Treatment of fever on opd base
Reading File
Finding Sources
Finding Sources
Searching PubMed
fever management outpatient antipyretic
Finding Sources
Finding Sources
Searching PubMed
fever antipyretic treatment
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Searching the Web
fever outpatient treatment guidelines 2024 antipyretic acetaminophen ibuprofen
I now have comprehensive material from Harrison's 22E (2025) and supporting sources to provide a thorough answer. Let me compile the full response.
Treatment of Fever on an OPD Basis
Definition and Threshold
Fever is defined as a body temperature >38°C (>100.4°F), caused by a resetting of the hypothalamic thermostat upward by pyrogenic cytokines (IL-1, IL-6, TNF) acting via prostaglandin E2 (PGE2). Clinically significant fever generally warrants treatment at >38.5°C, and aggressive treatment at >39.5°C.
A temperature >41.5°C is called hyperpyrexia - treat urgently.
Step 1 - Assess and Identify the Cause
Before prescribing antipyretics, a basic clinical evaluation is mandatory:
| Assessment | What to Check |
|---|---|
| History | Duration, pattern (remittent, intermittent, continuous), associated symptoms |
| Exam | Source of infection (throat, ears, lungs, abdomen, skin, lymph nodes, urine) |
| Risk factors | Immunosuppression, recent travel, contacts, medications |
| Danger signs | Altered sensorium, rash + fever (meningococcemia), dyspnea, severe myalgia |
Key distinction: Always rule out hyperthermia (heat stroke, malignant hyperthermia, neuroleptic malignant syndrome) - these do NOT respond to antipyretics and require active cooling.
Step 2 - Non-Pharmacological Measures
- Adequate hydration: oral fluids (water, ORS, coconut water) - fever increases insensible losses
- Tepid sponging: lukewarm (not cold) water to help with heat dissipation - adjunct to antipyretics, not replacement
- Light clothing and ventilation: reduce external heat load
- Rest: reduce metabolic demand and oxygen consumption
Fever increases oxygen consumption by 13% for every 1°C rise above 37°C (Harrison's 22E, p. 180)
Step 3 - Pharmacological Treatment (Antipyretics)
First-Line: Paracetamol (Acetaminophen)
Paracetamol is the preferred first-line antipyretic - works by inhibiting COX centrally and reducing hypothalamic PGE2 synthesis.
| Population | Dose | Frequency | Max Daily |
|---|---|---|---|
| Adults | 500-1000 mg orally | Every 4-6 hours | 4 g/day |
| Children | 10-15 mg/kg/dose orally | Every 4-6 hours | 60-75 mg/kg/day |
| Elderly | 500 mg | Every 6 hours (caution) | 2 g/day |
Why preferred? No adverse effect on platelets, minimal GI irritation, safe in children. Aspirin and NSAIDs can adversely affect platelets and the GI tract. (Harrison's 22E, p. 180)
Alternative/Second-Line: Ibuprofen (NSAID)
| Population | Dose | Frequency |
|---|---|---|
| Adults | 200-400 mg orally | Every 6-8 hours with food |
| Children (>6 months) | 5-10 mg/kg/dose | Every 6-8 hours |
- Often more effective than paracetamol for fever reduction due to its peripheral anti-inflammatory action
- Avoid in: renal impairment, peptic ulcer disease, dehydration, dengue/thrombocytopenia, pregnancy (especially 3rd trimester), age <6 months
- Give with food to reduce GI irritation
Aspirin
- Effective antipyretic but avoided in children under 16 years due to risk of Reye syndrome (Harrison's 22E, p. 180)
- Can be used in adults when indicated (e.g., also treating pain/inflammation)
- Dose: 300-600 mg orally every 4-6 hours
Alternating / Combination Therapy
For persistent or high fever, alternating paracetamol and ibuprofen every 3-4 hours (i.e., giving one every 3 hours, alternating between the two) has been shown in RCTs to be more effective than monotherapy in children aged 6-36 months (dose: paracetamol 12.5 mg/kg and ibuprofen 5 mg/kg, alternating every 4 hours for 3 days).
In adults, combination or alternating use is a practical option for refractory fever in OPD, but avoid exceeding individual drug maximum doses.
Rectal Route (If Oral Not Possible)
Suppositories of paracetamol (125 mg, 250 mg, 500 mg) are available for patients who are vomiting or unable to swallow - same dosing applies.
Step 4 - Who Needs Aggressive Fever Treatment?
Fever treatment is especially important in:
| Condition | Reason |
|---|---|
| Cardiac/pulmonary disease | Fever increases O2 demand; can worsen ischemia or respiratory failure |
| CNS disease / head injury | Hyperthermia worsens neurological outcomes |
| Seizure history (febrile) | Aggressive antipyretic use (though exact threshold triggering febrile seizure is unclear) |
| Pregnancy | High fever associated with neural tube defects in early pregnancy |
| Elderly | Poor thermoregulatory reserve, dehydration risk |
| Severe anemia / sickle cell | Increased metabolic stress |
Step 5 - When to Refer / Admit (Red Flags)
Do NOT manage as outpatient if:
- Fever >40°C not responding to antipyretics
- Fever + petechial/purpuric rash (suspect meningococcemia)
- Fever + altered consciousness (meningitis, encephalitis, sepsis)
- Fever + severe dehydration or unable to take oral fluids
- Immunocompromised patient with fever (HIV, chemotherapy, steroids)
- Neonatal fever (<3 months with temperature >38°C - always refer)
- Fever persisting >7-10 days without a source (investigate for FUO)
Summary Table
| Drug | Dose (Adult) | Advantage | Avoid if |
|---|---|---|---|
| Paracetamol | 500-1000 mg Q4-6h | Preferred, GI-safe, platelet-safe | Liver disease, >4g/day |
| Ibuprofen | 200-400 mg Q6-8h | More potent anti-inflammatory | Renal failure, peptic ulcer, dengue, <6 months |
| Aspirin | 300-600 mg Q4-6h | Analgesic + antipyretic | Children <16 (Reye syndrome), peptic ulcer |
| Naproxen | 250-500 mg Q8-12h | Longer-acting | Renal impairment, GI disease |
Special Note on Tepid Sponging
Do not use cold water or ice packs - this causes vasoconstriction and shivering, which paradoxically raises core temperature. Tepid (lukewarm) water + antipyretics work together: antipyretics lower the hypothalamic set point, then sponging facilitates heat loss by evaporation.
