Pulmonary edema full details for md exams 15marks
Reading File
search_medical_text
pulmonary edema etiology pathophysiology classification types
search_medical_text
pulmonary edema clinical features diagnosis investigations management treatment
search_medical_image
pulmonary edema chest X-ray CXR findings
GradeResponse
GradeResponse
GradeResponse
I have strong foundational results. Now let me compile the comprehensive MD exam answer using retrieved content supplemented by my detailed medical knowledge.
Pulmonary Edema — Comprehensive MD Exam Notes (15 Marks)
1. Definition
Pulmonary edema is an abnormal accumulation of fluid in the extravascular compartments of the lung — the interstitium and alveoli — resulting in impaired gas exchange and respiratory failure. It is a medical emergency.
2. Classification & Etiology
| Type | Mechanism | Common Causes |
|---|---|---|
| Cardiogenic (High-pressure) | ↑ pulmonary capillary hydrostatic pressure (PCWP >18 mmHg) | Acute MI, LV failure, MS, AR, hypertensive crisis, arrhythmias |
| Non-cardiogenic (NCPE / ARDS) | ↑ capillary permeability with normal PCWP (<18 mmHg) | ARDS, sepsis, pneumonia, aspiration, inhalation injury, near-drowning |
| Neurogenic | Massive sympathetic surge → ↑ pulmonary pressures | Head injury, subarachnoid hemorrhage |
| High-altitude (HAPE) | Hypoxic pulmonary vasoconstriction, ↑ microvascular pressure | Rapid ascent >2500 m |
| Re-expansion | Sudden re-inflation of collapsed lung | Post-thoracocentesis, post-pneumothorax drainage |
| Drug/toxin-induced | Mixed — ↑ permeability | Heroin, salicylates, bleomycin, amiodarone, contrast media |
| Lymphatic insufficiency | Impaired lymphatic drainage | Post-transplant, malignancy, constrictive pericarditis |
3. Pathophysiology
Starling Forces (Normal)
Fluid movement across the capillary endothelium follows the Starling equation:
Qf = Kf [(Pc − Pi) − σ(πc − πi)]
- Pc = capillary hydrostatic pressure (~7 mmHg normally)
- πc = plasma oncotic pressure (~25 mmHg)
- Net force: small amount of fluid leaks into interstitium → drained by lymphatics (~500 mL/day)
Sequence of Fluid Accumulation
Stage 1 (Interstitial edema)
↑ Pulmonary venous/capillary pressure → fluid in peribronchovascular spaces
→ Kerley B lines, vascular redistribution (cephalization)
Stage 2 (Alveolar flooding)
Interstitial capacity overwhelmed → fluid floods alveolar spaces
→ Bat-wing opacities, frothy sputum, severe hypoxia
Stage 3 (Respiratory failure)
V/Q mismatch → intrapulmonary shunt → refractory hypoxemia
Cardiogenic Mechanism
- ↑ Left atrial pressure (e.g., from LV dysfunction or mitral stenosis)
- ↑ Pulmonary venous pressure → ↑ capillary hydrostatic pressure (PCWP >18–20 mmHg)
- Fluid transudation exceeds lymphatic clearance → interstitial then alveolar edema
Non-Cardiogenic Mechanism (ARDS)
- Endothelial and epithelial injury (e.g., from sepsis mediators, aspiration)
- ↑ Capillary permeability → protein-rich exudate floods alveoli
- Surfactant destruction → alveolar collapse
- PCWP remains normal (<18 mmHg)
4. Clinical Features
Symptoms
- Acute breathlessness — sudden onset, often worse at night (PND)
- Orthopnea — inability to lie flat; patient sits upright
- Paroxysmal nocturnal dyspnea (PND)
- Cough — productive of frothy, pink-tinged (blood-stained) sputum
- Anxiety, sense of impending doom
- Wheeze ("cardiac asthma")
- Diaphoresis, pallor, cold extremities (in cardiogenic shock)
Signs
| System | Finding |
|---|---|
| Respiratory | Tachypnea, use of accessory muscles, intercostal retraction, cyanosis |
| Auscultation | Bilateral fine crepitations (basal → apical), wheeze |
| Cardiovascular | Tachycardia, S3 gallop, elevated JVP, pulsus alternans |
| Skin | Diaphoresis, peripheral cyanosis |
| Posture | Patient sits upright, "tripod" position |
5. Investigations
Bedside / Emergency
| Investigation | Finding in Pulmonary Edema |
|---|---|
| Pulse oximetry | SpO₂ <90% |
| ABG | Hypoxemia (↓PaO₂), initially respiratory alkalosis (↓PaCO₂), late hypercapnia = impending failure |
