Explain me atleast 20 common heart disease with its ECG changes and ECG images of those diseases
ECG changes heart disease myocardial infarction
atrial fibrillation ECG tracing
heart block bradycardia ECG
ventricular tachycardia ventricular fibrillation ECG
hypertrophic cardiomyopathy dilated cardiomyopathy ECG LVH
pericarditis Wolff-Parkinson-White syndrome ECG changes
pulmonary embolism right heart strain ECG S1Q3T3
long QT syndrome Brugada syndrome ECG pattern
aortic stenosis mitral stenosis cardiac ECG findings
atrial flutter supraventricular tachycardia AVNRT ECG sawtooth waves
20 common heart diseases ECG changes electrocardiogram findings
20 Common Heart Diseases: ECG Changes & Images
1. 🫀 Acute ST-Elevation Myocardial Infarction (STEMI)
ECG Changes:
- Hyperacute T waves (earliest finding — tall, peaked, symmetric)
- ST-segment elevation ≥1 mm in ≥2 contiguous leads (convex/tombstone morphology)
- Reciprocal ST depression in opposite leads
- Pathological Q waves (>40 ms wide, >25% QRS amplitude) — develop after hours
- T-wave inversion in the evolutionary phase
- New LBBB is treated as STEMI equivalent
| Territory | Leads with STE | Culprit Artery |
|---|---|---|
| Anterior | V1–V4 | LAD |
| Anterolateral | V1–V6, I, aVL | Proximal LAD |
| Inferior | II, III, aVF | RCA / LCx |
| Posterior | ST depression V1–V3 (mirror) | RCA / LCx |
Anterior STEMI — Tombstone pattern:
Anterolateral STEMI:

Inferior STEMI with reciprocal changes:
2. 🫀 Non-ST-Elevation Myocardial Infarction (NSTEMI) / Unstable Angina
ECG Changes:
- ST-segment depression (horizontal or downsloping) in ischemic leads
- T-wave inversion (symmetric, deep)
- No ST elevation and no Q waves
- Dynamic ECG changes (worsen with symptoms)
- Leads may be normal in 1–6% of NSTEMI
Evolutionary Inferior MI (post-PCI changes):