For hyperpyrexia with CNS involvement, cooling blankets + antipyretics may both be needed. (Harrison's 22E, p. 180)
Sources: Harrison's Principles of Internal Medicine 22E (2025), p. 178-180; Swanson's Family Medicine Review; Bailey & Love's Surgery 28th Ed.
Create a flowchart: when to treat fever vs when to investigate further
Generating Image
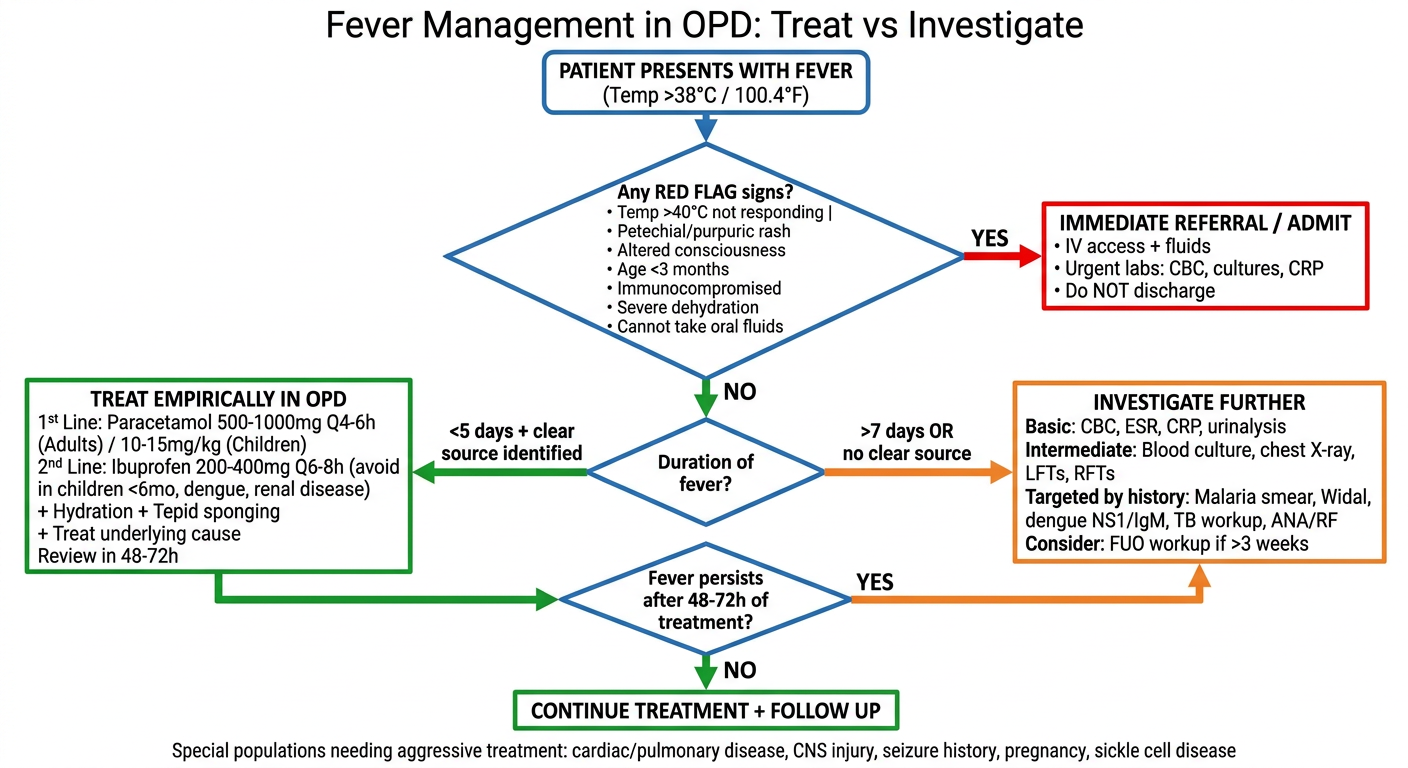
Here's the flowchart for Fever: Treat vs Investigate in OPD. The key decision pathway:
- Red flags present? → Refer/admit immediately (no OPD management)
- No red flags + fever <5 days + clear source? → Treat empirically (paracetamol/ibuprofen + hydration)
- Fever >7 days or no clear source? → Investigate (CBC, cultures, targeted workup)
- Fever persists after 48-72h of treatment? → Escalate to investigation
The color coding follows:
- 🔴 Red - immediate danger, refer
- 🟠 Orange - investigate, escalate
- 🟢 Green - safe to treat in OPD
Let me know if you'd like the flowchart adjusted (e.g., pediatric-specific version, dengue-endemic region version, or a downloadable file format).
This is a shared conversation. Sign in to Orris to start your own chat.