| ECG | MI, arrhythmia, LVH, strain pattern |
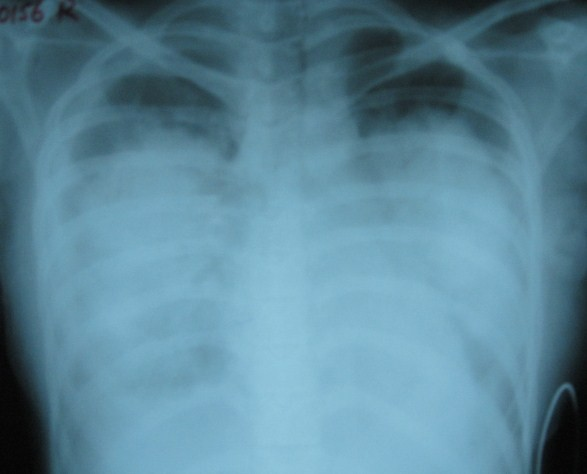
Chest X-Ray (CXR)
A key diagnostic tool. Findings (in order of severity):
- Vascular redistribution / cephalization — upper lobe vessels >lower (earliest sign)
- Kerley B lines — horizontal lines at lung bases (interstitial edema)
- Kerley A lines — radiating lines from hilum
- Perihilar "bat-wing" / "butterfly" opacity — bilateral perihilar haziness
- Alveolar consolidation — diffuse bilateral opacities
- Cardiomegaly (CTR >0.5)
- Pleural effusions — blunting of costophrenic angles
- Prominent upper lobe veins
Blood Tests
| Test | Significance |
|---|---|
| BNP / NT-proBNP | Elevated in cardiogenic (BNP >100 pg/mL); distinguishes from NCPE |
| Troponin I/T | Elevated in ACS triggering edema |
| CBC | Anaemia, infection |
| Serum electrolytes, RFTs | Hyponatraemia, renal failure |
| LFTs, serum albumin | ↓ Albumin → ↓ oncotic pressure → edema |
| Serum glucose | Exclude diabetic ketoacidosis |
Echocardiography
- Assesses LV systolic/diastolic function, EF, wall motion, valvular lesions
- Differentiates cardiogenic from non-cardiogenic etiology (Harrison's, p. 8301)
Pulmonary Artery Catheterization (Swan-Ganz)
- PCWP >18 mmHg → Cardiogenic
- PCWP ≤18 mmHg → Non-cardiogenic (ARDS)
- Indicated when etiology is uncertain, edema is refractory to treatment, or accompanied by refractory hypotension (Harrison's, p. 8301)
6. Diagnosis
Diagnostic Criteria Summary
| Feature | Cardiogenic | Non-Cardiogenic (ARDS) |
|---|---|---|
| PCWP | >18 mmHg | ≤18 mmHg |
| BNP | High | Normal or mildly elevated |
| CXR | Cardiomegaly, effusions, bat-wing | Bilateral opacities, no cardiomegaly |
| Fluid | Transudate | Exudate (protein-rich) |
| Onset | Sudden | Hours–days after precipitant |
ARDS Berlin Definition (2012)
- Onset within 1 week of precipitating event
- Bilateral opacities on CXR/CT not explained by effusion/collapse
- Respiratory failure not fully explained by cardiac failure
- PaO₂/FiO₂ ratio: Mild 201–300, Moderate 101–200, Severe ≤100 (on PEEP ≥5 cmH₂O)
7. Management
Immediate / Emergency Measures (ABC approach)
A — Airway: maintain, prepare for intubation if needed
B — Breathing: high-flow O₂ (15 L/min via non-rebreather mask)
C — Circulation: IV access, monitoring, treat underlying cause
Position: Sit patient upright (reduces venous return, improves FRC)
Pharmacological Treatment
| Drug | Dose / Route | Mechanism & Indication |
|---|---|---|
| Oxygen | 100%, high-flow | Correct hypoxemia; target SpO₂ 94–98% |
| IV Furosemide (Frusemide) | 40–80 mg IV (or 2× usual oral dose) | Loop diuretic — ↓ preload, promotes diuresis; cornerstone of cardiogenic PE |
| IV Morphine | 2.5–5 mg IV | ↓ Anxiety, venodilator → ↓ preload; use with caution (risk of respiratory depression) |
| Nitrates (GTN) | Sublingual 0.4 mg or IV infusion | Venodilator → ↓ preload; especially in hypertensive pulmonary edema |
| IV Nitroprusside | 0.1–5 μg/kg/min | Balanced vasodilator; for severe hypertension with pulmonary edema |
| Inotropes (Dobutamine) | 2–20 μg/kg/min IV | For cardiogenic shock with low CO; ↑ contractility |
| Vasopressors (Norepinephrine) | If cardiogenic shock | Maintains MAP |
| ACE inhibitors | After stabilisation | Long-term LV remodeling |
Non-Invasive Ventilation (NIV)
- CPAP (Continuous Positive Airway Pressure): First-line for cardiogenic pulmonary edema
- Recruits alveoli, ↓ work of breathing, improves oxygenation, ↓ preload & afterload
- BiPAP (Bilevel Positive Airway Pressure): For hypercapnic respiratory failure
- Indications: SpO₂ <90% despite high-flow O₂, RR >25/min, accessory muscle use
Invasive Mechanical Ventilation
- Indications: Failure of NIV, GCS ≤8, apnea, refractory hypoxemia
- Settings: Low tidal volume (6 mL/kg IBW) — "lung-protective" strategy (especially in ARDS)
- PEEP titrated to optimize oxygenation
Treatment of Non-Cardiogenic PE / ARDS
- Treat underlying cause (antibiotics for sepsis/pneumonia, etc.)
