Dowm syndrome clinical features and management in deatil
Reading File
search_medical_text
Down syndrome trisomy 21 clinical features physical findings
search_medical_text
Down syndrome management complications cardiac intellectual disability
search_medical_image
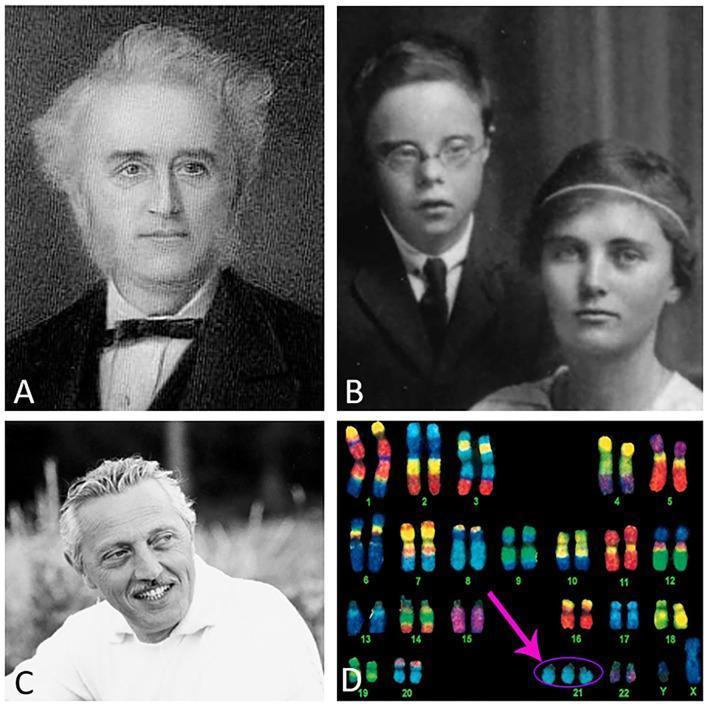
Down syndrome facial features karyotype
GradeResponse
GradeResponse
GradeResponse
The retrieval was limited, so I'll synthesize a comprehensive answer from my medical knowledge combined with retrieved content.
Down Syndrome (Trisomy 21) — Clinical Features & Management
1. Genetics & Epidemiology
| Feature | Detail |
|---|---|
| Incidence | ~1 in 700 live births (most common chromosomal disorder) |
| Prevalence | Most common genetic cause of intellectual disability |
| Maternal age risk | Increases sharply after age 35 (1:385 at 35 → 1:30 at 45) |
Chromosomal Subtypes
| Type | Frequency | Mechanism |
|---|---|---|
| Free trisomy 21 | ~95% | Nondisjunction during meiosis (usually maternal meiosis I) |
| Robertsonian translocation | ~4% | Chromosome 21 attached to another (usually chr 14); hereditary risk |
| Mosaic trisomy 21 | ~1% | Nondisjunction in early mitosis; milder phenotype |
Key point: Robertsonian translocation does NOT increase with maternal age and may be inherited — parents must be karyotyped to assess recurrence risk.
