Make MCQ of nclex level and advanced norcet level on topic Cardio pulmonary resuscitation with images based questions
CPR MCQ Bank - NCLEX & Advanced NORCET Level
SECTION A - NCLEX LEVEL (Questions 1-10)
Question 1 - Image-Based (Algorithm)
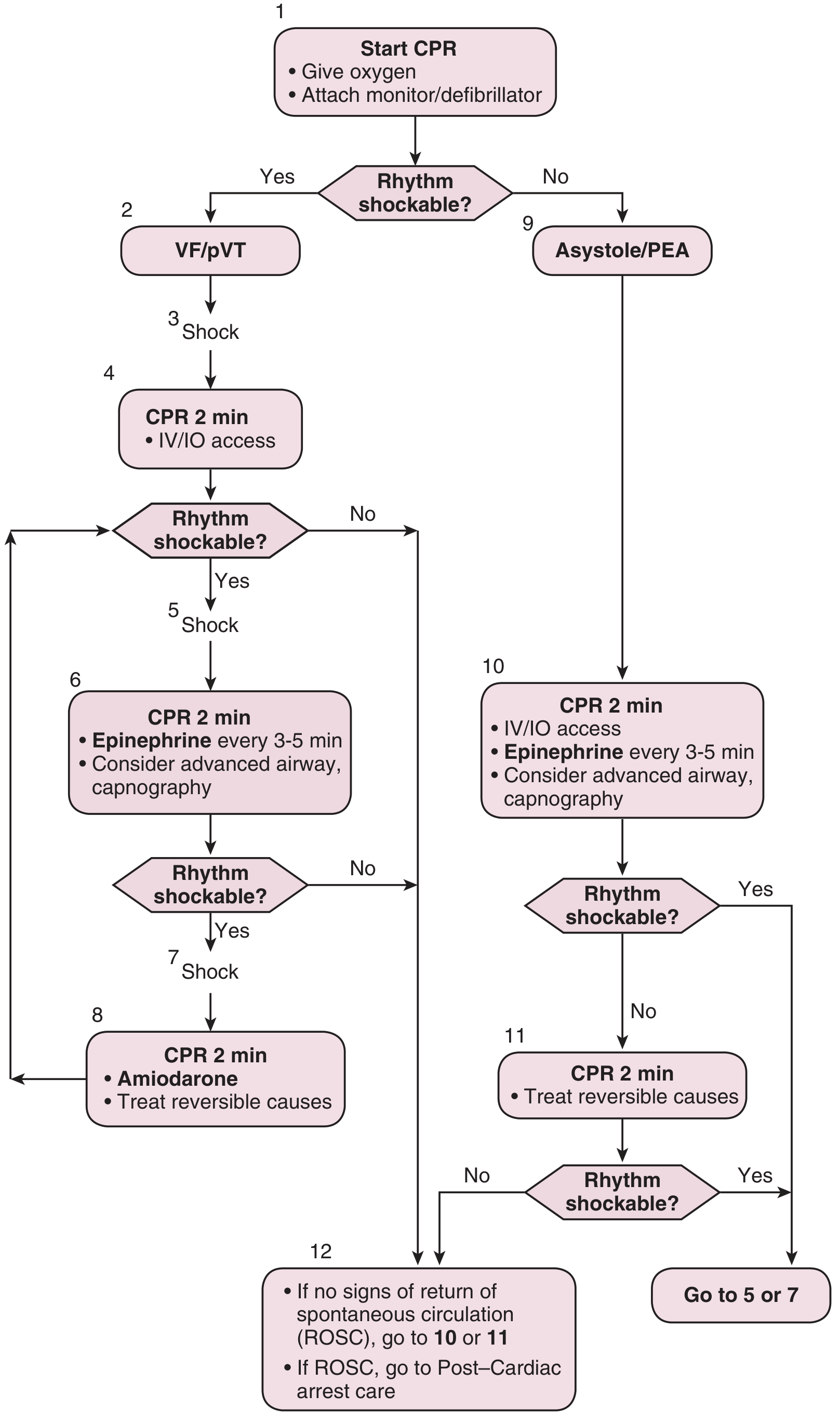
- A. Check pulse and assess rhythm immediately
- B. Administer epinephrine 1 mg IV/IO
- C. Resume CPR for 2 minutes and establish IV/IO access
- D. Administer amiodarone 300 mg IV
Rationale: Per the AHA algorithm (Step 4), after the first shock for VF/pVT, CPR is immediately resumed for 2 minutes while IV/IO access is obtained. Pulse check before the 2-minute CPR cycle is incorrect - rhythm/pulse checks are only done after the CPR cycle. Epinephrine is introduced in Step 6 (after the second shock) and amiodarone in Step 8 (after the third shock).
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
Question 2 - Clinical Scenario
- A. Rate of 80-100/min, depth of 1.5 inches
- B. Rate of 100-120/min, depth of 2.0-2.4 inches
- C. Rate of 120-140/min, depth of at least 3 inches
- D. Rate of 60-80/min, depth of 2.5 inches
Rationale: AHA guidelines specify compressing the sternum to a depth of 2.0-2.4 inches at a rate of 100-120 compressions/min. Compressing too fast (>120/min) reduces depth and prevents full chest recoil. Compressing too slowly reduces cardiac output. The 50:50 compression-to-relaxation ratio must be maintained.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 392
Question 3 - Priority Question
- A. Defibrillate immediately
- B. Administer amiodarone 300 mg IV
- C. Administer epinephrine 1 mg IV/IO every 3-5 minutes
- D. Prepare for synchronized cardioversion
Rationale: PEA is a non-shockable rhythm - defibrillation is NOT indicated. Amiodarone is used for refractory shockable rhythms (VF/pVT). Per the algorithm (right side, Step 10), PEA/Asystole management includes CPR, IV/IO access, and epinephrine every 3-5 minutes. Synchronized cardioversion is contraindicated in pulseless patients.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
Question 4 - Image Interpretation
- A. Lidocaine 1.5 mg/kg
- B. Vasopressin 40 units IV
- C. Magnesium sulfate 2g IV
- D. Amiodarone 300 mg IV
Rationale: Step 8 of the AHA algorithm introduces amiodarone for refractory VF/pVT after the third shock. Amiodarone (300 mg IV, second dose 150 mg) is the antiarrhythmic of choice. While lidocaine is an alternative, amiodarone is the first-line per AHA. Only two drugs are currently recommended for cardiac arrest - epinephrine and amiodarone - and no ACLS drug has been proven to improve long-term survival.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 313
Question 5 - Select All That Apply (NCLEX-style)
- A. Allow full chest recoil between compressions
- B. Stop compressions to deliver medications IV
- C. Rotate rescuers every 2-3 minutes
- D. Keep pauses in compressions to a minimum
- E. Compress to a depth of 1.5 inches
- F. Avoid leaning on the chest between compressions
Rationale:
- (A) Full chest recoil allows blood to re-enter the heart from the vena cava - essential for adequate ventricular filling.
- (C) Rotating rescuers every 2-3 minutes prevents fatigue-related decline in compression quality.
- (D) Minimizing pauses is critical - even short pauses profoundly reduce coronary perfusion pressure.
- (F) Not leaning prevents compression of the chest between compressions, restoring venous return.
- (B) is WRONG - medications can and should be given during compressions to avoid interruptions.
- (E) is WRONG - depth must be 2.0-2.4 inches, not 1.5.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
Question 6 - Clinical Scenario
- A. Mouth-to-mouth ventilation only
- B. 30 compressions : 2 breaths ratio
- C. Chest compression-only CPR (hands-only CPR)
- D. 15 compressions : 2 breaths ratio
Rationale: Chest compression-only CPR (CC-CPR/Hands-Only CPR) is endorsed by AHA for untrained lay bystanders. Studies show CC-CPR is as effective as standard CPR for witnessed adult cardiac arrest. In Arizona, switching to this approach increased bystander CPR rates from 28% to 40% and survival improved from 7.8% to 13.3%. The AHA shifted from "ABC" to "CAB" (Compressions, Airway, Breathing) since 2010, with emphasis on high-quality chest compressions.