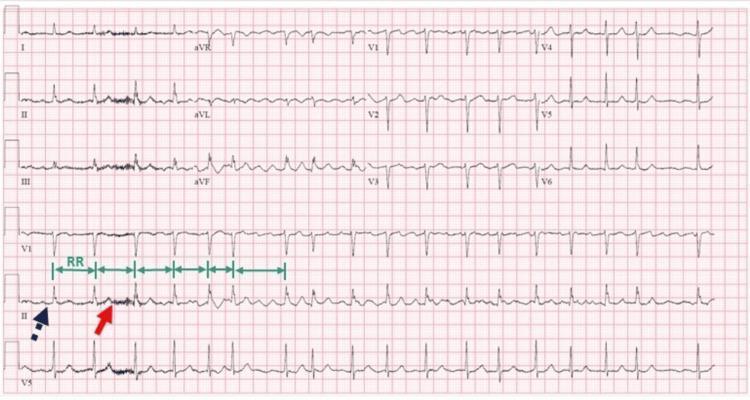
3. 🫀 Atrial Fibrillation (AF)
ECG Changes:
- Absent P waves — replaced by fine fibrillatory (f) waves, best seen in V1
- Irregularly irregular R-R intervals — the hallmark
- Narrow QRS complexes (unless aberrant conduction or pre-excitation)
- Ventricular rate variable (60–200+ bpm depending on AV node)
- Baseline chaotic, undulating
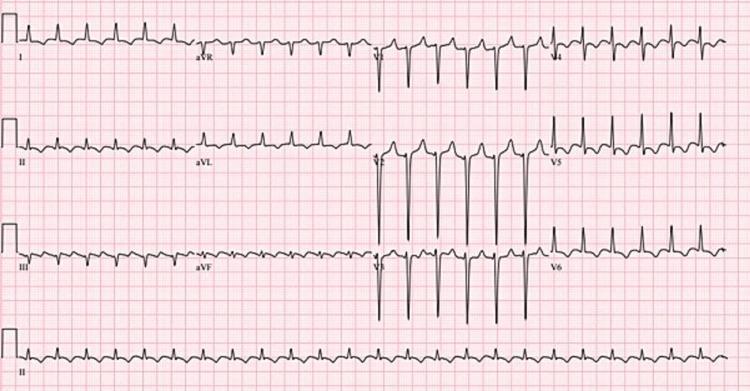
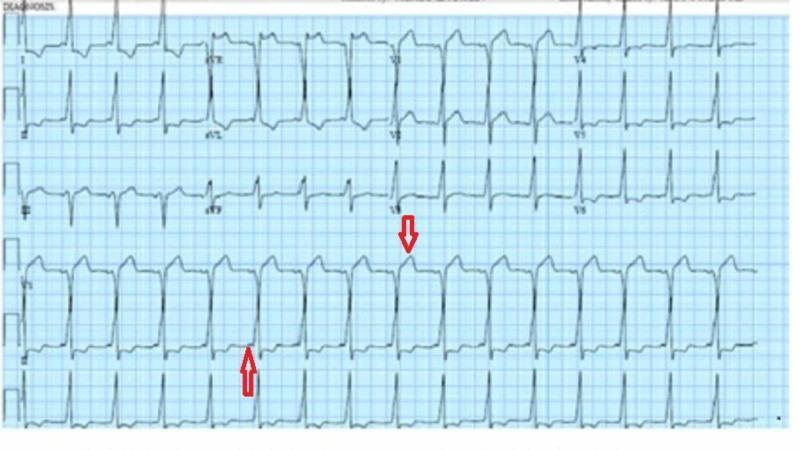
4. 🫀 Atrial Flutter
ECG Changes:
- "Sawtooth" flutter (F) waves at ~300 bpm — best seen in II, III, aVF, V1
- Regular ventricular response — typically 2:1 (150 bpm), 3:1, or 4:1
- No isoelectric baseline between flutter waves
- Narrow QRS complexes
- Counter-clockwise flutter (typical) = negative F-waves in inferior leads
5. 🫀 Third-Degree (Complete) AV Block
ECG Changes:
- Complete AV dissociation — P waves and QRS complexes occur independently
- Bradycardia — ventricular rate 20–40 bpm (escape rhythm)
- Wide QRS if ventricular escape (>120 ms); narrow if junctional escape
- P rate > QRS rate (atrial rate normal ~60–100 bpm)
- No relationship between P waves and QRS complexes

6. 🫀 First-Degree AV Block
ECG Changes:
- Prolonged PR interval >200 ms (>5 small squares)
- Every P wave followed by a QRS — 1:1 conduction maintained
- QRS complexes narrow and morphologically normal
- Benign finding; commonly caused by vagal tone, medications, or inferior MI
7. 🫀 Second-Degree AV Block (Mobitz Type I & II)
ECG Changes:
- Progressive PR prolongation → dropped QRS
- Grouped beating pattern
- Site of block: AV node (usually benign)
- Constant PR interval → sudden dropped QRS (no warning)
- Often with bundle branch block
- Site of block: His-Purkinje (more dangerous, can progress to complete block)