2. Clinical Features
2.1 Dysmorphic / Physical Features
Craniofacial:
- Flat facial profile (midface hypoplasia)
- Brachycephaly (flat occiput)
- Upward-slanting palpebral fissures
- Epicanthic folds
- Brushfield spots (white/grey speckles on iris periphery)
- Flat nasal bridge, small nose
- Small ears, often low-set
- Protruding tongue (relative macroglossia + small oral cavity)
- Short neck with excess nuchal skin
Limbs & Hands:
- Short stature (adult height ~150 cm men, ~138 cm women)
- Short, broad hands
- Single palmar (Simian) crease
- Clinodactyly (incurved 5th finger)
- Wide gap between 1st and 2nd toes ("sandal gap")
- Hypotonia (generalized, prominent in infancy)
- Joint hypermobility/laxity
Other:
- Low birth weight
- Excess skin at nape of neck in neonates
2.2 Neurodevelopmental Features
| Domain | Finding |
|---|---|
| Intellectual disability | Mild to moderate (IQ typically 35–70); severe in ~10% |
| Speech & language | Expressive > receptive delay; dysarthria common |
| Motor development | Delayed (walking at ~2 years on average) |
| Behavior | Generally sociable, affectionate; may show stubbornness, repetitive behaviors |
| ADHD | Present in ~6–10% |
| Autism Spectrum Disorder | ~5–10%; higher in males |
2.3 Systemic Complications
Cardiovascular (40–50%)
- AVSD (atrioventricular septal defect) — most characteristic; ~40% of cardiac defects
- VSD (~32%)
- ASD (~10%)
- Tetralogy of Fallot (~6%)
- PDA
- Early pulmonary hypertension if unrepaired (Eisenmenger syndrome risk)
Gastrointestinal (5–15%)
- Duodenal atresia ("double bubble" sign on X-ray — nearly pathognomonic)
- Hirschsprung disease (~2%)
- Tracheoesophageal fistula
- Pyloric stenosis
- Imperforate anus
- Celiac disease (~5–7%)
Hematological
- Transient Myeloproliferative Disorder (TMD): ~10% of neonates; usually resolves spontaneously
- Acute Megakaryoblastic Leukemia (AMKL/AML-M7): ~1–2%; risk 150× higher than general population
- ALL: 20× increased risk
- Polycythemia in neonates
Endocrine
- Hypothyroidism (congenital or acquired — Hashimoto's) in ~15–20%
- Diabetes mellitus (type 1 and 2)
- Obesity — very common in older children/adults
Musculoskeletal
- Atlantoaxial instability (~15%): subluxation risk; may cause cord compression
- Hip instability/dislocation
- Patellar instability
- Flat feet (pes planus)
Respiratory
- Obstructive sleep apnea (OSA) — very common (~50–75%)
- Recurrent otitis media with effusion
- Subglottic stenosis
- Increased susceptibility to respiratory infections
Ophthalmological
- Refractive errors (very common — ~70%)
- Strabismus (~30%)
- Nystagmus
- Cataracts (congenital or acquired)
- Keratoconus
Hearing
- Conductive hearing loss (very common — ~50–70%) due to chronic serous otitis media
- Sensorineural hearing loss (~20%)
Neurological
- Seizures (~8–13%)
- Infantile spasms
- Alzheimer's disease: virtually universal neuropathological changes by age 40; clinical dementia in ~50% by age 60 (linked to APP gene on chromosome 21)
Dermatological
- Dry skin, xerosis
- Alopecia areata
- Folliculitis
3. Prenatal Diagnosis
Screening
| Test | Timing | Markers |
|---|---|---|
| First trimester combined | 11–13+6 weeks | Nuchal translucency (NT) + β-hCG + PAPP-A |
| Second trimester quad screen | 15–20 weeks | AFP↓, β-hCG↑, uE3↓, inhibin A↑ |
| Cell-free DNA (cfDNA/NIPT) | ≥10 weeks | Most sensitive/specific (DR ~99%, FPR <0.1%) |
Diagnostic (Confirmatory)
- Chorionic villus sampling (CVS): 10–13 weeks
- Amniocentesis: 15–20 weeks
- Karyotype or chromosomal microarray on obtained cells
4. Management
Down syndrome requires multidisciplinary, lifelong care. Management is organized below by domain and age.