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e
Question 7 - Pharmacology
- A. Increases myocardial contractility by beta-1 stimulation
- B. Causes coronary and cerebral vasodilation
- C. Alpha-1-mediated systemic vasoconstriction increases coronary perfusion pressure
- D. Directly converts VF to sinus rhythm
Rationale: Epinephrine's primary beneficial effect in cardiac arrest is through alpha-1 adrenergic receptor stimulation, causing peripheral vasoconstriction. This increases aortic diastolic pressure, which drives coronary perfusion pressure (the gradient that perfuses the heart during CPR diastole). Notably, concerns have been raised that epinephrine may worsen neurologic outcomes due to cerebral vasoconstriction, which is why it remains controversial. Epinephrine does NOT directly defibrillate.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 313
Question 8 - AED Scenario
- A. Check for a pulse and if absent, defibrillate manually
- B. Immediately resume CPR for 2 minutes
- C. Administer epinephrine and wait for the next rhythm analysis
- D. Intubate the patient immediately
Rationale: "No shock advised" on an AED indicates a non-shockable rhythm (PEA or asystole). The correct response is to immediately resume CPR. Defibrillation is only indicated for shockable rhythms (VF/pulseless VT). The survival rate drops 7-10% per minute without defibrillation when VF is present, but defibrillating asystole or PEA provides no benefit and may harm.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
Question 9 - Pediatric CPR
- A. 30:2
- B. 15:2
- C. 5:1
- D. 30:1
Rationale: For pediatric CPR with two rescuers, the ratio is 15:2 (15 compressions : 2 breaths). For a single rescuer performing CPR on a child, the ratio is 30:2 (same as adults). For infants, two-finger compression or the thumb-encircling technique is used. This differs from adult CPR where 30:2 applies regardless of rescuer number.
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e
Question 10 - Post-Arrest Care
- A. Immediate coronary angiography regardless of ECG findings
- B. Maintain MAP >65 mmHg and SBP >90 mmHg
- C. Administer high-dose corticosteroids to reduce cerebral edema
- D. Hyperventilate to reduce cerebral CO2
Rationale: Post-ROSC hemodynamic stabilization is the immediate priority. Hypotension (MAP <65, SBP <90) dramatically reduces cerebral blood flow and causes secondary brain injury - especially dangerous because cerebral autoregulation is often lost after cardiac arrest. Current recommendations target MAP >65 mmHg and SBP >90 mmHg using IV fluids and vasopressors as needed. Hyperventilation is harmful as it causes cerebral vasoconstriction and reduces CBF.
- ROSEN's Emergency Medicine, p. 71
SECTION B - ADVANCED NORCET LEVEL (Questions 11-20)
Question 11 - Advanced Algorithm (Image-Based)
- A. Ventricular fibrillation
- B. Return of spontaneous circulation (ROSC)
- C. Pulseless electrical activity
- D. Worsening cerebral ischemia
Rationale: A sharp increase in ETCO2 (usually >25-30 mmHg) during CPR is a reliable indicator of ROSC. When cardiac output is restored, CO2 that accumulated in tissues during the low-flow state is rapidly transported to the lungs and exhaled, causing a sudden spike in PETCO2. ETCO2 is used as a real-time CPR quality monitor - values <10 mmHg during CPR predict poor outcomes and may indicate futility.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
Question 12 - Pathophysiology (Image-Based)
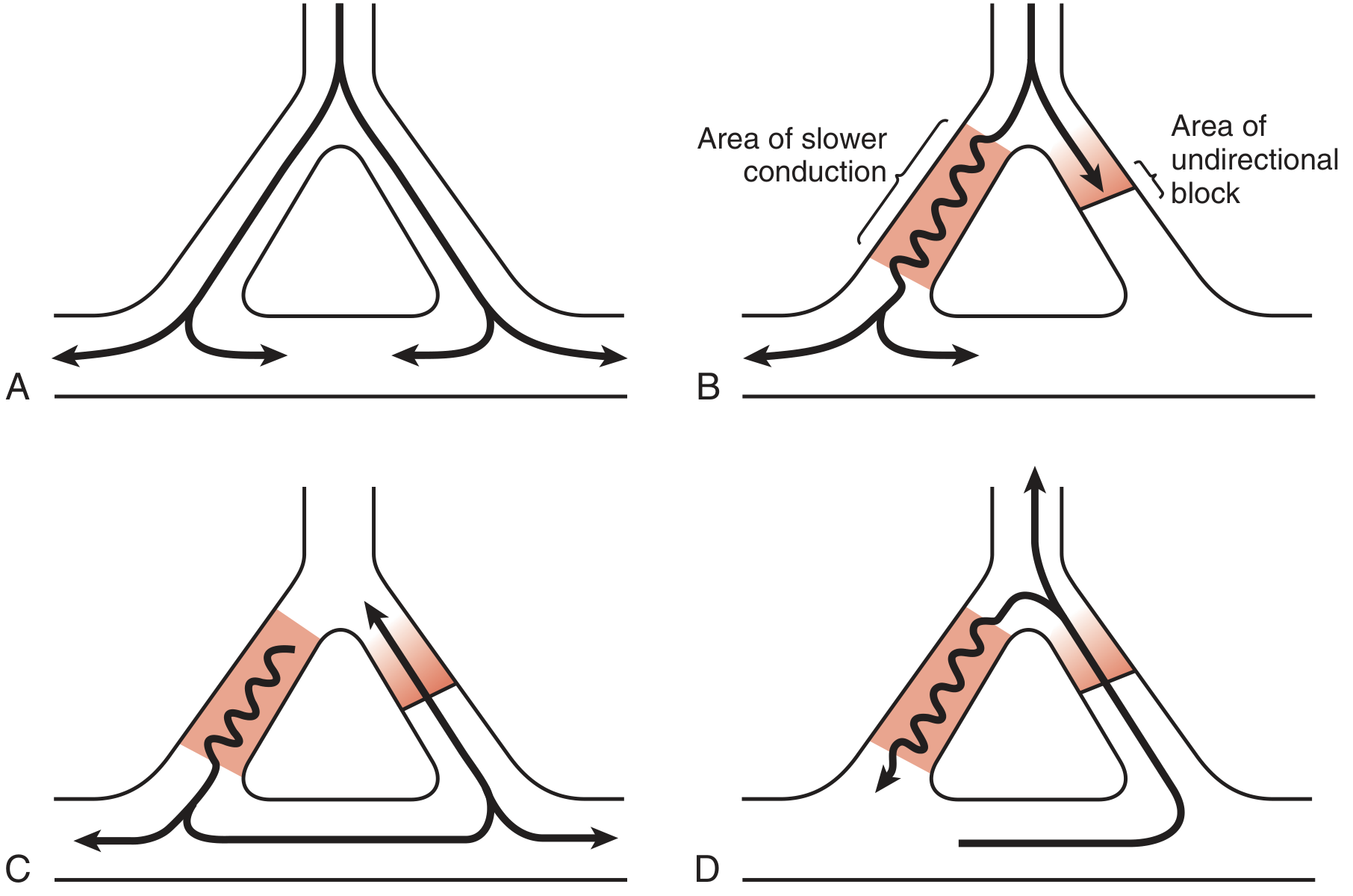
- A. Complete heart block
- B. Ventricular fibrillation (VF)
- C. Sinus bradycardia
- D. Junctional escape rhythm
Rationale: The diagram shows reentry: Panel A shows normal dual-pathway conduction; Panel B shows one pathway with slow conduction and another with unidirectional block; Panel C shows antegrade conduction looping around; Panel D shows the completed reentry circuit. Reentry is the primary electrophysiologic mechanism behind VF and pulseless VT - the most common shockable rhythms in sudden cardiac arrest (SCA). During VF, myocytes consume oxygen and ATP at the same or higher rate than during normal contraction.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 310
Question 13 - Advanced Pharmacology
- A. Epinephrine consistently improves both ROSC and long-term neurologic outcomes
- B. Epinephrine improves ROSC rates but may worsen neurologic outcomes via cerebral vasoconstriction
- C. Epinephrine has been removed from ACLS guidelines due to harm
- D. Epinephrine 0.2 mg IV is the current recommended dose every 5-10 minutes
Rationale: Only epinephrine and amiodarone are currently recommended ACLS drugs, but neither has proven long-term survival benefit. More critically, epinephrine is associated with worsened final outcomes, possibly through prolonged cerebral vasoconstriction - a clinically significant finding that has prompted debate. The recommended dose remains 1 mg IV/IO every 3-5 minutes. This represents a major controversy in resuscitation medicine.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 313
Question 14 - Team Leadership & Resuscitation
- A. The team leader should always perform defibrillation, not compressions
- B. The team leader performing compressions compromises their ability to monitor rhythm, direct drug administration, and maintain overall control of the resuscitation
- C. Only physicians are permitted to perform chest compressions
- D. The team leader should exclusively manage the airway
Rationale: The team leader's role is to oversee and direct - not to perform tasks. They must monitor rhythm, order initiation/termination of compressions, direct drug delivery, observe CPR quality, and order rescuer rotations. If the team leader is physically performing compressions, they lose situational awareness and overall control of the resuscitation rapidly deteriorates. Per guidelines, the team leader should stand where they can direct the entire resuscitation.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 394
Question 15 - ACLS Drug Sequencing
- A. Repeat 300 mg IV bolus
- B. 150 mg IV (second dose)
- C. 360 mg IV (loading dose)
- D. Switch to lidocaine 1 mg/kg IV
Rationale: The AHA ACLS protocol for amiodarone in refractory VF/pulseless VT is:
- First dose: 300 mg IV/IO
