Rheumatpoid arthritis according to robbins book of pathology add flowchart for easjer understanding of pathophysiology
Reading File
Finding Sources
Searching the Web
Robbins pathology rheumatoid arthritis pathophysiology 2024
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
I now have all the content needed from both Robbins books plus the official pathogenesis diagram. Let me compile the comprehensive answer with the flowchart.
Rheumatoid Arthritis - Robbins Pathology
(Based on Robbins & Kumar Basic Pathology and Robbins, Cotran & Kumar Pathologic Basis of Disease)
Definition
Rheumatoid arthritis (RA) is a chronic autoimmune disorder that principally attacks the joints, producing a nonsuppurative, proliferative, and inflammatory synovitis. It often progresses to destruction of articular cartilage and, in some cases, joint fusion (ankylosis). Extraarticular lesions may also occur in the skin, heart, blood vessels, and lungs.
- Prevalence: 0.25-1% in the United States
- 3x more common in females
- Peak incidence: 3rd to 5th decade
Pathogenesis Diagram (from Robbins)
This is the official Robbins figure (Fig. 19.34 / 26.33) illustrating the pathogenesis:
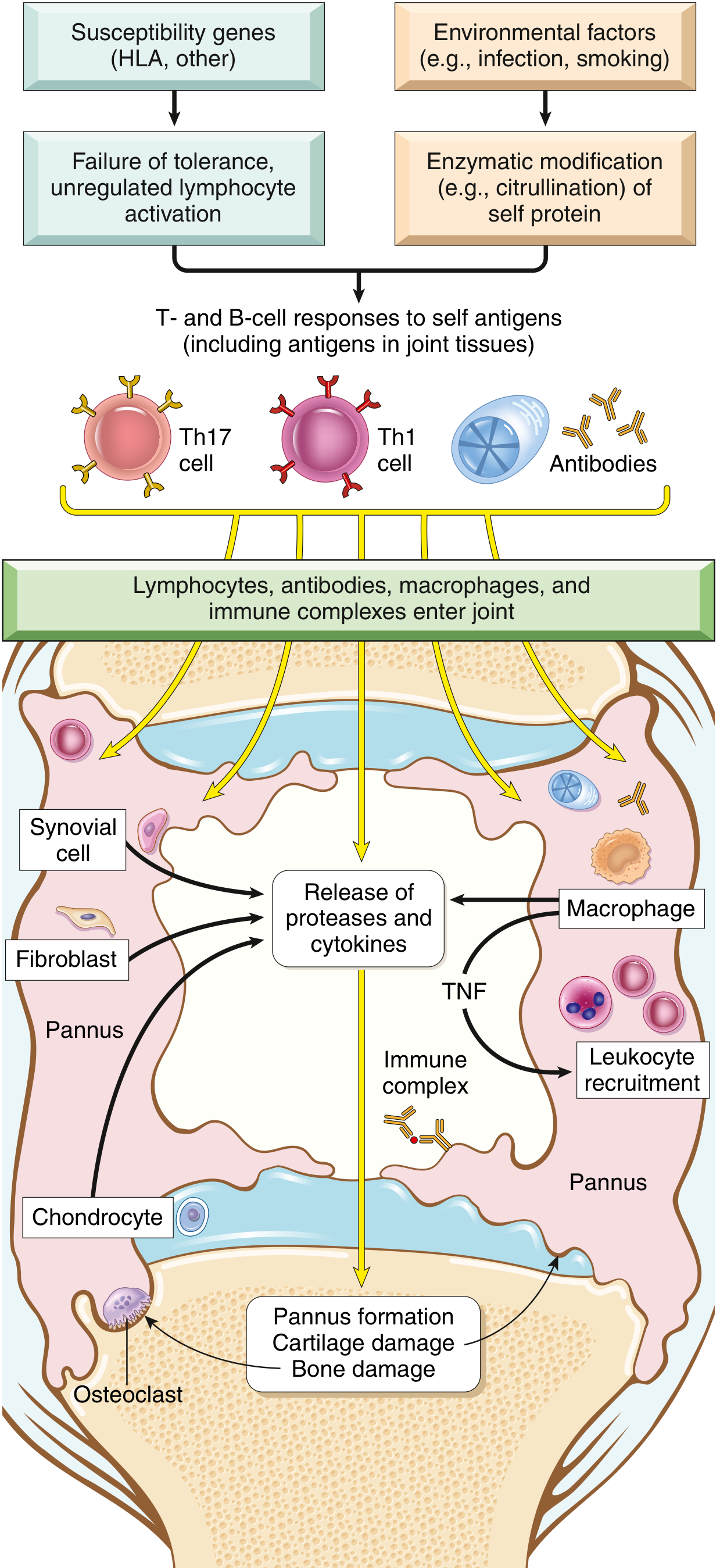
FIG. 19.34/26.33: Major processes involved in the pathogenesis of rheumatoid arthritis. (Robbins Pathology)
Flowchart: Pathophysiology of RA
GENETIC FACTORS ENVIRONMENTAL FACTORS
(HLA-DR4, HLA alleles, (Infection, smoking,
PTPN22 gene variants) periodontitis)
│ │
▼ ▼
Failure of tolerance Enzymatic modification
(unregulated lymphocyte + of self-proteins
activation) (e.g., citrullination of
fibrinogen, collagen,
α-enolase, vinculin)
│ │
└──────────────┬────────────────────┘
