Malaria and pulmonary disease Full details for md exams 15marks
Reading File
search_medical_text
malaria pulmonary complications acute lung injury ARDS pathophysiology
search_medical_text
severe malaria respiratory distress clinical features diagnosis management
search_medical_image
malaria pulmonary edema chest X-ray ARDS
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive, exam-ready answer on Malaria and Pulmonary Disease structured for a 15-mark MD examination.
Malaria and Pulmonary Disease
1. Introduction
Pulmonary complications are among the most serious manifestations of malaria, predominantly associated with Plasmodium falciparum (severe malaria) but also increasingly recognized in P. vivax infection. They range from mild respiratory distress to fulminant Acute Respiratory Distress Syndrome (ARDS) and are a leading cause of death in adults with severe malaria.
2. Types of Pulmonary Involvement
| Type | Description |
|---|---|
| Pulmonary edema (non-cardiogenic) | Most feared; ARDS-like picture |
| Acute Lung Injury (ALI) | Milder precursor to ARDS |
| Respiratory distress due to metabolic acidosis | Compensatory hyperpnoea without true lung disease |
| Aspiration pneumonia | Secondary to altered consciousness |
| Malarial pleural effusion | Uncommon |
| Concurrent bacterial pneumonia | Especially in endemic regions |
3. Epidemiology
- Pulmonary edema/ARDS occurs in ~3–10% of adults with severe falciparum malaria.
- Mortality in malaria-associated ARDS exceeds 80% in some series.
- P. vivax — historically considered benign — is now well-documented to cause ARDS (see CXR series below).
- Pregnant women and non-immune adults (travelers) are at highest risk.
4. Pathophysiology
A. Cytokine-Mediated Endothelial Injury
- Parasitized RBCs (pRBCs) express PfEMP1 (P. falciparum Erythrocyte Membrane Protein 1) on their surface.
- PfEMP1 mediates cytoadherence to pulmonary capillary endothelium via ICAM-1, CD36, and PECAM-1.
- Sequestration of pRBCs in pulmonary microvasculature causes:
- Microvascular obstruction
- Local hypoxia
- Endothelial activation
B. Inflammatory Cascade
- Massive release of TNF-α, IL-1, IL-6, IL-8, IFN-γ
- Neutrophil and monocyte activation → oxidative burst
- Reactive oxygen species (ROS) damage alveolar capillary membrane
- Increased microvascular permeability → non-cardiogenic pulmonary edema
C. Mechanical and Biochemical Factors
| Factor | Effect |
|---|---|
| Reduced RBC deformability | Plugging of pulmonary capillaries |
| Rosetting (pRBCs + uninfected RBCs) | Worsened microvascular obstruction |
| Hypoalbuminaemia | Reduced oncotic pressure → alveolar flooding |
| Fluid over-resuscitation | Precipitates or worsens pulmonary edema |
| Metabolic acidosis | Drives compensatory hyperventilation (Kussmaul breathing) |
| Severe anaemia | Exacerbates hypoxia |
D. ARDS Mechanism (Berlin Definition)
Malaria causes indirect ARDS (via systemic sepsis-like state):
- Diffuse alveolar damage (DAD)
- Hyaline membrane formation
- Alveolar collapse and consolidation
- Impaired gas exchange → V/Q mismatch and shunt
5. Clinical Features
Symptoms
- Dyspnea — acute onset, rapidly progressive
- Tachypnea (RR >30/min)
- Cough (may be productive)
- Hypoxia — cyanosis, low SpO₂
- Fever (may be high or may paradoxically decrease as condition worsens)
Signs
- Kussmaul breathing — deep sighing respiration due to metabolic acidosis (must be distinguished from true pulmonary edema)
- Bilateral crepitations on auscultation
- Features of severe malaria: altered consciousness, jaundice, hepatosplenomegaly, pallor
Timing
- Pulmonary edema classically develops after starting antimalarial treatment (paradoxical worsening) — thought to be due to sudden parasite clearance releasing pro-inflammatory mediators.
- Can appear within hours to days of admission.