- Second dose: 150 mg IV/IO If amiodarone is unavailable, lidocaine is an acceptable alternative. The sequential dosing prevents toxicity from excessive cumulative doses (amiodarone can cause hypotension, bradycardia).
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
Question 16 - Advanced Pathophysiology
- A. Are in a resting state with minimal oxygen demand
- B. Consume oxygen and ATP at the same or higher rate than during normal contraction
- C. Receive adequate perfusion through retrograde coronary flow
- D. Stop all electrical activity completely
Rationale: This is a critical concept. During VF, despite disorganized contraction, myocytes are electrically active and metabolically consuming O2 and ATP at rates equal to or exceeding normal contraction. This explains why CPR quality (washing out ischemic metabolic byproducts, maintaining coronary perfusion) directly affects defibrillation success - a metabolically "exhausted" myocardium is refractory to defibrillation. Shallow compressions fail to clear these byproducts.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 310
Question 17 - LVAD/Device Scenario
- A. CPR is absolutely contraindicated in LVAD patients
- B. Standard ACLS algorithms should be followed; peripheral pulses may be absent even with LVAD functioning
- C. External defibrillation cannot be used in LVAD patients
- D. The LVAD provides adequate perfusion so CPR is unnecessary
Rationale: LVAD patients present unique challenges - the absence of peripheral pulses is normal even with the device functioning (continuous flow). In arrest, standard ACLS algorithms are followed. Verify the machine is connected, battery is charged, and it has an audible hum. External defibrillation can be used (pads placed >10 cm from device in anteroposterior configuration, lowest effective energy). Standard CPR may potentially dislodge the device (a concern), but ACLS should not be withheld.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 335-336
Question 18 - Survival Statistics & Decision Making
- A. 10-20% reduction
- B. 40-50% reduction
- C. 56-80% reduction
- D. 5-10% reduction
Rationale: Survival from VF/SCA drops 7-10% for every minute without treatment (no CPR, no defibrillation). At 8 minutes: 8 × 7% = 56% to 8 × 10% = 80% reduction. If CPR is initiated, the decline slows to 3-4%/minute. This underscores why immediate bystander CPR and early defibrillation are critical. Immediate CPR + defibrillation has been shown to increase survival up to fourfold in witnessed VF arrest.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 4197
Question 19 - Defibrillator Management (Advanced)
- A. Stop CPR immediately - the AICD will terminate the arrhythmia
- B. Continue CPR; the shocks are harmless to rescuers; if the shocks impede CPR performance, apply a magnet over the device corner to disable it
- C. Defibrillate immediately with pads placed directly over the AICD
- D. Administer lidocaine to suppress AICD discharge
Rationale: AICD shocks during CPR are harmless to rescuers (low current density at the rescuer's hands). CPR should continue. If AICD shocks are impeding CPR performance OR if SVT occurs during resuscitation, the AICD can be disabled by placing a magnet over the corner of the device from which leads emerge (pause until AICD activity ceases). External defibrillation pads must be placed >10 cm from the pulse generator - never directly over it. Anteroposterior pad placement is preferred.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 335
Question 20 - Critical Thinking (Highest Level NORCET)
- A. Cooling to 33°C is definitively superior to 36°C for neurologic outcomes
- B. TTM at 36°C versus 33°C showed no significant difference in outcomes in landmark RCTs; fever prevention remains the core goal
- C. TTM is contraindicated in patients with prolonged downtime >15 minutes
- D. TTM must be started within 1 hour of ROSC for any benefit
Rationale: The TTM Trial (2013, NEJM) randomized 950 patients to 33°C vs 36°C and found no significant difference in mortality or neurologic outcomes. A subsequent trial (Dankiewicz et al., TTM2, NEJM 2021) found normothermia (avoiding fever >37.8°C) was non-inferior to hypothermia at 33°C. Current practice therefore focuses on fever prevention post-ROSC rather than mandatory deep cooling. However, active fever treatment and neurological monitoring remain standard of care. TTM is not absolutely contraindicated by downtime alone.
- ROSEN's Emergency Medicine; Miller's Anesthesia, 10e
Summary Table
| Q# | Level | Topic | Key Teaching Point |
|---|---|---|---|
| 1 | NCLEX | Algorithm-based | After shock for VF → CPR 2 min immediately |
| 2 | NCLEX | Compression quality | 100-120/min, 2.0-2.4 inch depth |
| 3 | NCLEX | PEA management | Non-shockable → epinephrine, not defibrillation |
| 4 | NCLEX | Drug sequencing | Amiodarone at Step 8 (3rd shock cycle) |
| 5 | NCLEX | High-quality CPR (SATA) | Full recoil, rotate rescuers, minimize pauses |
| 6 | NCLEX | Bystander CPR | Hands-only CPR for untrained laypeople |
| 7 | NCLEX | Epinephrine mechanism | Alpha-1 vasoconstriction → coronary perfusion |
| 8 | NCLEX | AED no-shock | Resume CPR immediately for non-shockable |
| 9 | NCLEX | Pediatric CPR | 2-rescuer child = 15:2 ratio |
| 10 | NCLEX | Post-ROSC care | MAP >65, SBP >90; avoid hypotension |
| 11 | NORCET | ETCO2 | Sharp ETCO2 rise = ROSC indicator |
| 12 | NORCET | Reentry diagram | Reentry → VF/pVT mechanism |
| 13 | NORCET | Advanced pharmacology | Epinephrine: ROSC ↑ but neurologic outcome ? |
| 14 | NORCET | Team leadership | Leader must NOT perform compressions |
| 15 | NORCET | Amiodarone dosing | 300 mg → 150 mg second dose |
| 16 | NORCET | VF physiology | Myocytes consume ATP at full rate in VF |
| 17 | NORCET | LVAD arrest | Standard ACLS; no pulses ≠ arrest in LVAD |
| 18 | NORCET | Survival statistics | 7-10%/min survival loss without CPR |
| 19 | NORCET | AICD during CPR | Shocks harmless; magnet to disable if needed |
| 20 | NORCET | TTM evidence | 33°C = 36°C; fever prevention is key goal |
- Roberts and Hedges' Clinical Procedures in Emergency Medicine (Roberts & Hedges)
- ROSEN's Emergency Medicine: Concepts and Clinical Practice
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9th ed.
