Extensive Tinea corporis and cruris treatment
Reading File
search_medical_text
extensive tinea corporis cruris treatment systemic antifungal therapy
search_medical_text
tinea corporis cruris topical antifungal agents management guidelines
search_medical_image
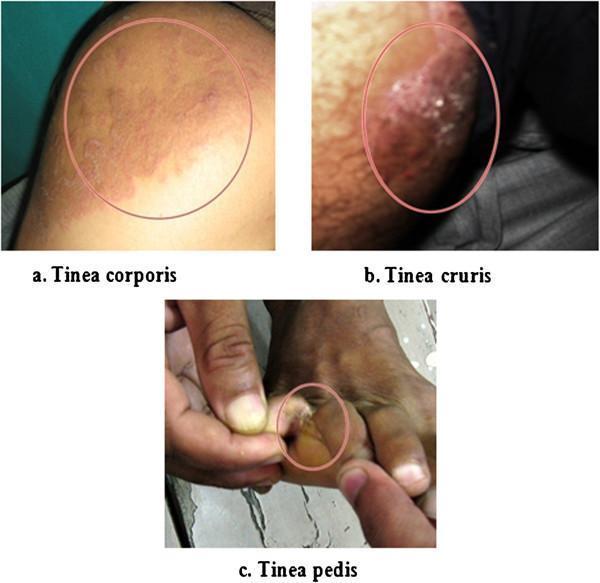
tinea corporis cruris clinical presentation ringworm groin
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive guide to managing extensive Tinea corporis and Tinea cruris:
Overview
Tinea corporis (ringworm of the body) and tinea cruris (jock itch) are superficial dermatophyte infections caused most commonly by Trichophyton rubrum, T. mentagrophytes, and Epidermophyton floccosum. Extensive disease — defined by large body surface area involvement, multiple sites, or treatment-refractory lesions — requires a more aggressive approach than limited infection.
When to Use Systemic (Oral) Therapy
Topical monotherapy is appropriate for limited, uncomplicated tinea corporis/cruris. Oral antifungals are indicated when:
- Extensive skin involvement (large or confluent lesions)
- Multiple anatomical sites affected simultaneously
- Immunocompromised host
- Recalcitrant disease failing topical therapy
- Tinea corporis with concurrent tinea capitis or onychomycosis (which mandate systemic treatment)
(Harrison's, p. 1542 & 6315)
Treatment Options
1. Systemic (Oral) Antifungals — First-Line for Extensive Disease
| Drug | Dose | Duration | Notes |
|---|---|---|---|
| Terbinafine | 250 mg/day PO | 2–4 weeks | First-line; fewer drug interactions than itraconazole; fungicidal |
| Itraconazole | 100–200 mg/day PO | 2–4 weeks | Effective; more drug-drug interactions (CYP3A4); requires acidic stomach for absorption |
| Fluconazole | 150 mg/week PO | 2–4 weeks | Alternative; useful when daily adherence is difficult |
| Griseofulvin | 500 mg/day (microsize) PO | 4–6 weeks | Older agent; less preferred; fungistatic; requires fatty meal for absorption |
Terbinafine is the preferred first-line oral agent due to its fungicidal mechanism, superior efficacy, and lower drug interaction profile compared to itraconazole. (Harrison's, p. 6315)
2. Topical Antifungals — Adjunctive or for Limited Disease
Even in extensive disease, topical therapy can be used adjunctively to accelerate clearance and reduce transmission.
| Agent | Class | Application | Notes |
|---|---|---|---|
| Terbinafine 1% (cream/spray) | Allylamine | Once or twice daily | Fastest clearance; fungicidal |
| Clotrimazole 1% | Azole | Twice daily | Widely available OTC |
| Miconazole 2% | Azole | Twice daily | Available OTC; spray form useful for cruris |
| Econazole 1% | Azole | Once or twice daily | Prescription; good tissue penetration |
| Ketoconazole 2% | Azole | Once daily | Effective; limited by rare hepatotoxicity risk |
| Butenafine 1% | Benzylamine | Once daily | Fungicidal; OTC availability |
| Ciclopirox 0.77% | Hydroxypyridinone | Twice daily | Broad antifungal + antibacterial |
Application tips:
- Apply topicals 1–2 cm beyond the visible border of the lesion
- Continue for 1 week beyond clinical resolution to prevent relapse
- Lotions and sprays are preferred over creams for large or hairy areas
- Powders (e.g., miconazole powder) are useful adjuncts for tinea cruris to reduce moisture
3. Tinea Cruris — Specific Considerations
- Keep the inguinal/groin area as dry as possible — moisture is a key driver of persistence and relapse (Harrison's, p. 6315)
- Wear loose-fitting, breathable (cotton) underwear
- Address concurrent tinea pedis (very common co-infection) to prevent autoinoculation — treat the feet simultaneously
- Avoid topical corticosteroids; if a combination steroid-antifungal (e.g., clotrimazole-betamethasone) was previously used, discontinue the steroid component — prolonged steroid use can cause tinea incognito (masked/atypical presentation with worsening spread)
Practical Management Algorithm
Extensive Tinea Corporis / Cruris
│
▼
Oral antifungal (Terbinafine 250 mg/day × 2–4 weeks)
+
Adjunctive topical antifungal (terbinafine or azole cream/spray BID)
+
Hygiene measures (keep dry, loose clothing, treat tinea pedis)
│
▼
Reassess at 2–4 weeks
│
┌──────┴──────┐
Resolved Persisting
│ │
Maintain Extend oral course OR
hygiene check for re-exposure / immunosuppression /
confirm diagnosis (KOH scraping / culture)
Adjunctive & Preventive Measures
- KOH preparation or fungal culture to confirm diagnosis before prolonged oral therapy
- Rule out or treat diabetes mellitus and immunocompromised states (HIV, corticosteroid use) which predispose to extensive/recurrent infection
- Treat all affected household members and close contacts
- Wash clothing, towels, and bedding that contact affected areas
- Avoid sharing personal items
- Address obesity and excessive sweating (hyperhidrosis), which are predisposing factors for tinea cruris
Monitoring & Safety
| Drug | Key Safety Consideration |
|---|---|
| Terbinafine | Hepatotoxicity (rare); taste/smell disturbances; check LFTs if prolonged use |
| Itraconazole | Negative inotrope — avoid in heart failure; multiple CYP3A4 drug interactions |
| Griseofulvin | Photosensitivity; teratogenic (contraindicated in pregnancy) |
| Fluconazole | QTc prolongation risk with other QT-prolonging drugs |
Key Takeaway
For extensive tinea corporis/cruris, the treatment of choice is oral terbinafine 250 mg/day for 2–4 weeks, combined with a topical antifungal and rigorous hygiene (especially keeping the groin dry and treating co-existing tinea pedis). Itraconazole or fluconazole are acceptable alternatives. Clinical response should be assessed at the end of the course, and the diagnosis should be re-confirmed by KOH/culture if the response is suboptimal. (Harrison's Principles of Internal Medicine, 21st Ed., pp. 1542, 6315)
This is a shared conversation. Sign in to Orris to start your own chat.