6. Chest X-Ray Findings
The image below shows serial CXRs of ARDS secondary to P. vivax malaria across three patients (A, B, C), illustrating different rates of progression:
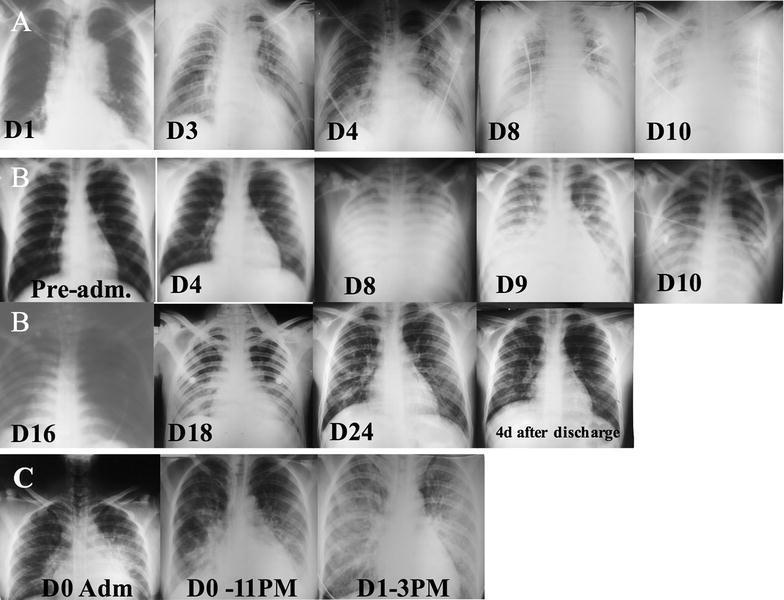
Patient A: Right-sided opacification → diffuse bilateral alveolar infiltrates and ground-glass opacities by Day 10.
Patient B: Rapid bilateral opacification by D8–16, including complete left hemithorax opacification, with gradual resolution by D24.
Patient C: Hyperacute progression from normal to dense bilateral infiltrates within 24 hours.
CXR findings in malaria-associated ARDS:
- Bilateral diffuse alveolar infiltrates / ground-glass opacities
- Air bronchograms
- No cardiomegaly (distinguishes from cardiogenic pulmonary edema)
- Normal or near-normal cardiac silhouette
- Kerley B lines absent (unlike LVF)
7. Diagnosis
Criteria (Berlin Definition for ARDS — Harrison's, p. 8195)
| Category | PaO₂/FiO₂ ratio | Mortality |
|---|---|---|
| Mild ARDS | 200–300 mmHg | ~27% |
| Moderate ARDS | 100–200 mmHg | ~32% |
| Severe ARDS | <100 mmHg | ~45% |
Additional criteria:
- Acute onset (<1 week)
- Bilateral infiltrates on CXR/CT not fully explained by effusion/collapse
- Not fully explained by cardiac failure (PAWP <18 or echocardiographic assessment)
Investigations
| Investigation | Finding |
|---|---|
| Peripheral blood smear | Parasitized RBCs (ring forms, trophozoites, schizonts) |
| RDT (Rapid Diagnostic Test) | HRP2, pLDH antigens positive |
| ABG | Hypoxemia (PaO₂ low), respiratory alkalosis early → metabolic acidosis late |
| CBC | Anaemia, thrombocytopenia |
| LFT | Elevated bilirubin (hemolytic + hepatic) |
| Serum lactate | Elevated in severe disease |
| CXR / CT Chest | Bilateral infiltrates, ground-glass opacities |
| ECHO | Preserved LV function (rules out cardiogenic cause) |
| PCWP (Swan-Ganz) | <18 mmHg (non-cardiogenic) |
| Blood culture | Rule out co-existing bacteremia |
8. Differential Diagnosis of Respiratory Distress in Malaria
| Cause | Key Feature |
|---|---|
| Malaria-associated ARDS | Bilateral infiltrates, non-cardiogenic, severe malaria |
| Metabolic acidosis (Kussmaul) | Deep breathing, no crackles, normal CXR |
| Aspiration pneumonia | Lobar/segmental consolidation, fever |
| Cardiogenic pulmonary edema | Elevated PCWP, cardiomegaly, Kerley B lines |
| Concurrent bacterial pneumonia | Productive cough, lobar consolidation |
| Anaemia-related dyspnea | Pallor, no infiltrates |
9. Management
A. Antimalarial Treatment (Treat the underlying cause)
| Drug | Regimen |
|---|---|
| Artesunate IV (1st line, severe malaria) | 2.4 mg/kg IV at 0, 12, 24 h then daily |
| Quinine IV + Doxycycline | Alternative if artesunate unavailable |
| Switch to oral ACT | Once tolerating orally (complete 3-day course) |
B. Respiratory Support
| Severity | Management |
|---|---|
| Mild hypoxia (SpO₂ 90–94%) | Supplemental O₂ via face mask (FiO₂ 40–60%) |
| Moderate ARDS (PaO₂/FiO₂ 100–200) | High-flow nasal cannula (HFNC) or NIV (CPAP/BiPAP) |
| Severe ARDS (PaO₂/FiO₂ <100) | Invasive mechanical ventilation |
C. Lung-Protective Ventilation Strategy (for ARDS)
- Tidal volume: 6 mL/kg ideal body weight (low VT strategy)
- Plateau pressure: <30 cmH₂O
- PEEP: Adequate PEEP (5–15 cmH₂O) to prevent de-recruitment
- FiO₂: Titrate to SpO₂ 88–95%
- Prone positioning: ≥16 hours/day if PaO₂/FiO₂ <150
- Permissive hypercapnia acceptable
D. Fluid Management
⚠️ Critical point: Fluid overload is a major precipitant of pulmonary edema in malaria. Aggressive IV fluids are CONTRAINDICATED.