- Miller's Anesthesia, 10th ed.
- AHA 2015 ACLS Guidelines; TTM Trial (Nielsen et al., NEJM 2013); TTM2 Trial (Dankiewicz et al., NEJM 2021)
Generate a quick reference poster comparing pediatric vs adult CPR parameters
A professional medical quick reference poster titled "CPR Parameters: Adult vs Pediatric" with a clean clinical design. The poster is divided into two main columns - left side for ADULT CPR (blue color scheme) and right side for PEDIATRIC CPR (green color scheme), with a header row. Include the following data in a clear comparison table format: HEADER: "CPR QUICK REFERENCE GUIDE — Adult vs Pediatric" with a red heart icon and "Based on AHA Guidelines" subtitle ADULT CPR column (blue): - Age: ≥8 years / Pubescent - Compression Rate: 100–120 / min - Compression Depth: 2.0–2.4 inches (5–6 cm) - Compression:Ventilation Ratio (1 rescuer): 30:2 - Compression:Ventilation Ratio (2 rescuers): 30:2 - Hand Position: 2 hands — heel of hand on lower half of sternum - Chest Recoil: Full recoil between compressions - Defibrillation Energy (biphasic): 200 J (device-specific) - Defibrillation Energy (monophasic): 360 J - Epinephrine Dose: 1 mg IV/IO every 3–5 min - Airway: Head-tilt chin-lift or jaw thrust - Sequence: C–A–B (Compressions first) PEDIATRIC CPR column (green): - Age: 1–8 years (child) / <1 year (infant) - Compression Rate: 100–120 / min - Compression Depth: Child: 2 inches (5 cm) / Infant: 1.5 inches (4 cm) - Compression:Ventilation Ratio (1 rescuer): 30:2 - Compression:Ventilation Ratio (2 rescuers): 15:2 - Hand Position: Child: 1–2 hands on lower sternum / Infant: 2 fingers or 2-thumb encircling - Chest Recoil: Full recoil between compressions - Defibrillation Energy: 2 J/kg first shock → 4 J/kg subsequent - Epinephrine Dose: 0.01 mg/kg IV/IO (max 1 mg) every 3–5 min - Airway: Neutral position for infants, slight sniff for children - Sequence: C–A–B (Compressions first) At the bottom, include a UNIVERSAL PRINCIPLES section in a yellow/amber banner: "Minimize interruptions • Full chest recoil • Avoid hyperventilation • Switch compressors every 2 min • High-quality compressions save lives" Also add a small KEY DIFFERENCES box highlighting: "2-rescuer pediatric ratio changes to 15:2 | Infant: 2-finger or thumb-encircling technique | Peds defib dose is weight-based (J/kg)" Design should be clean, modern, clinical, high-contrast, suitable for hospital wall display. Use bold fonts for numbers, color-coded sections, icons for each parameter where possible.
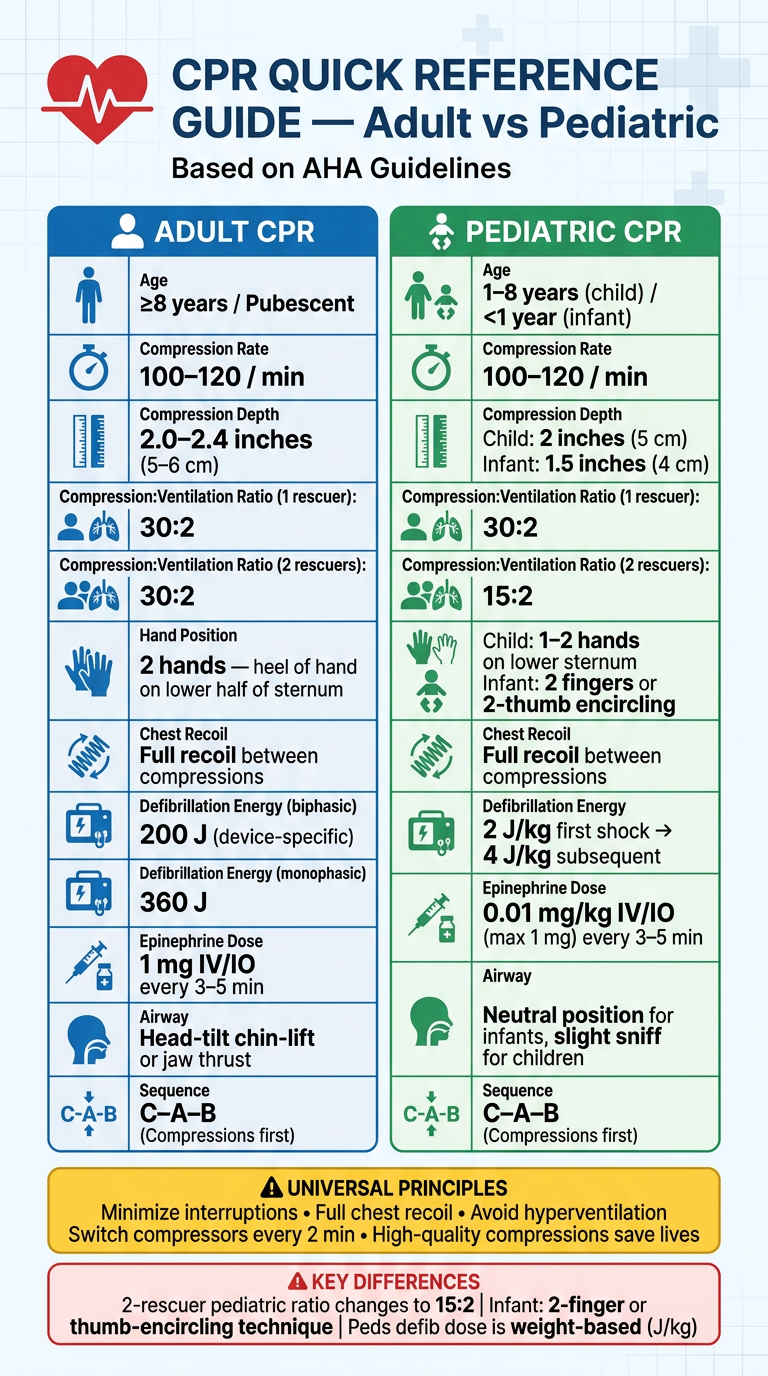
| Parameter | Adult | Child (1-8 yrs) | Infant (<1 yr) |
|---|---|---|---|
| Compression Rate | 100-120/min | 100-120/min | 100-120/min |
| Compression Depth | 2.0-2.4 inches | ~2 inches | ~1.5 inches |
