Bppv
Reading File
Finding Sources
Searching PubMed
"benign paroxysmal positional vertigo"[MeSH Terms] AND treatment
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a thorough review of Benign Paroxysmal Positional Vertigo (BPPV):
Benign Paroxysmal Positional Vertigo (BPPV)
Definition & Epidemiology
BPPV is the most common cause of dizziness seen by otolaryngologists. It is characterized by brief, paroxysmal attacks of vertigo and nystagmus triggered by specific head position changes - not by a sustained position, but by the act of changing position (hence some prefer the term "positioning vertigo"). Individual episodes last less than 1 minute and can recur over days, months, or rarely years.
Pathophysiology
Two mechanisms are recognized:
-
Canalithiasis (more common) - Otoconia (calcium carbonate crystals) detach from the otolith (utricle macula) and float freely as debris ("canaliths") in the endolymph of the semicircular canal. With head movement, these particles gravitate to the most dependent part of the canal and induce endolymph currents that deflect the cupula, triggering vertigo.
-
Cupulolithiasis - Debris becomes adherent to the cupula itself, making it inappropriately gravity-sensitive.
Canal involved:
- Posterior semicircular canal - ~90% of cases
- Horizontal (lateral) canal - ~10% of cases
- Superior canal - rare
(Adams and Victor's Principles of Neurology, 12th Ed.)
Precipitating Factors
- Post-traumatic (head injury) - ~17% of cases
- Viral neurolabyrinthitis - ~15% of cases
- Osteoporosis - associated with higher frequency
- Often idiopathic
Clinical Features
Typical history:
- Vertigo on lying down, rolling over in bed, bending over and straightening up, or tilting the head back
- Often begins in middle of the night or early morning while shifting during sleep
- Episodes < 1 minute, but may recur for months
Characteristics that define "benign paroxysmal" type:
- Triggered by head position change (not by a sustained position)
- Latency of onset (few seconds after positioning)
- Brief duration (< 30-40 s, usually < 15 s)
- Reversal of nystagmus direction on sitting up
- Fatigability - nystagmus diminishes and disappears with repetition of the maneuver, returns only after prolonged rest
- No associated hearing loss or other ear signs
