Dengue and it's pulmonary disease Full details for md exams 15marks
Reading File
search_medical_text
dengue fever pathophysiology classification clinical features diagnosis
search_medical_text
dengue pulmonary manifestations lung complications dengue pneumonitis pleural effusion ARDS
search_medical_image
dengue pulmonary complications chest X-ray pleural effusion
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive, exam-ready answer on Dengue and its Pulmonary Manifestations for MD examinations.
Dengue Fever and Pulmonary Disease — Comprehensive Review (15 Marks)
1. Introduction
Dengue is an acute arboviral illness caused by the Dengue virus (DENV), a single-stranded RNA virus belonging to the family Flaviviridae, genus Flavivirus. It is transmitted by the bite of Aedes aegypti (primary vector) and Aedes albopictus mosquitoes. It is the most common arthropod-borne viral disease globally, with ~400 million infections per year (WHO 2023). Pulmonary involvement, once considered rare, is now recognized as a significant cause of morbidity and mortality in severe dengue.
2. Etiology and Epidemiology
| Feature | Details |
|---|---|
| Causative agent | DENV serotypes 1, 2, 3, 4 (DENV-5 reported rarely) |
| Vector | Aedes aegypti (primary), Aedes albopictus |
| Transmission | Bite of infected female mosquito (daytime biter) |
| Incubation period | 4–10 days |
| Endemic regions | Tropical & subtropical — Southeast Asia, Americas, Africa |
| Risk for severe disease | Secondary infection with a different serotype (antibody-dependent enhancement) |
3. Pathophysiology
Core Mechanisms:
- Viral replication in monocytes/macrophages, dendritic cells → release of TNF-α, IL-6, IL-8, IFN-γ
- Antibody-Dependent Enhancement (ADE): Pre-existing non-neutralizing antibodies from prior serotype enhance viral uptake by Fc-receptor-bearing cells → massive cytokine storm in secondary infection
- Capillary leak syndrome: Cytokines (especially C3a, C5a, VEGF, NS1 protein) disrupt endothelial tight junctions → plasma leakage into third spaces (pleural cavity, peritoneum, pericardium)
- Thrombocytopenia: Immune-mediated platelet destruction + suppressed megakaryopoiesis → bleeding tendency
- NS1 protein activates TLR4 → endothelial glycocalyx disruption → vascular permeability
4. WHO 2009 Classification (Revised)
Dengue
├── Dengue Without Warning Signs
├── Dengue With Warning Signs*
└── Severe Dengue
├── Severe plasma leakage → Dengue Shock Syndrome (DSS)
├── Severe bleeding
└── Severe organ impairment (liver, CNS, heart, kidney, LUNGS)
Warning signs*:
- Abdominal pain or tenderness
- Persistent vomiting
- Clinical fluid accumulation (pleural effusion, ascites)
- Mucosal bleeding
- Lethargy / restlessness
- Liver enlargement >2 cm
- Rapidly rising HCT with rapid platelet fall
(Clinical Management of Arboviral Diseases, WHO, p. 27)
5. Clinical Phases of Dengue
| Phase | Duration | Features |
|---|---|---|
| Febrile | Days 1–3 | High-grade fever (breakbone fever), flushing, myalgia, headache, retro-orbital pain, early rash |
| Critical | Days 4–6 | Defervescence; plasma leakage, DSS, organ failure — most dangerous |
| Recovery | Days 7–10 | Fluid reabsorption, bradycardia, confluent rash with islands of sparing |
6. Pulmonary Manifestations of Dengue — Core Focus
Pulmonary involvement occurs primarily during the critical phase and may persist into recovery. It is caused by capillary leak, immune-mediated injury, and volume overload.