4.1 Neonatal Period
- Cardiac echo: all newborns — ~50% have CHD, often asymptomatic at birth
- Feeding support: for hypotonia and poor suck
- Thyroid function (TSH, T4) at birth and at 6 months
- Hearing screen (OAE/ABR)
- Ophthalmology referral
- Karyotype confirmation
- Genetic counseling for family
- Early intervention referral
4.2 Cardiovascular Management
- Echocardiogram in all neonates
- Surgical repair of CHD (AVSD repair typically at 3–6 months before pulmonary hypertension establishes)
- Cardiology follow-up lifelong
- Endocarditis prophylaxis per guidelines
4.3 Neurodevelopmental Interventions
| Therapy | Target | Timing |
|---|---|---|
| Early intervention | Global development | Birth to 3 years |
| Speech-language therapy | Language, feeding, articulation | As soon as delay identified |
| Occupational therapy | Fine motor, ADLs | Early childhood onward |
| Physical therapy | Gross motor, hypotonia | Infancy onward |
| Special education / IEP | Cognitive, academic | School age |
| Augmentative & alternative communication (AAC) | Non-verbal or limited verbal children | As needed |
- Inclusion in mainstream education with appropriate support improves outcomes
- Behavioral therapy for ADHD/ASD comorbidities
4.4 Endocrine & Metabolic
- Thyroid screening: at birth, 6 months, 12 months, then annually
- Treatment with levothyroxine for hypothyroidism
- Dietary counseling and physical activity for obesity prevention/management
- Bone density monitoring in adults
4.5 Atlantoaxial Instability
- Clinical surveillance for symptoms (neck pain, weakness, gait change, torticollis)
- Cervical spine X-rays (flexion/extension views) in symptomatic patients or before contact sports/surgery
- Atlanto-dens interval (ADI) >4.5 mm = abnormal; >7–10 mm = surgical concern
- Restrict contact sports/gymnastics if symptomatic instability
- Neurosurgical referral for myelopathy
4.6 Hearing & ENT
- Hearing screen at birth and annual audiological assessment
- Myringotomy + grommets (PE tubes) for recurrent serous otitis media
- Hearing aids when indicated
- Adenotonsillectomy for OSA (first-line surgical treatment)
- Polysomnography recommended for all children with Down syndrome (~2–4 years)
4.7 Ophthalmology
- Annual ophthalmology review from infancy
- Glasses for refractive errors
- Patching/surgery for strabismus
- Slit lamp for cataracts/keratoconus
4.8 Hematological Surveillance
| Condition | Action |
|---|---|
| TMD (neonatal) | Usually observe; low-dose cytarabine for symptomatic/life-threatening cases |
| AML/ALL | Prompt oncology referral; Down syndrome-associated leukemia often MORE responsive to chemotherapy (favorable prognosis for AMKL) |
| Polycythemia | Partial exchange transfusion if symptomatic |
4.9 Gastrointestinal
- Surgical correction of duodenal atresia, Hirschsprung disease, TEF in neonatal period
- Screen for celiac disease (anti-tissue transglutaminase IgA + total IgA) at ~2–3 years and if symptomatic
- Constipation management (common due to hypotonia + Hirschsprung)
4.10 Alzheimer's Disease & Adult Neurological Care
- Virtually all adults with Down syndrome develop Alzheimer's pathology by age 40
- Clinical dementia onset typically in 5th–6th decade
- Baseline cognitive and adaptive functioning assessment at ~30 years
- Annual monitoring for cognitive decline from age 40
- Cholinesterase inhibitors (donepezil) may offer modest symptomatic benefit
- Support for caregivers and advance care planning
4.11 Mental Health
- Screen for depression, anxiety, ADHD, ASD
- Psychotherapy, behavioral interventions
- Pharmacotherapy when needed (SSRIs for depression/anxiety; stimulants for ADHD with monitoring)
5. Health Surveillance Summary (by Age)
| Age | Key Checks |
|---|---|
| Neonate | Echo, TSH, hearing, karyotype, feeding assessment, ophthalmology |
| 6 months | TSH, developmental review, audiology, ophthalmology |
| 1–2 years | TSH, audiology, ophthalmology, celiac screen, cervical spine if concerns |
| 3–5 years | Polysomnography (OSA screen), ENT, development |
| School age | Annual TSH, audiology, ophthalmology, behavior/mental health, BMI |
| Adolescence | Pubertal development, contraception counseling, vocational planning |
| Adults (30+) | Baseline cognitive assessment, annual TSH, bone density, Alzheimer's surveillance |
6. Prognosis & Quality of Life
- Median life expectancy has improved dramatically: ~60 years today (vs. 25 years in 1983)
- Many adults live semi-independently or with supported living
- Meaningful employment is achievable with appropriate vocational support
- Recurrence risk: ~1% for free trisomy 21 + age-related risk; up to 100% for certain translocations (e.g., 21;21 translocation parent)
Key References: Nelson Textbook of Pediatrics | Smith's Recognizable Patterns of Human Malformation | AAP Health Supervision Guidelines for Children with Down Syndrome (2022) | GeneReviews — Trisomy 21
This is a shared conversation. Sign in to Orris to start your own chat.