▼
T-cell & B-cell responses to SELF ANTIGENS
(especially antigens in joint tissues)
│
┌─────────────┼────────────────┐
▼ ▼ ▼
Th1 cells Th17 cells B cells / Plasma cells
(IFN-γ) (IL-17) │
│ │ ├─► ACPA (Anti-citrullinated
▼ ▼ │ peptide antibodies) - 70%
Activates Recruits ├─► Rheumatoid Factor (IgM/IgA
macrophages neutrophils & │ anti-IgG Fc) - 80%
& synovial monocytes └─► Immune complexes deposited
cells in joints
│
▼
Macrophage activation
→ TNF, IL-1, IL-6 secretion
(TNF = KEY MEDIATOR)
│
┌──────────────┴──────────────────┐
▼ ▼
Recruit & activate Stimulate synovial cells
more leukocytes → to secrete PROTEASES
→ destroy hyaline cartilage
│
▼
RANKL on activated T cells
→ stimulates OSTEOCLASTS
→ BONE RESORPTION + periarticular erosions
│
▼
┌──────────────────────────────────────┐
│ SYNOVIAL CHANGES │
│ │
│ • Synovial cell hyperplasia │
│ • Dense infiltrates (CD4+ T cells, │
│ B cells, macrophages, plasma cells)│
│ • Lymphoid follicles with germinal │
│ centers form │
│ • Increased angiogenesis │
│ • Fibrin-rich exudate + neutrophils │
└──────────────────────────────────────┘
│
▼
PANNUS FORMATION
(mass of edematous synovium +
inflammatory cells + granulation
tissue + fibroblasts)
│
▼
PANNUS grows over & erodes articular cartilage
│
▼
CARTILAGE DESTRUCTION
│
▼
Pannus bridges opposing bones
│
┌─────────┴──────────┐
▼ ▼
Fibrous ankylosis Subchondral cysts
│ + erosions
▼
Bony ankylosis
(bone fusion)
Pathogenesis - Key Details
Triggering Event
The autoimmune response is initiated by CD4+ helper T cells reacting against a joint antigen. Evidence supports molecular mimicry - an epitope on citrullinated vinculin mimics epitopes on microbes and is presented by HLA-DR4.