6.1 Spectrum of Pulmonary Disease
| Manifestation | Mechanism | Frequency |
|---|---|---|
| Pleural Effusion | Plasma leakage (capillary leak) | Most common (20–40%) |
| Pulmonary Edema | Capillary leak + fluid overload | Common in severe dengue |
| ARDS (Acute Respiratory Distress Syndrome) | Cytokine storm + direct viral lung injury | 0.5–6% (high mortality) |
| Dengue Pneumonitis | Direct viral infection of lung parenchyma | Uncommon |
| Pulmonary Hemorrhage | Thrombocytopenia + coagulopathy | Rare, life-threatening |
| Diaphragmatic Weakness | Electrolyte imbalance, myositis | Rare |
6.2 Pleural Effusion
- Most common pulmonary complication
- Predominantly right-sided (due to hepatomegaly + perihepatic capillary leak); can be bilateral
- Exudative in nature (protein-rich plasma leaked)
- Clinically: Dyspnea, reduced breath sounds, stony dullness on percussion
- CXR/USG: Blunting of costophrenic angle, meniscus sign
- Management: Observation; reabsorbed spontaneously during recovery. Thoracocentesis only if causing respiratory compromise
6.3 Pulmonary Edema
- Two types:
- Non-cardiogenic (capillary leak) — predominant mechanism; cytokine-mediated endothelial injury → fluid into alveoli
- Cardiogenic — myocarditis, dengue-induced cardiac dysfunction (rare)
- CXR: Bilateral fluffy/alveolar opacities, Kerley B lines, enlarged cardiac silhouette
- Management: Fluid restriction, diuretics during recovery phase; cautious fluid resuscitation
6.4 ARDS in Dengue
- Defined by: Acute onset hypoxia (PaO₂/FiO₂ <300), bilateral infiltrates on CXR, non-cardiogenic origin (Berlin Definition)
- Dengue ARDS triggers:
- Direct alveolar damage by DENV
- Massive cytokine storm (TNF-α, IL-6, IL-8)
- Immune complex deposition in alveolar capillaries
- Iatrogenic fluid overload during resuscitation
- Clinical Features: Acute-onset dyspnea, progressive hypoxemia, diffuse bilateral crackles, refractory to O₂
- CXR/CT: Bilateral ground-glass opacities, consolidation, "white-out" lungs in severe ARDS
- Mortality: 20–50% in dengue ARDS
ARDS Management in Dengue:
- Lung-protective ventilation: Tidal volume 6 ml/kg IBW; plateau pressure <30 cmH₂O
- PEEP titration (FiO₂/PEEP table)
- Prone positioning if PaO₂/FiO₂ <150
- Fluid conservative strategy after initial resuscitation
- Treat underlying dengue — no specific antivirals; supportive care
- Corticosteroids: Not routinely recommended in dengue ARDS; controversial
6.5 Dengue Pneumonitis
- Direct viral infection of lung parenchyma
- Clinically resembles atypical pneumonia: Fever, cough, exertional dyspnea, hypoxia
- CXR: Patchy interstitial infiltrates
- BAL: May show lymphocytic alveolitis; viral RNA detectable
- Must be differentiated from bacterial superinfection
- Treatment: Supportive; no specific antivirals
6.6 Pulmonary Hemorrhage
- Rare but life-threatening
- Due to severe thrombocytopenia (platelets <10,000/μL) + DIC
- Presents as: Massive hemoptysis, blood-tinged endotracheal secretions, rapidly falling Hb
- CXR: Dense unilateral or bilateral opacities (blood-filled alveoli)
- Management: Platelet transfusion (target >50,000 for active bleed), FFP for coagulopathy, intubation if massive
7. Chest X-Ray in Dengue — Key Findings
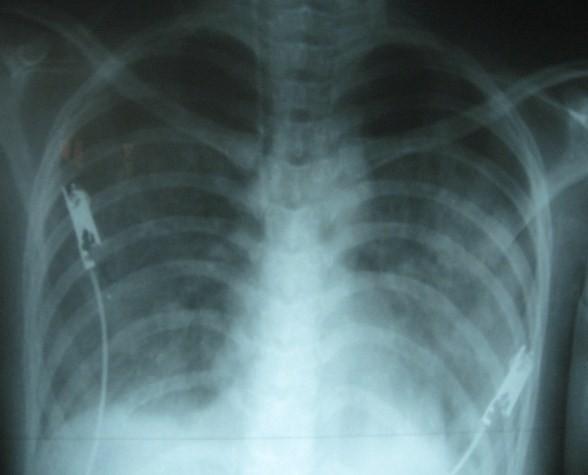
AP CXR in a 19-year-old female with Dengue Shock Syndrome: bilateral diffuse fluffy opacities (pulmonary edema), blunting of right costophrenic angle (pleural effusion), and enlarged cardiac silhouette. ECG leads visible — acute monitoring setting.
| CXR Finding | Associated Condition |
|---|---|
| Right-sided blunting of CPA | Pleural effusion (most common) |
| Bilateral fluffy alveolar opacities | Pulmonary edema / ARDS |
| Ground-glass opacities | Pneumonitis / early ARDS |
| Unilateral consolidation | Pneumonitis / hemorrhage |
| Enlarged cardiac silhouette | Pericardial effusion / myocarditis |
8. Diagnosis
Laboratory Diagnosis
| Test | Window | Utility |
|---|---|---|
| NS1 Antigen | Days 1–5 | Early diagnosis; highly specific |
| IgM ELISA | Day 5 onwards | Acute/recent infection |
| IgG ELISA | Secondary infection | High titer in secondary dengue |
| RT-PCR (Gold standard) | Days 1–5 | Serotyping; confirms viremia |
| CBC | Throughout | Thrombocytopenia + leukopenia + rising HCT |
| NS1 + IgM combo | Days 1–7 | Highest sensitivity in first week |
Investigations for Pulmonary Assessment
- Chest X-ray: First-line; detects effusion, edema, infiltrates
- HRCT Chest: Ground-glass opacities, consolidation, interlobular septal thickening
- Pulse oximetry / ABG: PaO₂/FiO₂ ratio for ARDS classification
- Bedside USG: Rapidly detects pleural effusion (>95% sensitivity)
- Echocardiography: Rule out cardiogenic cause; detect pericardial effusion
9. Differential Diagnosis of Pulmonary Involvement
| Condition | Distinguishing Features |
|---|---|
| Leptospirosis | Weil's disease; conjunctival suffusion; renal failure |
| Hantavirus pulmonary syndrome | Rodent exposure; Sin Nombre virus |
| Scrub typhus with lung | Eschar present; responds to doxycycline |
| Influenza pneumonia | Rapid A/H5N1 test; seasonal clustering |
| Bacterial CAP | Lobar consolidation; neutrophilia; responds to antibiotics |
| Malaria | Peripheral smear/RDT positive; P. falciparum |
10. Management
A. General Principles
- No specific antiviral therapy — management is entirely supportive
- Three-group WHO triage:
- Group A: Outpatient (no warning signs, able to tolerate orals)
- Group B: In-hospital (warning signs, comorbidities)
- Group C: ICU (severe dengue — DSS, ARDS, severe bleeding, organ failure)
B. Fluid Management (Critical)
| Phase | Strategy |
|---|---|
| Febrile phase | Oral ORS; paracetamol for fever |
| Critical phase (DSS) | IV crystalloids (NS/RL) 10–20 ml/kg bolus; titrate by HCT, BP, UO |
| Recovery phase | Fluid restriction + diuretics to prevent pulmonary edema from fluid reabsorption |
⚠️ Key Exam Point: Fluid overload during the recovery phase (Days 7–10) is the most common iatrogenic cause of pulmonary edema in dengue. Plasma is reabsorbed from third spaces → intravascular overload → pulmonary edema.