Diagnosis
Dix-Hallpike Maneuver (for posterior canal BPPV)
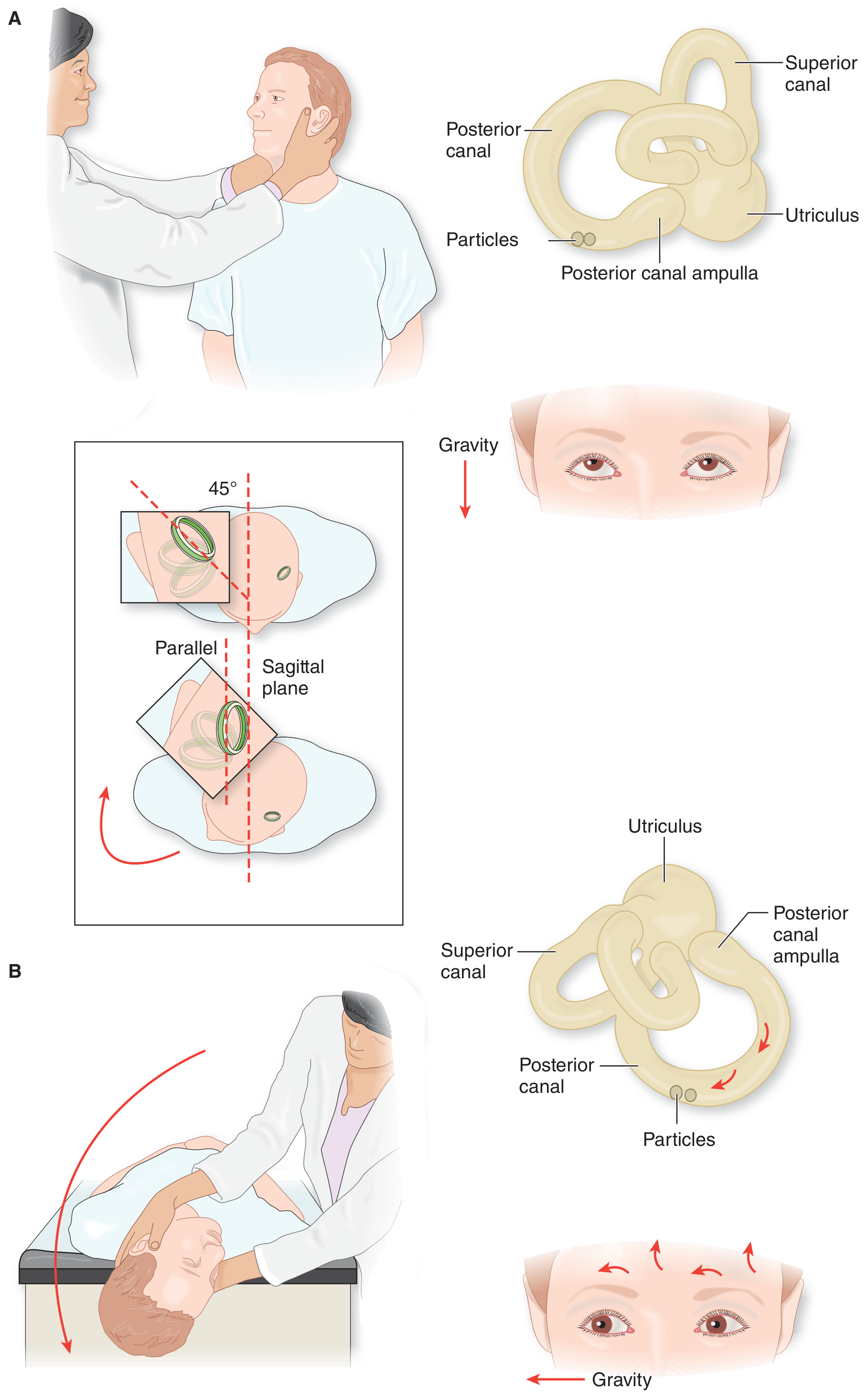
Technique:
- Patient sits upright on examination table
- Head turned 45 degrees toward the ear being tested (aligns posterior canal with the sagittal plane)
- Patient is rapidly brought to recumbency with the head hanging 30-40 degrees over the table edge
Positive test findings:
- Latency of 2-10 seconds
- Vertical-torsional nystagmus: fast phase toward the forehead (upbeating), torsional component beats the top of the eye toward the ground (geotropic torsion)
- The affected ear is the one that is downward when vertigo is elicited
- Nystagmus lasts < 30-40 s and reverses direction on returning to sitting
- Fatigues with repeated testing
For horizontal canal BPPV: standard Dix-Hallpike may be negative. Instead, bring patient supine and turn head to each side. A purely horizontal nystagmus is seen that persists longer than posterior canal BPPV. Geotropic nystagmus = canalithiasis; ageotropic nystagmus = cupulolithiasis.
(Shambaugh Surgery of the Ear; Adams and Victor's Principles of Neurology)
Treatment
1. Epley Canalith Repositioning Maneuver (CRM) - First Line for Posterior Canal Canalithiasis
This is the treatment of choice. The goal is to guide the free-floating debris out of the posterior canal back into the utricle through a series of sequential head movements.
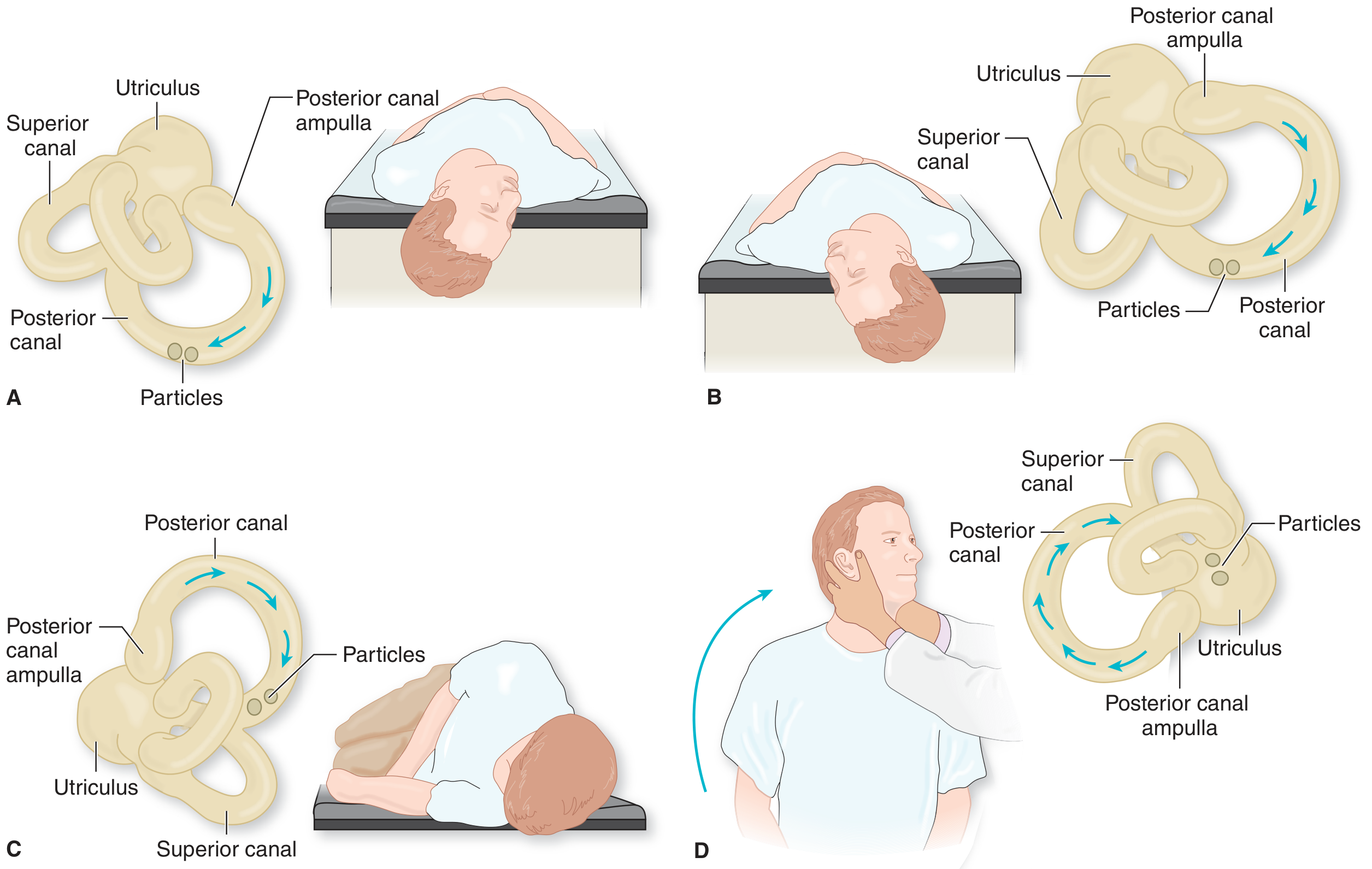
Steps (for right ear BPPV):
- A. Dix-Hallpike position with head rotated 45° right, neck slightly extended - head hanging right
- B. Once nystagmus/vertigo ceases, head rotated 45-60° toward the opposite (left) ear
- C. Patient rolled onto side with head continuing to turn until nearly face-down; held 10-15 s
- D. Head kept turned left as patient is brought back to sitting
Each step separated by ~20 seconds. ~80% respond to a single sequence. A second immediate sequence may help additional cases.
Note: The last face-down step is sometimes incorrectly omitted - it is necessary for complete repositioning. An incomplete maneuver risks converting posterior canal to the harder-to-treat lateral canal variant.
2. Semont (Liberatory) Maneuver - for Cupulolithiasis