Key Cytokines and Their Roles
| Cytokine / Mediator | Source | Role |
|---|---|---|
| TNF | Macrophages | Key mediator - recruits leukocytes, activates cells, stimulates proteases. Basis for TNF antagonist therapy |
| IL-1 | Macrophages | Recruits leukocytes, stimulates protease secretion |
| IL-6 | Macrophages | Recruits leukocytes, systemic inflammation |
| IL-17 | Th17 cells | Recruits neutrophils and monocytes |
| IFN-γ | Th1 cells | Activates macrophages and resident synovial cells |
| RANKL | Activated T cells | Stimulates osteoclasts → bone resorption |
Autoantibodies
- ACPA (Anti-citrullinated peptide antibody): Present in ~70% of patients. More specific for RA. Associated with disease severity. Target proteins include fibrinogen, type II collagen, α-enolase, vimentin/vinculin.
- Rheumatoid Factor (RF): IgM or IgA antibodies against Fc of IgG. Present in ~80% of patients. Not exclusive to RA (can be present without RA).
Morphology (Gross & Microscopic)
Joint Changes
The synovium becomes edematous, thickened, and hyperplastic, with a smooth contour replaced by delicate and bulbous villi.
Histologic hallmarks (5 features):
- Synovial cell hyperplasia and proliferation
- Dense inflammatory infiltrate - CD4+ T cells, B cells (forming lymphoid follicles), plasma cells, dendritic cells, macrophages
- Increased vascularity (angiogenesis)
- Fibrin-rich exudate with neutrophils on synovial surfaces
- Osteoclastic activity in subchondral bone - inflamed synovium penetrates bone, causing periarticular erosions and subchondral cysts
The pannus is defined as: a mass of edematous synovium + inflammatory cells + granulation tissue + fibroblasts that grows over and erodes articular cartilage. Eventually leads to fibrous and then bony ankylosis.
Rheumatoid Nodules
- Infrequent, occur in subcutaneous tissue over forearm, elbows, occiput, lumbosacral area
- Microscopically: central zone of fibrinoid necrosis surrounded by a rim of activated macrophages (palisading) + lymphocytes + plasma cells
Extraarticular
- Leukocytoclastic vasculitis (small and large arteries)
- Pleural, pericardial, or pulmonary involvement
- Uveitis and keratoconjunctivitis
Clinical Features
- Begins with malaise, fatigue, generalized musculoskeletal pain (weeks to months before joint involvement)
- Symmetric arthritis of small joints first (hands and feet), then wrists, ankles, elbows, knees
- In hands: MCP and PIP joints involved (not DIP, unlike OA)
- Pain worse in morning or after inactivity (morning stiffness > 1 hour)
- Characteristic deformities: ulnar deviation, swan-neck deformity, boutonnière deformity
- Radiographic findings: joint effusions, juxtaarticular osteopenia, erosions, joint space narrowing, cartilage loss
OA vs RA (Robbins Comparison)
| Feature | Osteoarthritis | Rheumatoid Arthritis |
|---|---|---|
| Pathogenesis | Mechanical wear + cartilage degradation | Autoimmune (CD4+ T cells) |
| Inflammation | Minimal | Prominent synovitis |
| Joint distribution | Asymmetric, weight-bearing | Symmetric, small joints |
| MCP/PIP | Spared | Involved |
| DIP joints | Heberden's nodes | Usually spared |
| Morning stiffness | Brief (<30 min) | Prolonged (>1 hr) |
| Autoantibodies | None | ACPA, Rheumatoid Factor |
| Pannus formation | Absent | Present |
| Systemic features | Absent | Present |
Treatment Rationale (Robbins)
- Corticosteroids: anti-inflammatory
- Methotrexate: immunosuppressant
- TNF antagonists (e.g., etanercept, infliximab): most notable - block the key mediator. Not curative; patients must be maintained long-term. Risk of opportunistic infections (especially M. tuberculosis)
- Other biologics targeting T- and B-lymphocyte responses are also approved
Sources: Robbins & Kumar Basic Pathology (10e), p. 792 and Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 1106-1107
This is a shared conversation. Sign in to Orris to start your own chat.