| C:V Ratio (1 rescuer) | 30:2 | 30:2 | 30:2 |
| C:V Ratio (2 rescuers) | 30:2 | 15:2 | 15:2 |
| Hand Technique | 2 hands | 1-2 hands | 2 fingers / thumb-encircling |
| Defib Energy | 200 J biphasic | 2 J/kg → 4 J/kg | 2 J/kg → 4 J/kg |
| Epinephrine | 1 mg IV/IO q3-5 min | 0.01 mg/kg IV/IO | 0.01 mg/kg IV/IO |
- 2-rescuer pediatric CPR uses 15:2, not 30:2
- Infant compression technique - 2-finger or thumb-encircling method
- Pediatric defibrillation is weight-based (2 J/kg first, 4 J/kg after)
Generate clinical scenario cards for pediatric vs adult arrest decisions
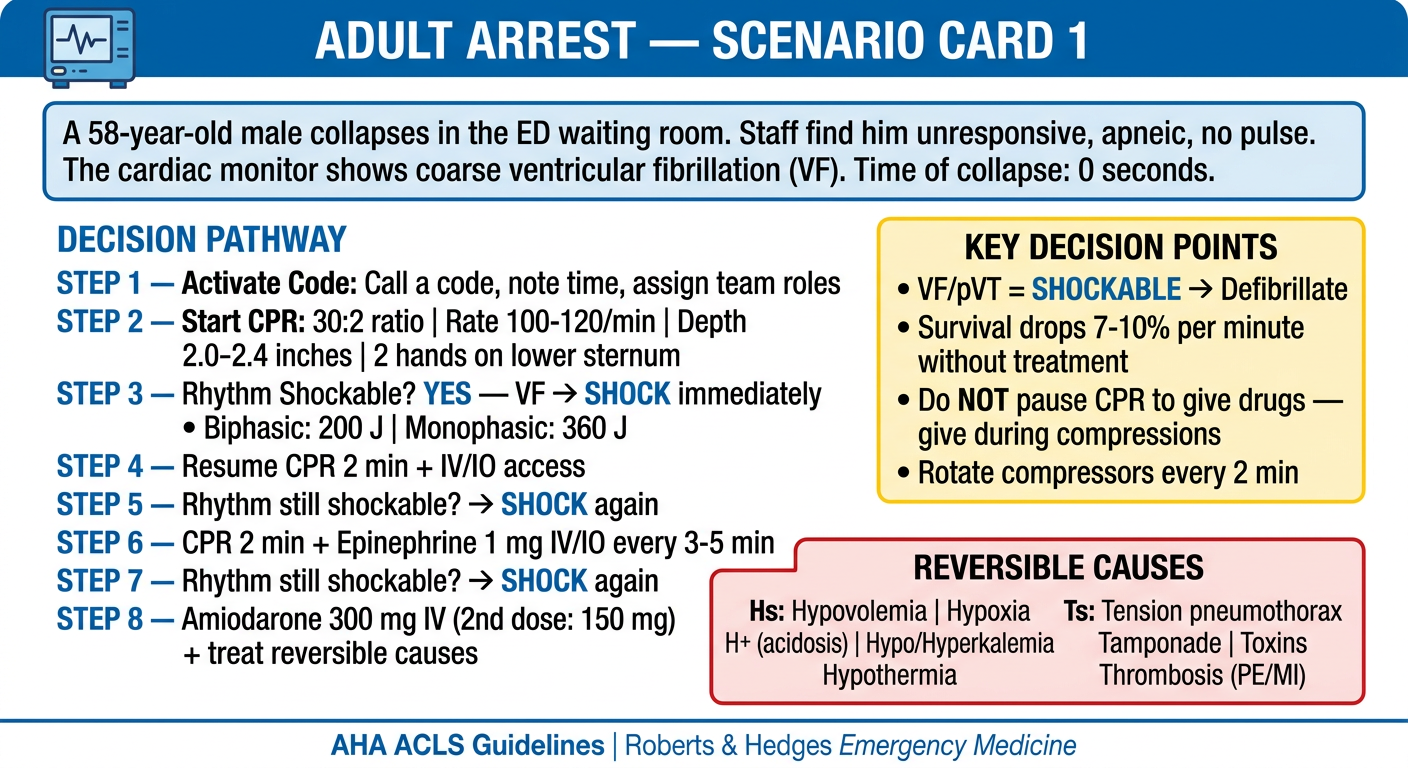
A professional medical clinical scenario flashcard. Design: clean white background with a bold blue header bar. Title at top: "ADULT ARREST — SCENARIO CARD 1" with a small blue cardiac monitor icon. SCENARIO BOX (light blue background): "A 58-year-old male collapses in the ED waiting room. Staff find him unresponsive, apneic, no pulse. The cardiac monitor shows coarse ventricular fibrillation (VF). Time of collapse: 0 seconds." DECISION PATHWAY section (structured step-by-step): STEP 1 — Activate Code: Call a code, note time, assign team roles STEP 2 — Start CPR: 30:2 ratio | Rate 100-120/min | Depth 2.0-2.4 inches | 2 hands on lower sternum STEP 3 — Rhythm Shockable? YES — VF → SHOCK immediately • Biphasic: 200 J | Monophasic: 360 J STEP 4 — Resume CPR 2 min + IV/IO access STEP 5 — Rhythm still shockable? → SHOCK again STEP 6 — CPR 2 min + Epinephrine 1 mg IV/IO every 3-5 min STEP 7 — Rhythm still shockable? → SHOCK again STEP 8 — Amiodarone 300 mg IV (2nd dose: 150 mg) + treat reversible causes KEY DECISION POINTS box (yellow): • VF/pVT = SHOCKABLE → Defibrillate • Survival drops 7-10% per minute without treatment • Do NOT pause CPR to give drugs — give during compressions • Rotate compressors every 2 min REVERSIBLE CAUSES box (red border, 2 columns): Hs: Hypovolemia | Hypoxia | H+ (acidosis) | Hypo/Hyperkalemia | Hypothermia Ts: Tension pneumothorax | Tamponade | Toxins | Thrombosis (PE/MI) Footer: "AHA ACLS Guidelines | Roberts & Hedges Emergency Medicine" Color scheme: Blue and white, professional medical style, bold fonts for key numbers
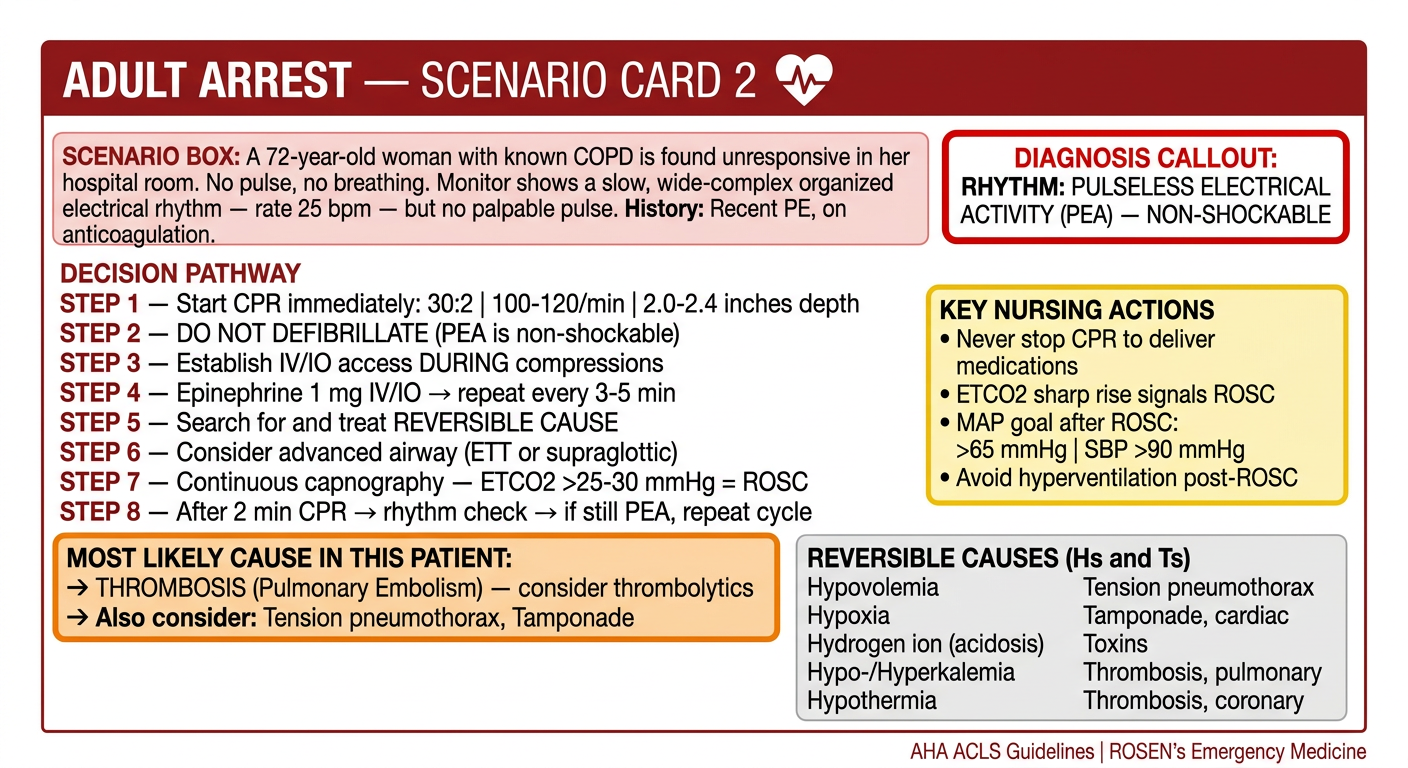
A professional medical clinical scenario flashcard. Design: clean white background with a bold dark red header bar. Title at top: "ADULT ARREST — SCENARIO CARD 2" with a cardiac icon. SCENARIO BOX (light red/pink background): "A 72-year-old woman with known COPD is found unresponsive in her hospital room. No pulse, no breathing. Monitor shows a slow, wide-complex organized electrical rhythm — rate 25 bpm — but no palpable pulse. History: Recent PE, on anticoagulation." DIAGNOSIS CALLOUT (bold