Glomerulonephritis
Reading File
search_medical_text
glomerulonephritis etiology pathophysiology classification diagnosis management
search_medical_image
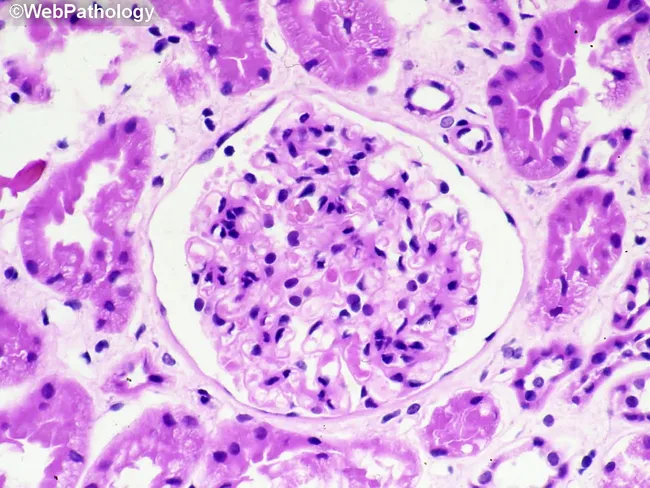
glomerulonephritis histology microscopy renal biopsy
GradeResponse
GradeResponse
Glomerulonephritis (GN)
Overview
Glomerulonephritis refers to a heterogeneous group of conditions characterized by inflammation of the glomeruli, typically presenting with hematuria, proteinuria, hypertension, and varying degrees of renal impairment. It is a leading cause of chronic kidney disease (CKD) and end-stage renal disease (ESRD) worldwide.
Classification
GN is broadly classified by clinical syndrome, histopathology, and immunofluorescence pattern:
By Clinical Syndrome
| Syndrome | Key Features |
|---|---|
| Nephritic | Hematuria (dysmorphic RBCs, RBC casts), proteinuria <3.5 g/day, HTN, oliguria, azotemia |
| Nephrotic | Proteinuria >3.5 g/day, edema, hypoalbuminemia, hyperlipidemia, lipiduria |
| Mixed | Features of both (e.g., membranoproliferative GN) |
| RPGN | Rapidly progressive GN — rapid loss of renal function over days to weeks |
| Asymptomatic hematuria/proteinuria | Incidental finding, often IgA nephropathy |
Etiology & Specific Subtypes
Primary GN (intrinsic renal disease)
| Type | IF Pattern | Key Features |
|---|---|---|
| IgA Nephropathy (Berger's) | Mesangial IgA | Episodic gross hematuria after mucosal infections; most common primary GN globally |
| Minimal Change Disease | Negative (normal LM) | Podocyte effacement on EM; most common nephrotic in children |
| Focal Segmental Glomerulosclerosis (FSGS) | IgM/C3 (segmental) | Podocyte injury; common in adults, associated with obesity, HIV, heroin |
| Membranous Nephropathy | Granular IgG along GBM | Anti-PLA2R antibodies in ~70% of primary cases; #1 nephrotic in older adults |
| Membranoproliferative GN (MPGN) | Mixed granular | Tram-track GBM on LM; complement dysregulation or immune complex deposition |
| Anti-GBM disease (Goodpasture's) | Linear IgG along GBM | Anti-GBM antibodies; pulmonary hemorrhage + nephritis = Goodpasture syndrome |
| Pauci-immune GN | Negative | ANCA-associated: GPA, MPA, EGPA |
Secondary GN (systemic disease)
| Cause | GN Type |
|---|---|
| SLE | Lupus nephritis (classes I–VI), "full-house" IF pattern |
| Diabetes | Diabetic glomerulosclerosis |
| Strep infection | Post-infectious/post-streptococcal GN |
| Hepatitis B/C | Membranous (HBV), MPGN (HCV + cryoglobulinemia) |
| HIV | Collapsing FSGS (HIVAN) |
| Amyloidosis | AA or AL amyloid deposition |
| Vasculitis | IgA vasculitis (HSP), ANCA-associated vasculitis |
Pathophysiology
Key mechanisms (Harrison's, p. 8477):
- Immune complex deposition — in situ (e.g., anti-GBM, membranous) or circulating (e.g., post-infectious, lupus nephritis)
- Complement activation — classical or alternative pathway → inflammation, GBM damage
- Cell-mediated immunity — podocyte injury in MCD/FSGS
- ANCA-mediated neutrophil activation — pauci-immune necrotizing GN
- Hyperfiltration — shared final pathway in CKD progression regardless of initial cause
Rapidly Progressive GN (RPGN)
A nephrology emergency. Characterized histologically by crescent formation — proliferating parietal epithelial cells and infiltrating leukocytes compressing the capillary tuft (webpathology.com).