8. 🫀 Right Bundle Branch Block (RBBB)
ECG Changes:
- RSR' pattern ("M pattern") in V1–V3 — rabbit ears
- Wide, slurred S waves in I, aVL, V5–V6
- QRS duration ≥120 ms (complete RBBB)
- Secondary ST-T changes — ST depression + T-wave inversion in V1–V3
- Normal axis usually
9. 🫀 Left Bundle Branch Block (LBBB)
ECG Changes:
- Broad, notched ("M-shaped") R waves in I, aVL, V5–V6
- Deep QS or rS in V1–V3 (no septal Q waves in lateral leads)
- QRS duration ≥120 ms
- Discordant ST-T changes (ST/T opposite to QRS)
- Left axis deviation common
- New LBBB = STEMI equivalent until proven otherwise (Sgarbossa criteria)
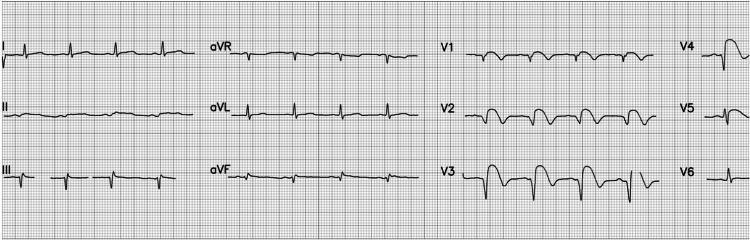
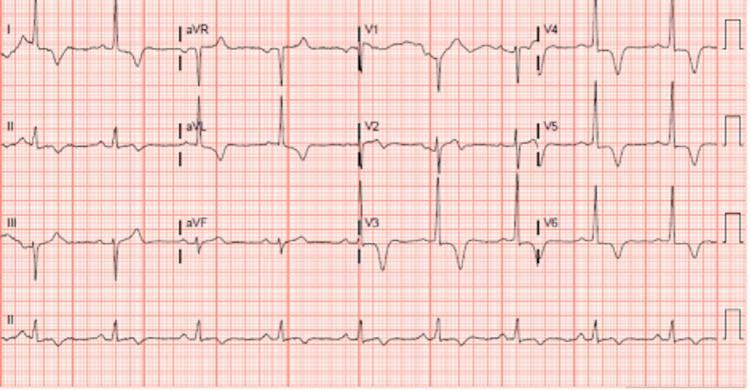
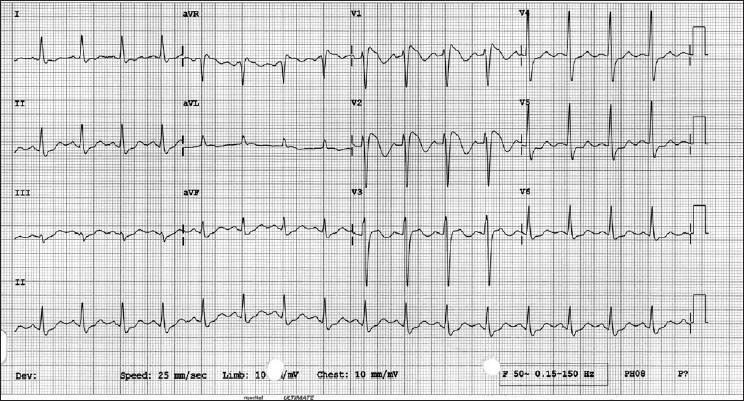
10. 🫀 Hypertrophic Cardiomyopathy (HCM)
ECG Changes:
- Left ventricular hypertrophy (LVH) voltage criteria — tall R in V4–V6, deep S in V1–V3 (Sokolow-Lyon >35 mm)
- Deep, giant, symmetric T-wave inversions in V2–V6 (especially apical HCM / Yamaguchi syndrome)
- Lateral ST depression and T-wave inversions (strain pattern)
- Pathological Q waves in inferior and lateral leads (septal hypertrophy)
- Left axis deviation
- Atrial enlargement (broad, notched P waves in II)
11. 🫀 Dilated Cardiomyopathy (DCM)
ECG Changes:
- Low voltage QRS in limb leads (<5 mm) or precordial leads (<10 mm)
- LBBB pattern (very common)
- Non-specific ST-T wave changes
- Sinus tachycardia (compensatory)
- Atrial fibrillation (common complication)
- Pathological Q waves (pseudo-infarct pattern)
- Left atrial enlargement
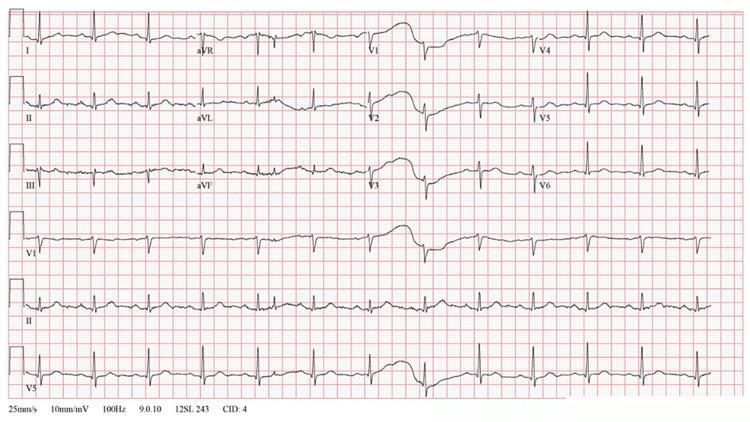
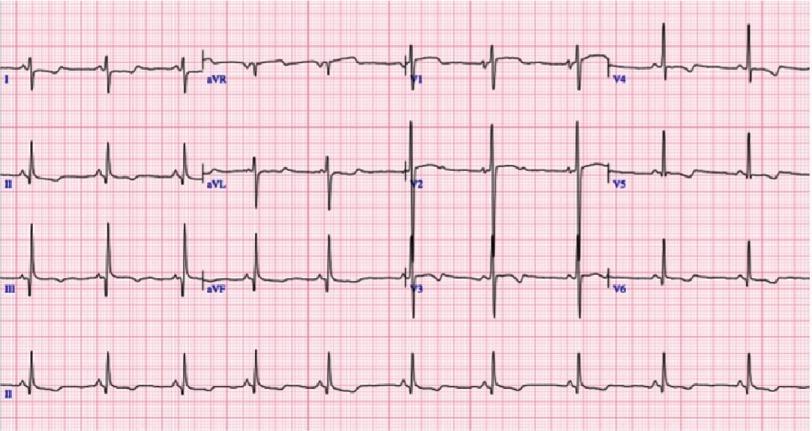
12. 🫀 Acute Pericarditis
ECG Changes (4 classic stages):
- Stage I — Diffuse saddle-shaped (concave up) ST elevation in most leads + PR depression (most specific sign); ST elevation in aVR with PR elevation