red border): "RHYTHM: PULSELESS ELECTRICAL ACTIVITY (PEA) — NON-SHOCKABLE" DECISION PATHWAY section: STEP 1 — Start CPR immediately: 30:2 | 100-120/min | 2.0-2.4 inches depth STEP 2 — DO NOT DEFIBRILLATE (PEA is non-shockable) STEP 3 — Establish IV/IO access DURING compressions STEP 4 — Epinephrine 1 mg IV/IO → repeat every 3-5 min STEP 5 — Search for and treat REVERSIBLE CAUSE STEP 6 — Consider advanced airway (ETT or supraglottic) STEP 7 — Continuous capnography — ETCO2 >25-30 mmHg = ROSC STEP 8 — After 2 min CPR → rhythm check → if still PEA, repeat cycle MOST LIKELY CAUSE IN THIS PATIENT (highlighted orange box): → THROMBOSIS (Pulmonary Embolism) — consider thrombolytics → Also consider: Tension pneumothorax, Tamponade KEY NURSING ACTIONS box (yellow): • Never stop CPR to deliver medications • ETCO2 sharp rise signals ROSC • MAP goal after ROSC: >65 mmHg | SBP >90 mmHg • Avoid hyperventilation post-ROSC REVERSIBLE CAUSES (Hs and Ts listed in 2 neat columns) Footer: "AHA ACLS Guidelines | ROSEN's Emergency Medicine" Color scheme: Red/maroon and white, professional clinical style
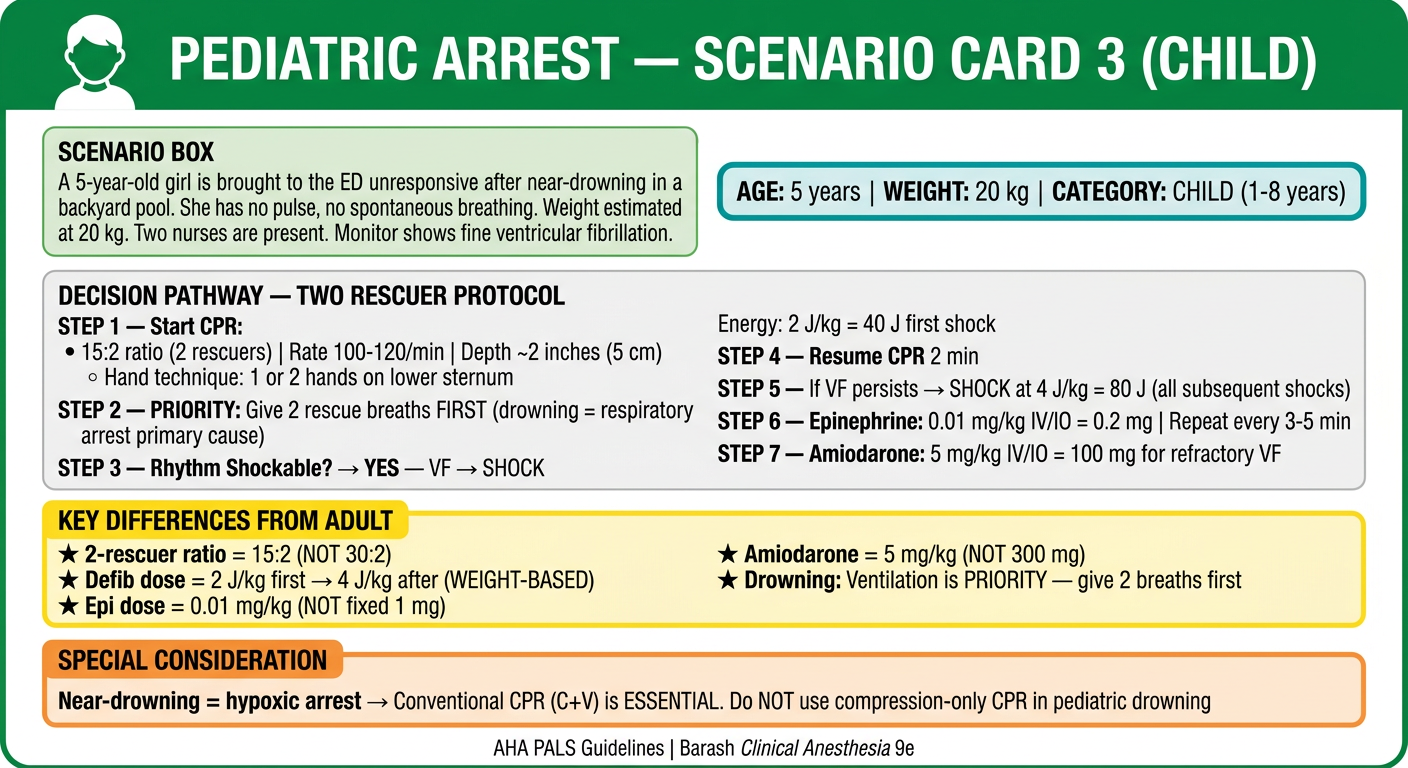
A professional medical clinical scenario flashcard for pediatric emergency. Design: clean white background with a bold green header bar. Title at top: "PEDIATRIC ARREST — SCENARIO CARD 3 (CHILD)" with a child silhouette icon. SCENARIO BOX (light green background): "A 5-year-old girl is brought to the ED unresponsive after near-drowning in a backyard pool. She has no pulse, no spontaneous breathing. Weight estimated at 20 kg. Two nurses are present. Monitor shows fine ventricular fibrillation." AGE/WEIGHT CALLOUT box (teal): "AGE: 5 years | WEIGHT: 20 kg | CATEGORY: CHILD (1-8 years)" DECISION PATHWAY — TWO RESCUER PROTOCOL: STEP 1 — Start CPR: 15:2 ratio (2 rescuers) | Rate 100-120/min | Depth ~2 inches (5 cm) Hand technique: 1 or 2 hands on lower sternum STEP 2 — PRIORITY: Give 2 rescue breaths FIRST (drowning = respiratory arrest primary cause) STEP 3 — Rhythm Shockable? YES — VF → SHOCK Energy: 2 J/kg = 40 J first shock STEP 4 — Resume CPR 2 min STEP 5 — If VF persists → SHOCK at 4 J/kg = 80 J (all subsequent shocks) STEP 6 — Epinephrine: 0.01 mg/kg IV/IO = 0.2 mg | Repeat every 3-5 min STEP 7 — Amiodarone: 5 mg/kg IV/IO = 100 mg for refractory VF KEY DIFFERENCES FROM ADULT (highlighted yellow box with bold text): ★ 2-rescuer ratio = 15:2 (NOT 30:2) ★ Defib dose = 2 J/kg first → 4 J/kg after (WEIGHT-BASED) ★ Epi dose = 0.01 mg/kg (NOT fixed 1 mg) ★ Amiodarone = 5 mg/kg (NOT 300 mg) ★ Drowning: Ventilation is PRIORITY — give 2 breaths first SPECIAL CONSIDERATION (orange box): Near-drowning = hypoxic arrest → Conventional CPR (C+V) is ESSENTIAL Do NOT use compression-only CPR in pediatric drowning Footer: "AHA PALS Guidelines | Barash Clinical Anesthesia 9e" Color scheme: Green and white, child-focused clinical style, warm and clear