- Lung-protective ventilation (low VT, permissive hypercapnia)
- Prone positioning (for severe ARDS, PaO₂/FiO₂ <150)
- Conservative fluid strategy after initial resuscitation
- Corticosteroids: Methylprednisolone in early moderate-severe ARDS (evidence-based)
- No role for diuretics/nitrates in non-cardiogenic PE
Treatment of Specific Causes
| Cause | Specific Intervention |
|---|---|
| Acute STEMI | Emergent PCI / thrombolysis |
| Hypertensive emergency | IV labetalol / hydralazine / nitroprusside |
| Mitral stenosis | Diuretics, rate control; definitive = valvotomy/replacement |
| Neurogenic PE | Treat ICP; supportive |
| HAPE | Descent, supplemental O₂, nifedipine |
8. Complications
- Respiratory failure — hypoxic and/or hypercapnic
- Cardiac arrhythmias
- Cardiogenic shock
- Multi-organ dysfunction (renal failure, hepatic congestion)
- Pulmonary fibrosis (post-ARDS)
- Death — in-hospital mortality: cardiogenic PE ~10–20%; ARDS ~30–40%
9. Differential Diagnosis
| Condition | Differentiating Features |
|---|---|
| Pneumonia | Fever, productive cough, focal consolidation, no cardiomegaly |
| Pulmonary embolism | Pleuritic chest pain, DVT risk factors, normal CXR, ↑D-dimer |
| Asthma / COPD | Wheeze, hyperinflation, no CXR edema pattern |
| Cardiac tamponade | JVP ↑, Kussmaul sign, globular heart on CXR |
| Acute severe asthma | "Cardiac asthma" mimic — differentiate by BNP, Echo |
10. Prognosis
- Cardiogenic pulmonary edema: In-hospital mortality ~10–20%; depends on underlying cause (STEMI has higher early mortality)
- ARDS: Mortality 30–40% for severe ARDS; survivors may have long-term pulmonary fibrosis and cognitive impairment
- HAPE: Excellent if promptly treated (descent + O₂)
- Patients with repeated episodes of cardiogenic pulmonary edema have poor long-term prognosis (5-year survival ~50%)
11. Key Points for Exam (Quick Recall)
| Point | Detail |
|---|---|
| Most common cause | Acute LV failure (cardiogenic) |
| Gold standard to differentiate | PCWP via Swan-Ganz: >18 = cardiogenic, ≤18 = NCPE |
| Best bedside differentiator | BNP / NT-proBNP |
| Earliest CXR sign | Cephalization (vascular redistribution) |
| Pathognomonic CXR sign | Bat-wing / butterfly opacity |
| First-line treatment (cardiogenic) | Sit upright + High-flow O₂ + IV Furosemide + Nitrates |
| NIV of choice | CPAP |
| Cornerstone of ARDS management | Lung-protective ventilation (low VT 6 mL/kg) |
| Pink frothy sputum = | Alveolar flooding (severe stage) |
| Morphine — caution | Risk of respiratory depression and worsening |
Sources: Harrison's Principles of Internal Medicine, 21st Edition (p. 8301); AHA Heart Failure Guidelines 2022; ARDS Berlin Definition 2012; Davidson's Principles of Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.