Signs of posterior circulation stroke
Reading File
search_medical_text
posterior circulation stroke signs symptoms clinical features
search_medical_text
vertebrobasilar stroke brainstem cerebellum ischemia presentation
search_medical_image
posterior circulation stroke anatomy territory brainstem cerebellum
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive overview of the signs and symptoms of posterior circulation stroke.
Posterior Circulation Stroke
The posterior circulation comprises the paired vertebral arteries, the basilar artery, and the posterior cerebral arteries (PCAs). Strokes in this territory affect the brainstem, cerebellum, thalami, occipital lobes, and parts of the temporal lobes (Harrison's, p. 12110).
Key Clinical Features
Posterior circulation strokes are classically characterized by the "5 Ds" plus additional brainstem signs:
| Feature | Details |
|---|---|
| Diplopia | Cranial nerve III, IV, or VI involvement |
| Dysarthria | Cerebellar or corticobulbar involvement |
| Dysphagia | Involvement of IX/X nuclei (medulla) |
| Dizziness / Vertigo | Vestibular nuclei or cerebellum |
| Drop attacks | Sudden loss of tone without LOC |
| Ataxia | Cerebellar hemisphere or vermis |
| Visual field defects | Homonymous hemianopia (PCA territory) |
Signs by Territory
1. Brainstem (Medulla, Pons, Midbrain)
- Crossed deficits: ipsilateral cranial nerve palsy + contralateral hemiplegia/hemisensory loss — a hallmark of brainstem stroke
- Horner's syndrome (ptosis, miosis, anhidrosis): lateral medullary involvement
- Internuclear ophthalmoplegia (INO): pontine lesion affecting the MLF — adduction deficit ipsilateral, nystagmus contralateral
- Nystagmus: especially vertical or direction-changing, strongly suggests central (posterior fossa) origin
- Locked-in syndrome: bilateral ventral pontine infarction — quadriplegia + anarthria with preserved vertical gaze and consciousness
- Coma/reduced consciousness: reticular activating system involvement (bilateral basilar territory)
2. Cerebellum
- Limb ataxia: ipsilateral cerebellar hemisphere lesion
- Truncal ataxia / gait ataxia: vermis involvement
- Dysmetria, dysdiadochokinesia, intention tremor
- Nausea and vomiting (prominent, often early)
- Headache: occipital or nuchal, often the first symptom
⚠️ Cerebellar infarction with edema can cause obstructive hydrocephalus and tonsillar herniation — a neurosurgical emergency.
3. Posterior Cerebral Artery (PCA)
- Homonymous hemianopia (contralateral) — with macular sparing (if posterior cortex preserved)
- Visual agnosias, alexia without agraphia (dominant hemisphere)
- Prosopagnosia (bilateral occipital involvement)
- Thalamic infarction: contralateral hemisensory loss, thalamic pain syndrome, memory impairment
Named Brainstem Syndromes
| Syndrome | Location | Key Features |
|---|---|---|
| Wallenberg (lateral medullary) | PICA / vertebral | Ipsilateral face pain/temp loss, ipsilateral Horner's, dysphagia, hiccups, contralateral body pain/temp loss |
| Weber | Midbrain | Ipsilateral CN III palsy + contralateral hemiplegia |
| Millard-Gubler | Pons (ventral) | Ipsilateral CN VI + VII palsy + contralateral hemiplegia |
| Foville | Pons | Ipsilateral conjugate gaze palsy + CN VII palsy + contralateral hemiplegia |
| Top of the basilar | Midbrain/thalamus | Vertical gaze palsy, somnolence, visual hallucinations, amnesia |
Imaging: Acute Posterior Circulation Ischemia
The image below illustrates multi-territory cerebellar and brainstem infarction with basilar artery occlusion:
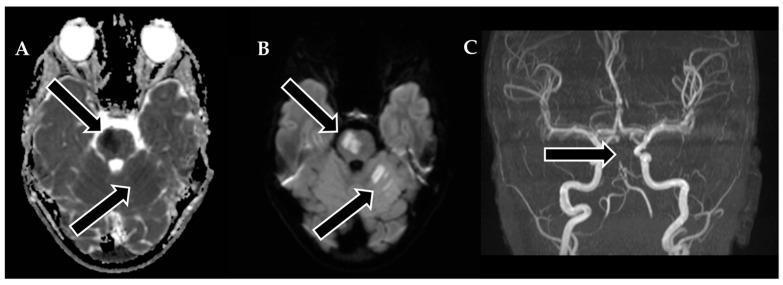
A: ADC map showing hypointense signal (restricted diffusion) in PICA, AICA, and SCA territories. B: DWI confirming acute infarction (bright signal). C: MRA showing abrupt flow cut-off in the distal basilar artery (arrow) — diagnostic of basilar artery occlusion.
Clinical Pearls
- Isolated vertigo can be the sole presenting symptom — use HINTS exam (Head Impulse, Nystagmus, Test of Skew) to differentiate central from peripheral: a normal head impulse test + direction-changing nystagmus + skew deviation = central cause until proven otherwise.
- Posterior circulation strokes are often missed on initial CT (~40% of infarcts invisible in first 24 hours) — MRI DWI is the preferred modality.
- Symptoms tend to fluctuate before major infarction, making early recognition critical.
- Vertebrobasilar TIAs may present with diplopia, vertigo, numbness, weakness, and dysarthria — often together (Harrison's, p. 968).
This is a shared conversation. Sign in to Orris to start your own chat.