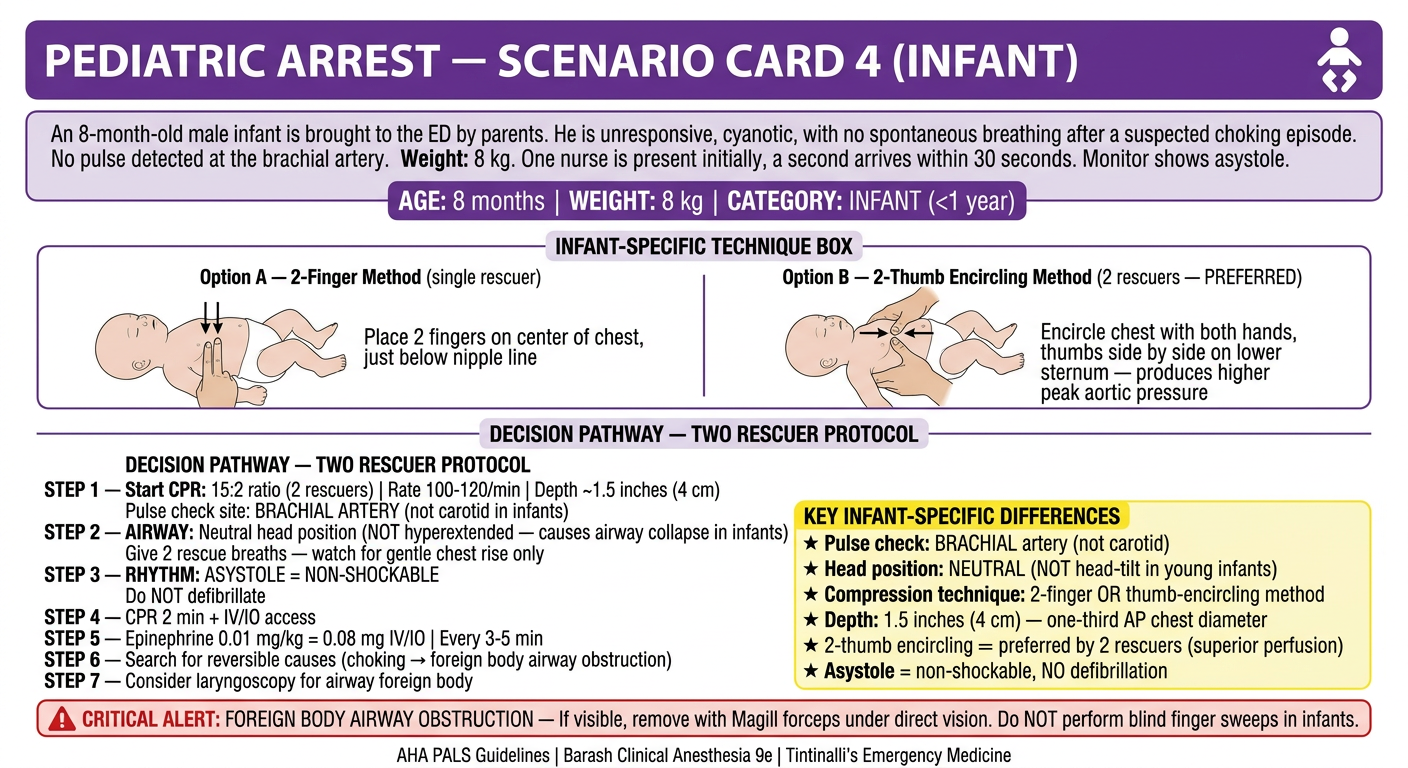
A professional medical clinical scenario flashcard for pediatric emergency. Design: clean white background with a bold purple header bar. Title at top: "PEDIATRIC ARREST — SCENARIO CARD 4 (INFANT)" with a baby/infant silhouette icon. SCENARIO BOX (light lavender background): "An 8-month-old male infant is brought to the ED by parents. He is unresponsive, cyanotic, with no spontaneous breathing after a suspected choking episode. No pulse detected at the brachial artery. Weight: 8 kg. One nurse is present initially, a second arrives within 30 seconds. Monitor shows asystole." AGE/WEIGHT CALLOUT box (purple): "AGE: 8 months | WEIGHT: 8 kg | CATEGORY: INFANT (<1 year)" INFANT-SPECIFIC TECHNIQUE BOX (with diagram description): COMPRESSION TECHNIQUE OPTIONS: Option A — 2-Finger Method (single rescuer): Place 2 fingers on center of chest, just below nipple line Option B — 2-Thumb Encircling Method (2 rescuers — PREFERRED): Encircle chest with both hands, thumbs side by side on lower sternum — produces higher peak aortic pressure DECISION PATHWAY — TWO RESCUER PROTOCOL: STEP 1 — Start CPR: 15:2 ratio (2 rescuers) | Rate 100-120/min | Depth ~1.5 inches (4 cm) Pulse check site: BRACHIAL ARTERY (not carotid in infants) STEP 2 — AIRWAY: Neutral head position (NOT hyperextended — causes airway collapse in infants) Give 2 rescue breaths — watch for gentle chest rise only STEP 3 — RHYTHM: ASYSTOLE = NON-SHOCKABLE Do NOT defibrillate STEP 4 — CPR 2 min + IV/IO access STEP 5 — Epinephrine 0.01 mg/kg = 0.08 mg IV/IO | Every 3-5 min STEP 6 — Search for reversible causes (choking → foreign body airway obstruction) STEP 7 — Consider laryngoscopy for airway foreign body KEY INFANT-SPECIFIC DIFFERENCES (yellow highlighted box): ★ Pulse check: BRACHIAL artery (not carotid) ★ Head position: NEUTRAL (NOT head-tilt in young infants) ★ Compression technique: 2-finger OR thumb-encircling method ★ Depth: 1.5 inches (4 cm) — one-third AP chest diameter ★ 2-thumb encircling = preferred by 2 rescuers (superior perfusion) ★ Asystole = non-shockable, NO defibrillation CRITICAL ALERT (red box): "FOREIGN BODY AIRWAY OBSTRUCTION — If visible, remove with Magill forceps under direct vision. Do NOT perform blind finger sweeps in infants." Footer: "AHA PALS Guidelines | Barash Clinical Anesthesia 9e | Tintinalli's Emergency Medicine" Color scheme: Purple and white, clinical infant care style, clear bold fonts
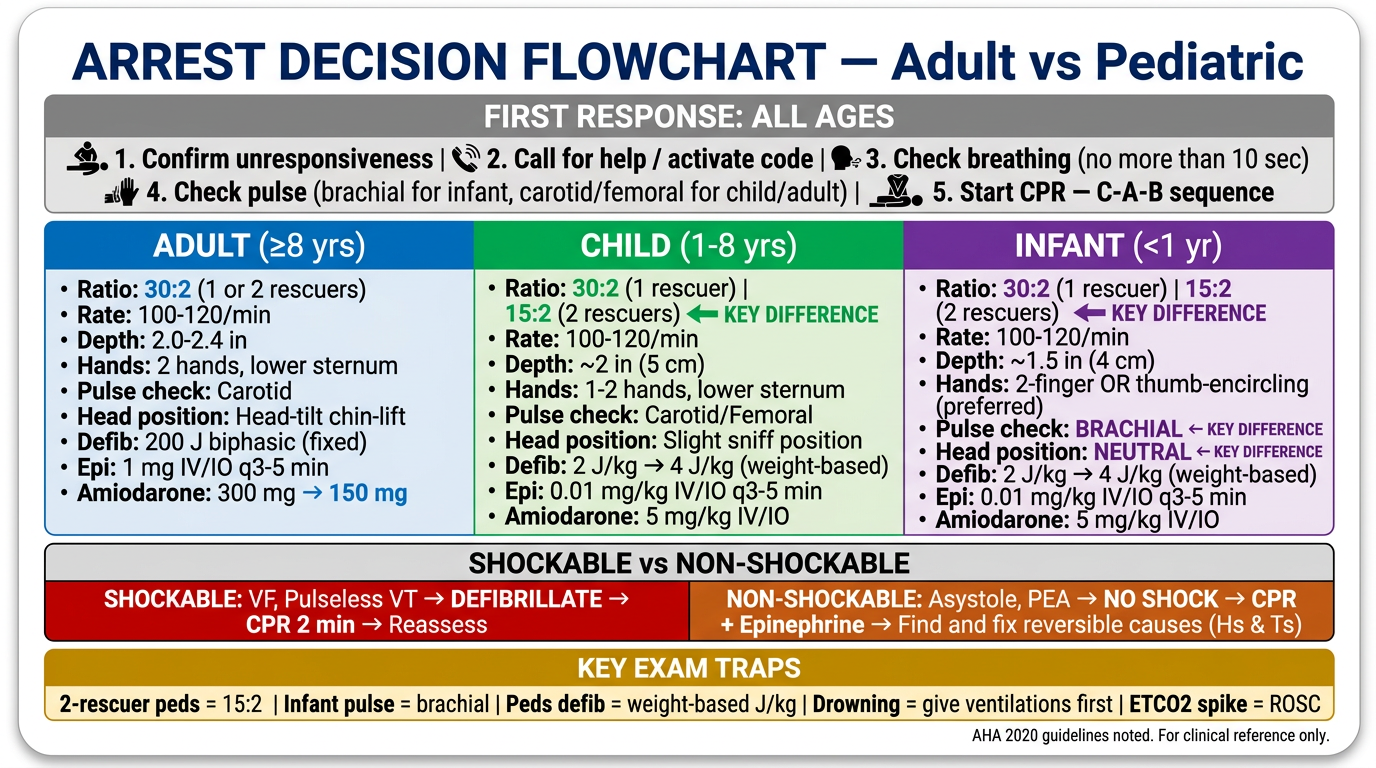