- Stage II — ST normalises, T waves flatten
- Stage III — T-wave inversions (without Q waves)
- Stage IV — Normalisation (weeks later)
- ST changes are diffuse (not territorial)
- No reciprocal depression (except aVR/V1)
- PR depression is hallmark
- No Q waves develop
13. 🫀 Pericardial Effusion / Cardiac Tamponade
ECG Changes:
- Sinus tachycardia
- Low QRS voltage (fluid dampening electrical signals)
- Electrical alternans — beat-to-beat alternation in QRS amplitude/axis (pathognomonic for large effusion/tamponade)
- P wave alternans may also occur
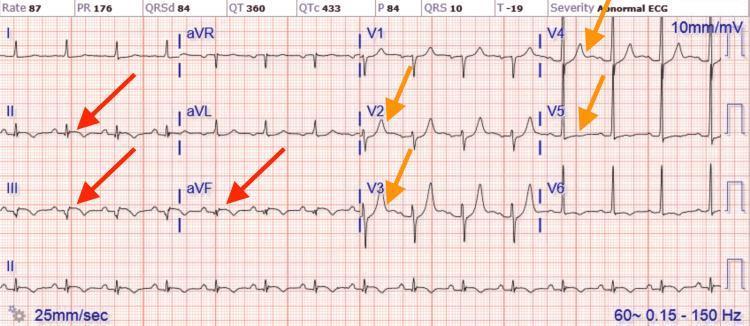
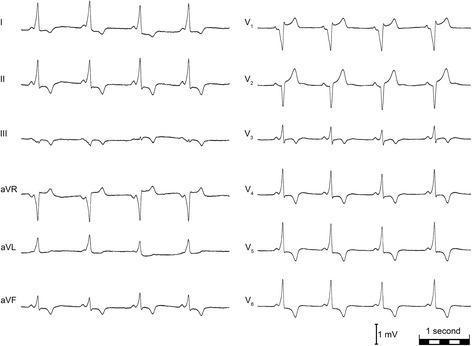
14. 🫀 Pulmonary Embolism (PE)
ECG Changes:
- Sinus tachycardia (most common finding, ~44%)
- S1Q3T3 pattern: Deep S in I + Q wave in III + T-wave inversion in III
- Incomplete or complete RBBB
- T-wave inversions in V1–V4 (right ventricular strain)
- Right axis deviation
- P pulmonale (peaked P in II >2.5 mm)
- New AF or flutter possible


15. 🫀 Wolff-Parkinson-White (WPW) Syndrome
ECG Changes:
- Short PR interval <120 ms (accessory pathway bypasses AV node delay)
- Delta wave — slurred upstroke at start of QRS (pre-excitation)
- Wide QRS (>120 ms) due to delta wave
- Secondary ST-T changes discordant with QRS
- Pseudo-infarct Q waves possible
- Risk: AF with rapid ventricular response through accessory pathway → VF
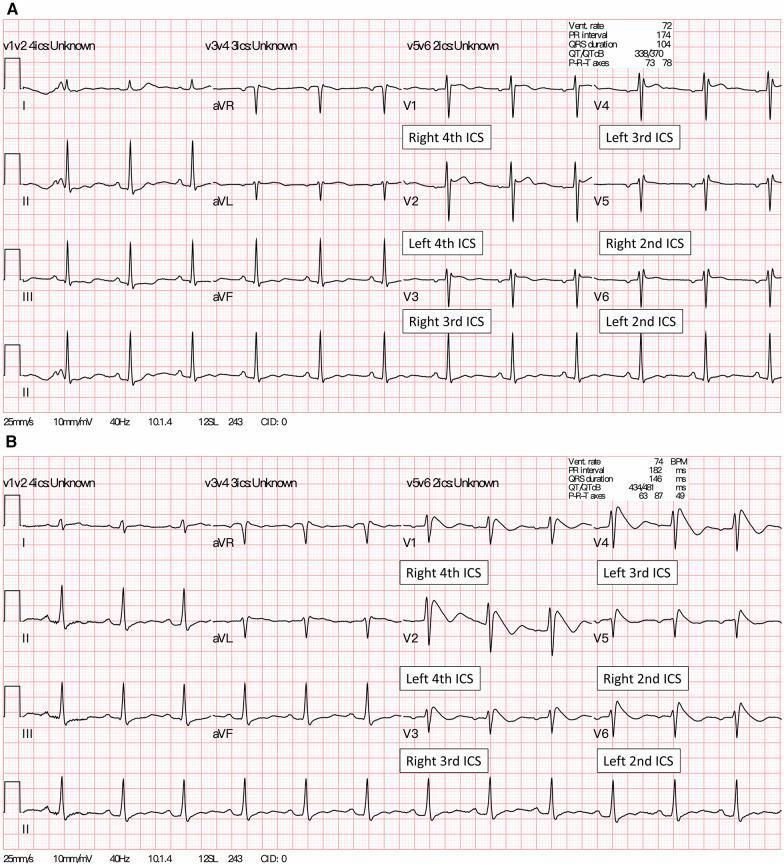
16. 🫀 Brugada Syndrome
ECG Changes:
- Type 1 (diagnostic): "Coved" ST elevation ≥2 mm with descending ST → negative T-wave in V1–V2 ("shark fin" or "ski slope")
- Type 2: "Saddleback" morphology — ST elevation ≥2 mm, rises then dips, upright T-wave (not diagnostic alone)
- Changes in right precordial leads V1–V3
- PR prolongation possible
- Normal QT interval