Preferred when debris is adherent to the cupula. Patient starts sitting with head turned 45° to one side, then rapidly drops to side-lying on the opposite ear, waits 1 min, then briskly swings 180° to the other side-lying position (nose down), waits 1 min, then returns to sitting.
3. Brandt-Daroff Exercises - Habituation
Used for:
- Persistent BPPV unresolved with CRM or Semont
- Residual vertigo without nystagmus
- Patients who cannot tolerate CRM
Technique: Sit on bed edge, turn head 45° to one side, quickly lie on the opposite side, wait 15 s, sit up, then repeat to the other side. Performed 5 times per set, 3 times daily.
4. Horizontal Canal BPPV
Requires a rolling maneuver - patient rolls from one side to the other in the supine position to reposition the debris from the horizontal canal back into the utricle (Barbecue roll/Lempert maneuver).
5. Surgical (rare)
Reserved for patients with persistent, disabling BPPV refractory to all conservative measures. Options include posterior semicircular canal occlusion or singular neurectomy.
| Treatment | Best for |
|---|---|
| Epley CRM | Posterior canal canalithiasis (most cases) |
| Semont (Liberatory) maneuver | Posterior canal cupulolithiasis |
| Brandt-Daroff exercises | Persistent BPPV; residual symptoms; CRM intolerance |
| Rolling (Barbecue) maneuver | Horizontal canal BPPV |
(Shambaugh Surgery of the Ear, Table 16-4)
Natural History & Prognosis
- Many attacks resolve spontaneously over weeks to months
- In the elderly, attacks may recur over years with no long-term consequences
- ~80% respond to a single Epley maneuver session
- Instruction to avoid head-down position for 24 hrs post-Epley was previously recommended but recent studies suggest it is not necessary
Recent Evidence (2024-2026)
A 2024 systematic review comparing four repositioning maneuvers (PMID 38900988) and a 2025 network meta-analysis (PMID 40098079) confirm the efficacy of particle repositioning maneuvers for posterior canal BPPV, with Epley remaining the standard. A 2026 meta-analysis on repositioning chairs (PMID 41771031) evaluated mechanical assistance devices but found insufficient evidence to recommend them over manual maneuvers routinely.
Sources: Adams and Victor's Principles of Neurology 12th Ed. - p. 322-324 | Shambaugh Surgery of the Ear - p. 336-337
This is a shared conversation. Sign in to Orris to start your own chat.