RPGN Classification
| Type | Immunofluorescence | Cause |
|---|---|---|
| Type I | Linear IgG | Anti-GBM disease / Goodpasture's |
| Type II | Granular | Immune complex GN (SLE, post-infectious) |
| Type III | Pauci-immune (negative) | ANCA-associated vasculitis (GPA, MPA) |
Clinical Features
- Hematuria: gross (tea/cola-colored urine) or microscopic; dysmorphic RBCs and RBC casts are pathognomonic of glomerular origin
- Proteinuria: sub-nephrotic or nephrotic range
- Hypertension: due to salt/water retention
- Edema: periorbital, peripheral
- Oliguria / Azotemia: in severe disease
- Systemic symptoms: fever, rash, arthritis, respiratory involvement (in systemic vasculitis)
Diagnosis
Laboratory
| Test | Purpose |
|---|---|
| Urinalysis + microscopy | RBC casts, dysmorphic RBCs, proteinuria |
| Spot urine PCR/ACR | Quantify proteinuria |
| BMP / creatinine | Assess GFR, electrolytes |
| CBC | Anemia (microangiopathic in severe disease) |
| ANA, anti-dsDNA, complement (C3/C4) | Lupus nephritis |
| ANCA (PR3, MPO) | Pauci-immune / vasculitis |
| Anti-GBM antibodies | Goodpasture's / anti-GBM disease |
| Anti-PLA2R | Primary membranous nephropathy |
| ASO, complement | Post-streptococcal GN |
| HBsAg, HCV Ab, HIV | Viral-associated GN |
| Serum/urine protein electrophoresis | Amyloidosis, multiple myeloma |
| Cryoglobulins | Cryoglobulinemic GN |
Imaging
- Renal ultrasound: assess kidney size (small = CKD, large = acute or infiltrative)
Renal Biopsy — Gold Standard
- Light microscopy: proliferation pattern, crescents, sclerosis
- Immunofluorescence: IgG, IgA, IgM, C3, C1q — pattern and distribution
- Electron microscopy: location of deposits (subepithelial, subendothelial, mesangial)
Management
General Principles
- Control hypertension — ACE inhibitors or ARBs (reduce proteinuria and slow CKD progression)
- Fluid and electrolyte management
- Dietary salt and protein restriction
- Treat underlying systemic disease
Disease-Specific Treatment
| GN Type | Treatment |
|---|---|
| Post-streptococcal GN | Supportive; antibiotics for active infection |
| IgA Nephropathy | RAAS blockade; steroids if proteinuria >1 g/day; SGLT2i; sparsentan (FDA 2023) |
| Minimal Change Disease | Oral prednisone (1 mg/kg/day); cyclophosphamide or calcineurin inhibitors for relapse |
| Membranous Nephropathy | RAAS blockade; rituximab (anti-CD20) for moderate-high risk; cyclophosphamide + steroids (Ponticelli) |
| Lupus Nephritis (Class III/IV) | Induction: mycophenolate mofetil + hydroxychloroquine + steroids; maintenance: MMF or azathioprine |
| ANCA-associated GN | Induction: rituximab or cyclophosphamide + high-dose steroids; plasma exchange if severe |
| Anti-GBM disease | Plasma exchange + cyclophosphamide + steroids (urgent) |
| FSGS | RAAS blockade; steroids; sparsentan; voclosporin for steroid-resistant |
Complications
- Acute kidney injury → ESRD
- Hypertensive emergency
- Hyperkalemia, metabolic acidosis
- Nephrotic complications: thromboembolism (renal vein thrombosis), infection (loss of immunoglobulins), hyperlipidemia
- Pulmonary hemorrhage (anti-GBM, ANCA vasculitis)
- CKD progression driven by hyperfiltration and glomerular hypertrophy (Harrison's, p. 8477)
Prognosis
Highly variable by subtype:
- Post-infectious GN: excellent — most cases resolve completely in children
- IgA nephropathy: ~20–40% progress to ESRD over 20–30 years
- Anti-GBM disease: poor without urgent treatment; irreversible if >50% crescents on biopsy
- ANCA-associated GN: remission achievable in ~80–90% with immunosuppression; relapse common
- Lupus nephritis Class III/IV: ~10–20% reach ESRD despite treatment
This is a shared conversation. Sign in to Orris to start your own chat.