A professional medical quick-decision summary card titled "ARREST DECISION FLOWCHART — Adult vs Pediatric" designed as a clinical reference tool for nurses and emergency staff. Layout: landscape orientation, clean white background with color-coded sections. TOP SECTION — "FIRST RESPONSE: ALL AGES" (gray banner): 1. Confirm unresponsiveness | 2. Call for help / activate code | 3. Check breathing (no more than 10 sec) | 4. Check pulse (brachial for infant, carotid/femoral for child/adult) | 5. Start CPR — C-A-B sequence MIDDLE SECTION — 3-column comparison table with bold headers: Column 1 — ADULT (≥8 yrs) — Blue: • Ratio: 30:2 (1 or 2 rescuers) • Rate: 100-120/min • Depth: 2.0-2.4 in • Hands: 2 hands, lower sternum • Pulse check: Carotid • Head position: Head-tilt chin-lift • Defib: 200 J biphasic (fixed) • Epi: 1 mg IV/IO q3-5 min • Amiodarone: 300 mg → 150 mg Column 2 — CHILD (1-8 yrs) — Green: • Ratio: 30:2 (1 rescuer) | 15:2 (2 rescuers) ← KEY DIFFERENCE • Rate: 100-120/min • Depth: ~2 in (5 cm) • Hands: 1-2 hands, lower sternum • Pulse check: Carotid/Femoral • Head position: Slight sniff position • Defib: 2 J/kg → 4 J/kg (weight-based) • Epi: 0.01 mg/kg IV/IO q3-5 min • Amiodarone: 5 mg/kg IV/IO Column 3 — INFANT (<1 yr) — Purple: • Ratio: 30:2 (1 rescuer) | 15:2 (2 rescuers) ← KEY DIFFERENCE • Rate: 100-120/min • Depth: ~1.5 in (4 cm) • Hands: 2-finger OR thumb-encircling (preferred) • Pulse check: BRACHIAL ← KEY DIFFERENCE • Head position: NEUTRAL ← KEY DIFFERENCE • Defib: 2 J/kg → 4 J/kg (weight-based) • Epi: 0.01 mg/kg IV/IO q3-5 min • Amiodarone: 5 mg/kg IV/IO BOTTOM SECTION — "SHOCKABLE vs NON-SHOCKABLE" decision box (split red/orange): SHOCKABLE: VF, Pulseless VT → DEFIBRILLATE → CPR 2 min → Reassess NON-SHOCKABLE: Asystole, PEA → NO SHOCK → CPR + Epinephrine → Find and fix reversible causes (Hs & Ts) BOTTOM BANNER (amber/gold): "KEY EXAM TRAPS: 2-rescuer peds = 15:2 | Infant pulse = brachial | Peds defib = weight-based J/kg | Drowning = give ventilations first | ETCO2 spike = ROSC" Style: Bold, clinical, high contrast, suitable as a printed laminated reference card. AHA 2020 guidelines noted at footer.
Card 1 - Adult Arrest: Shockable Rhythm (VF)
Card 2 - Adult Arrest: Non-Shockable (PEA)
Card 3 - Pediatric Arrest: Child (Drowning/VF)
Card 4 - Pediatric Arrest: Infant (Asystole/Choking)
Bonus - Master Decision Reference Card
| Card | Key Clinical Decision |
|---|---|
| Adult VF | Shock → CPR 2 min → Epi → Amiodarone sequence |
| Adult PEA | No shock, Epi only, hunt for Hs & Ts, ETCO2 for ROSC |
| Child drowning | 15:2 (2 rescuers), ventilations first, weight-based defib (40 J) |
| Infant choking | Brachial pulse, neutral head, thumb-encircling, NO blind finger sweep |
| Master card | All 3 populations side by side + shockable vs non-shockable split |