta wave | WPW accessory pathway |
Source: Harrison's Principles of Internal Medicine 22E (2025, McGraw Hill Medical), Chapter 247 — ECG section
This is a shared conversation. Sign in to Orris to start your own chat.