- Risk: ventricular fibrillation and sudden cardiac death (especially at rest/fever)
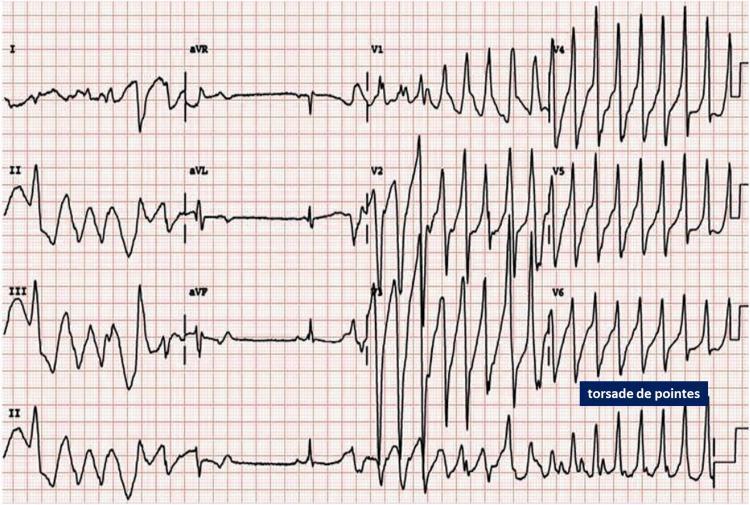
17. 🫀 Long QT Syndrome (LQTS)
ECG Changes:
- Prolonged QTc interval >450 ms (males), >460 ms (females), >480 ms pathological
- Corrected using Bazett formula: QTc = QT / √RR
- T-wave abnormalities — notched, biphasic, broad T waves
- Risk: Torsades de Pointes (TdP) — polymorphic VT with twisting QRS axis around baseline → VF → sudden death
Torsades de Pointes (complication of long QT):
18. 🫀 Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy (ARVC)
ECG Changes:
- Epsilon wave — small positive deflection at end of QRS in V1–V3 (pathognomonic — fibrofatty RV infiltration)
- T-wave inversions in V1–V4 (right precordial leads)
- Localised QRS prolongation >110 ms in V1–V3
- RBBB pattern (complete or incomplete)
- Ventricular tachycardia with LBBB morphology (arises from RV)
- S-wave upstroke >55 ms in V1–V3
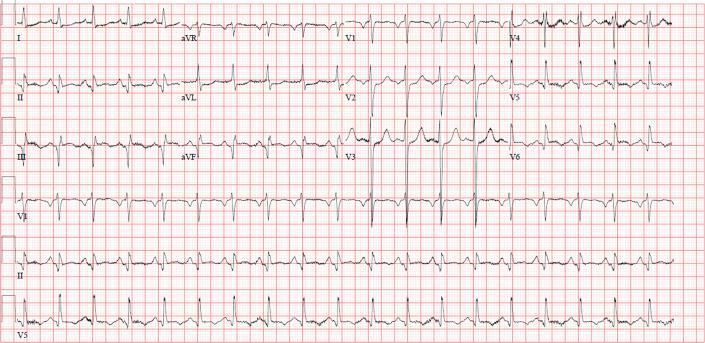
19. 🫀 Heart Failure with Left Ventricular Hypertrophy (LVH)
ECG Changes (Sokolow-Lyon criteria):
- S in V1 + R in V5 or V6 >35 mm
- R in aVL >11 mm
- LV strain pattern: ST depression + T-wave inversion in I, aVL, V5–V6
- Left axis deviation
- Broad, notched P waves (P mitrale) → left atrial enlargement
- LBBB pattern in severe disease
20. 🫀 Ventricular Tachycardia (VT)
ECG Changes:
- Wide complex tachycardia — QRS ≥120 ms, rate >100 bpm
- AV dissociation — P waves independent of QRS (key feature)
- Fusion beats and capture beats (diagnostic when present)
- Concordance — all precordial leads same polarity (positive or negative)
- Extreme axis deviation ("northwest axis")
- LBBB morphology VT = RV origin; RBBB morphology VT = LV origin
- Can degenerate into ventricular fibrillation (VF)