C. Respiratory Management
- Supplemental O₂ for SpO₂ <94%
- High-flow nasal cannula (HFNC) for moderate hypoxemia
- NIV / Intubation for ARDS (PaO₂/FiO₂ <200)
- Lung-protective ventilation: TV 6 ml/kg, Pplat <30, PEEP titrated
- Prone positioning for severe ARDS (PaO₂/FiO₂ <150 for >12 hours)
D. Specific Interventions
| Indication | Intervention |
|---|---|
| Pleural effusion + respiratory compromise | Thoracocentesis |
| Platelet <10,000 or active bleed with low platelets | Platelet transfusion |
| Massive hemorrhage/DIC | FFP, cryoprecipitate |
| Secondary bacterial pneumonia | Targeted antibiotics |
| Myocarditis with cardiogenic edema | Dobutamine, avoid overload |
E. Drugs to AVOID
- Aspirin / NSAIDs — increase bleeding risk
- Antibiotics — not for uncomplicated dengue
- Corticosteroids — not proven beneficial; may increase viral replication
- IM injections — hematoma risk with thrombocytopenia
11. Complications Summary
| System | Complication |
|---|---|
| Pulmonary | Pleural effusion, ARDS, pulmonary edema, pneumonitis, pulmonary hemorrhage |
| Cardiovascular | DSS, myocarditis, arrhythmias, pericardial effusion |
| Hepatic | Dengue hepatitis, fulminant hepatic failure |
| Neurological | Dengue encephalitis, Guillain-Barré, transverse myelitis |
| Renal | AKI, hyponatremia |
| Hematological | DIC, severe thrombocytopenia |
12. Prognosis
- Uncomplicated dengue: Self-limiting, mortality <1%
- Dengue with ARDS: Mortality 20–50%
- DSS: Mortality <1% with adequate management; up to 10–40% if untreated
- Poor prognostic markers: Fluid overload, ARDS, pulmonary hemorrhage, myocarditis, elevated liver enzymes, prolonged shock
13. Prevention
- Dengvaxia (CYD-TDV): Licensed; only for seropositive individuals ≥9 years; risk of severe disease in seronegative recipients
- TAK-003 (Qdenga): Newer vaccine; approved in some countries; effective against all 4 serotypes
- Vector control: Source reduction (eliminate standing water), larviciding, insecticide spraying
- Personal protection: Repellents (DEET), long-sleeved clothing, mosquito nets
14. Key Exam Points (High-Yield Summary)
- Most common pulmonary complication = Pleural effusion (right-sided)
- Most dangerous pulmonary complication = ARDS / Pulmonary hemorrhage
- Mechanism of lung injury = Capillary leak (cytokine-mediated endothelial damage) + fluid overload in recovery
- NS1 antigen = earliest serological marker (Days 1–5)
- Critical phase = Days 4–6 (defervescence phase) — most pulmonary complications occur here
- Avoid NSAIDs/aspirin — worsens bleeding
- Fluid restriction in recovery phase = prevents iatrogenic pulmonary edema
- ARDS management = Lung-protective ventilation (TV 6 ml/kg, Pplat <30 cmH₂O)
- Platelet transfusion threshold = <10,000/μL (prophylactic) or active hemorrhage regardless of count
- Dengvaxia risk: Contraindicated in seronegative individuals — increases risk of severe dengue
References: WHO Clinical Management of Arboviral Diseases (Dengue, Chikungunya, Zika, Yellow Fever), p. 27; Harrison's Principles of Internal Medicine, 21st Edition; WHO Dengue Guidelines 2009 (revised); Berlin Definition of ARDS 2012.
This is a shared conversation. Sign in to Orris to start your own chat.