- Cautious fluid resuscitation — target euvolemia
- Use 0.9% NaCl in small boluses (10 mL/kg over 30 min, reassess)
- Monitor CVP, urine output
- Use diuretics (furosemide) if fluid overload present
E. Additional Supportive Measures
| Intervention | Indication |
|---|---|
| Blood transfusion | If Hb <7 g/dL or haematocrit <20% |
| Treatment of hypoglycemia | 50% dextrose IV bolus |
| Broad-spectrum antibiotics | If concurrent bacterial infection suspected |
| Anti-convulsants | If seizures present |
| Renal replacement therapy | If AKI with oliguria |
| Nutritional support | NGT feeding if ventilated |
F. Interventions NOT Recommended
- Steroids — not beneficial, may worsen outcome
- Heparin — no proven benefit
- Mannitol — controversial, may worsen renal failure
10. Complications
| Complication | Details |
|---|---|
| Refractory hypoxemia | Leading cause of death in malaria ARDS |
| Secondary bacterial pneumonia | Ventilator-associated pneumonia (VAP) |
| Pneumothorax/barotrauma | From mechanical ventilation |
| Multi-organ dysfunction (MODS) | AKI + hepatic failure + DIC |
| Cerebral malaria | Concurrent CNS involvement |
11. Prognosis
- Mortality of malaria-associated ARDS: 50–80%
- Poor prognostic factors:
- High parasitemia (>5% pRBC)
- Severe acidosis (pH <7.2)
- Concurrent renal failure
- Delay in diagnosis and treatment
- PaO₂/FiO₂ <100 at presentation
- Survivors: may have full recovery of pulmonary function if survive the acute phase
12. Special Considerations
P. vivax and Pulmonary Disease
- Traditionally considered "benign" but increasing evidence of P. vivax-associated ARDS (as illustrated in the CXR series above)
- Mechanisms less well understood — possibly immune-mediated
- Responds to Chloroquine (where sensitive) + supportive care
Malaria in Pregnancy
- Pregnant women have heightened risk of pulmonary edema
- Quinine safer in 1st trimester; Artesunate preferred in 2nd/3rd trimester
- Monitor for hypoglycemia (worsened by quinine + pregnancy)
13. Summary Table for Quick Revision
| Feature | Detail |
|---|---|
| Most common organism | P. falciparum (also P. vivax |
| Mechanism | Cytoadherence, cytokine storm, endothelial injury |
| Key clinical sign | Tachypnea, hypoxia, bilateral crepitations |
| CXR finding | Bilateral diffuse alveolar infiltrates |
| PCWP | <18 mmHg (non-cardiogenic) |
| Ventilation strategy | Low tidal volume (6 mL/kg), adequate PEEP |
| Antimalaria drug of choice | IV Artesunate |
| Fluid strategy | Cautious — avoid overload |
| Mortality | 50–80% |
| Steroids | NOT recommended |
Key Exam Points to Remember
- Pulmonary edema in malaria is non-cardiogenic (low PCWP, normal cardiac function).
- It can occur paradoxically after starting treatment — explain the mechanism.
- Kussmaul breathing (metabolic acidosis) must be distinguished from true pulmonary edema — CXR and ABG are key.
- P. vivax can also cause ARDS — do not dismiss as benign.
- IV Artesunate is the drug of choice for severe malaria.
- Use lung-protective ventilation (6 mL/kg TV, PEEP, prone positioning).
- Steroids are NOT indicated — this is a classic exam trap.
- Fluid overload is both a trigger and a worsening factor — cautious fluid management is critical.
This is a shared conversation. Sign in to Orris to start your own chat.