21. 🫀 Ventricular Fibrillation (VF)
ECG Changes:
- Chaotic, irregular, baseline oscillations — no identifiable P waves, QRS, or T waves
- Variable amplitude and frequency
- Completely disorganized electrical activity
- Medical emergency — requires immediate defibrillation
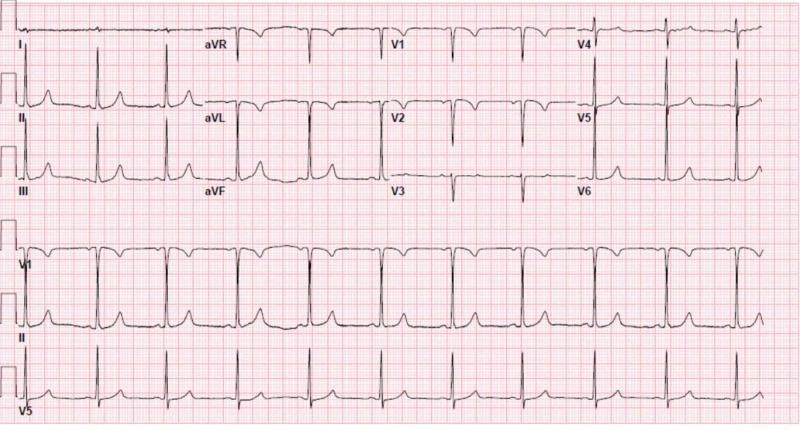
22. 🫀 Hyperkalemia
ECG Changes (progressive with rising K⁺):
- K⁺ 5.5–6.5 mmol/L: Tall, peaked ("tented") T waves (narrow base)
- K⁺ 6.5–7.5 mmol/L: Prolonged PR interval, widened QRS
- K⁺ >7.5 mmol/L: Flattened/absent P waves, sine wave pattern
- K⁺ >8–9 mmol/L: VF or asystole
23. 🫀 Hypokalemia
ECG Changes:
- Flattened or inverted T waves
- Prominent U waves (positive deflection after T wave, best seen V2–V3)
- ST depression
- Prolonged QT interval (when U wave merges with T wave)
- PR prolongation
- Risk of VT/TdP with severe hypokalemia
24. 🫀 Mitral Stenosis
ECG Changes:
- P mitrale — broad, notched P waves ≥120 ms in lead II (bifid P) = left atrial enlargement
- Biphasic P wave in V1 — terminal negative component (LA abnormality)
- Right ventricular hypertrophy signs if pulmonary hypertension develops: right axis deviation, dominant R in V1
- Atrial fibrillation (very common complication — LA dilation)
- P pulmonale in severe PAH
Quick Reference Table
| # | Disease | Key ECG Finding |
|---|---|---|
| 1 | STEMI | ST elevation + Q waves (territorial) |
| 2 | NSTEMI | ST depression + T-wave inversion |
| 3 | Atrial Fibrillation | Absent P waves, irregularly irregular |
| 4 | Atrial Flutter | Sawtooth F-waves ~300 bpm, 2:1 block |
| 5 | Complete AV Block | P-QRS dissociation, bradycardia |
| 6 | First-degree AV Block | PR >200 ms |
| 7 | Mobitz II | Fixed PR → sudden dropped QRS |
| 8 | RBBB | RSR' in V1, slurred S in V5–V6 |
| 9 | LBBB | Notched R in I/V5–V6, QS in V1 |
| 10 | HCM | Giant T-wave inversions V2–V6, LVH |
| 11 | DCM | Low voltage, LBBB, AF |
| 12 | Pericarditis | Diffuse concave ST↑, PR depression |
| 13 | Tamponade | Electrical alternans, low voltage |
| 14 | Pulmonary Embolism | S1Q3T3, RBBB, RV strain |
| 15 | WPW | Short PR, delta wave, wide QRS |
| 16 | Brugada | Coved ST↑ V1–V2, Type 1 |
| 17 | Long QT / TdP | QTc >460 ms, Torsades de Pointes |
| 18 | ARVC | Epsilon wave V1–V3, TWI V1–V4 |
| 19 | LVH / Heart Failure | Sokolow voltage >35 mm, strain pattern |
| 20 | VT/VF | Wide complex tachy, AV dissociation / chaos |
| 21 | Hyperkalemia | Peaked T waves → sine wave |
| 22 | Hypokalemia | Flat T, prominent U waves |
| 23 | Mitral Stenosis | P mitrale, AF, RVH |
Clinical Note: ECG changes should always be interpreted alongside clinical history, symptoms, and other investigations. A single ECG finding is rarely diagnostic in isolation — serial ECGs and troponin measurements are essential for ischemic syndromes.
You are not providing ECG images of all diseases. Please show me all diseases ECG
NSTEMI non-ST elevation myocardial infarction ST depression T wave inversion ECG
left bundle branch block LBBB ECG wide QRS notched R wave
acute pericarditis diffuse ST elevation PR depression ECG saddle shape
cardiac tamponade electrical alternans low voltage ECG
ventricular tachycardia wide complex tachycardia AV dissociation ECG
ventricular fibrillation chaotic baseline ECG
hyperkalemia peaked T waves wide QRS sine wave ECG potassium
hypokalemia flat T wave prominent U wave ECG
left ventricular hypertrophy LVH ECG Sokolow voltage criteria strain pattern
ARVC arrhythmogenic right ventricular cardiomyopathy epsilon wave ECG T wave inversion V1 V3
Mobitz type 2 second degree AV block Wenckebach dropped QRS ECG