Proton Pump Inhibitors, H2 blockers and Antacids pharmacology detailed notes
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a complete, detailed set of pharmacology notes. Here is the full answer:
Pharmacology Notes: PPIs, H2 Blockers, and Antacids
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics; Lippincott Illustrated Reviews: Pharmacology, 8e; Katzung's Basic and Clinical Pharmacology, 16e
Gastric Acid Physiology - The Foundation
Understanding these drugs requires knowing how acid is made. Three stimuli drive parietal cells to secrete H⁺:
- Acetylcholine (via M3 muscarinic receptors) - Ca²⁺-dependent pathway
- Histamine (via H2 receptors on parietal cells) - cAMP/PKA pathway
- Gastrin (via CCK2 receptors) - Ca²⁺-dependent pathway
All three pathways converge on activation of the H⁺/K⁺-ATPase (proton pump), which exchanges H⁺ for K⁺ across the apical membrane of the parietal cell into the gastric lumen. The proton pump is the final common effector of acid secretion.
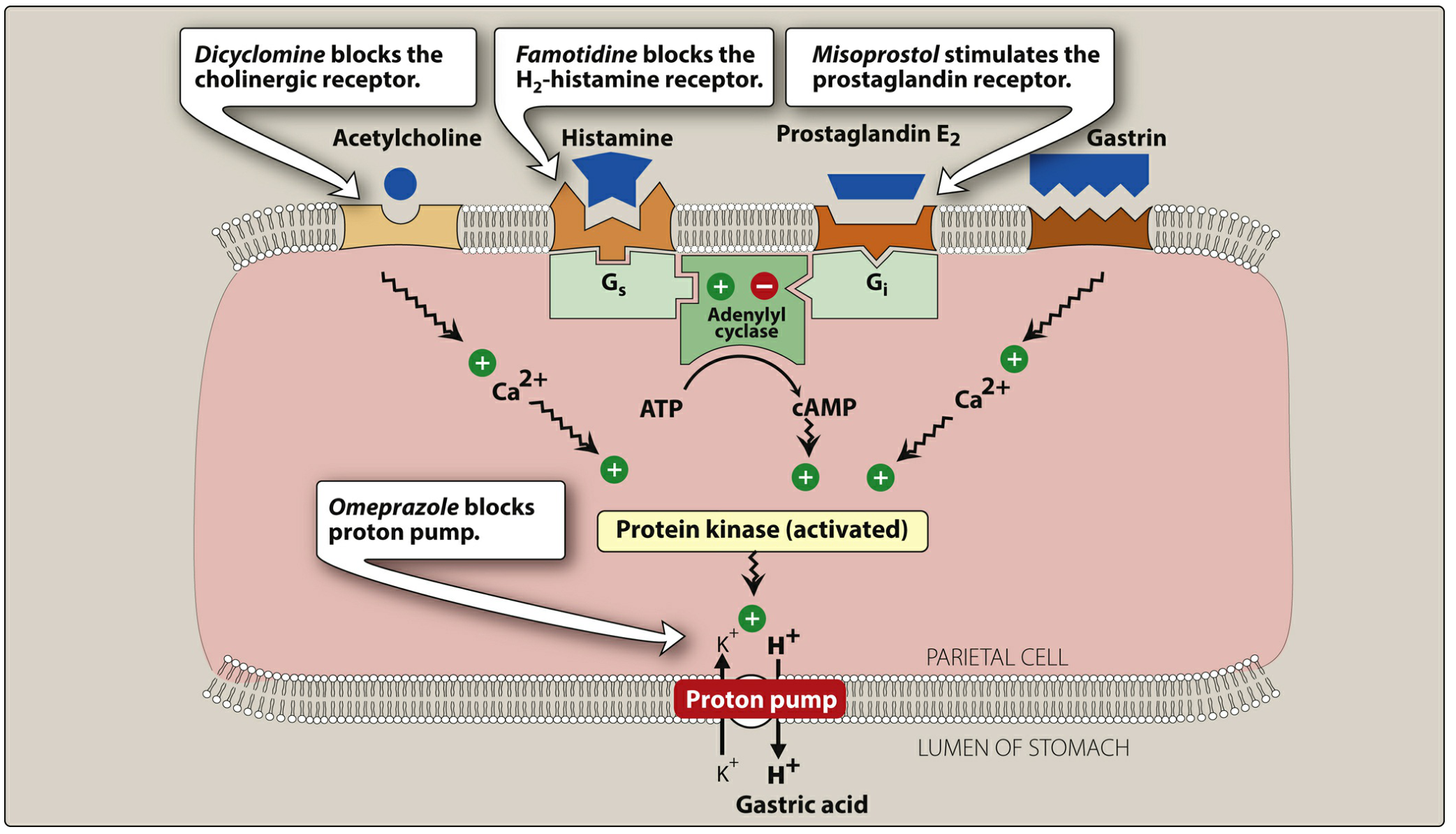
Figure: Gastric acid secretion by the parietal cell, showing sites of drug action - Lippincott Illustrated Reviews: Pharmacology
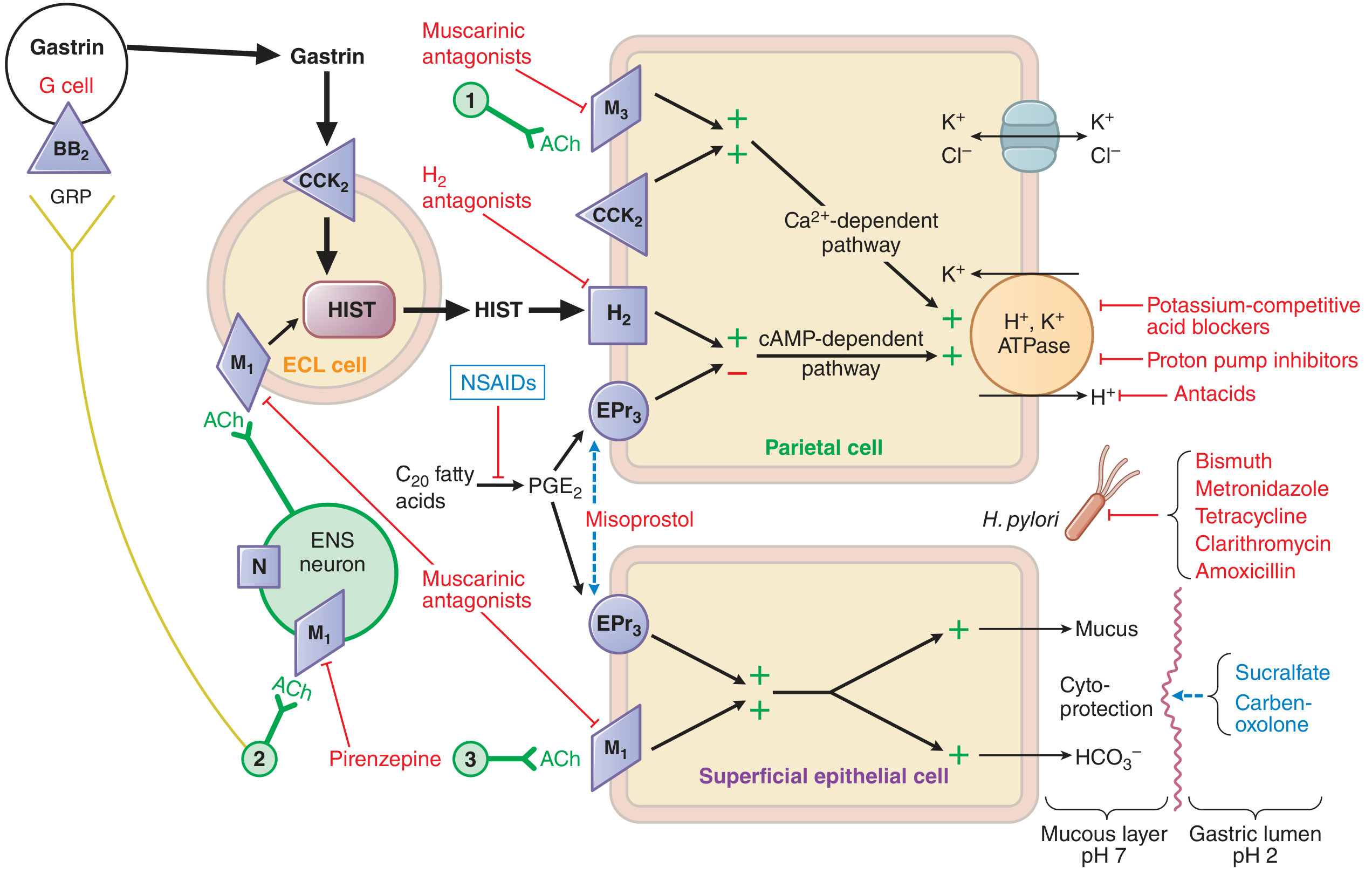
Figure: Pharmacological basis of therapy for acid-peptic disorders - Goodman & Gilman's
PART 1: PROTON PUMP INHIBITORS (PPIs)
Drugs in Class
| Generic Name | Brand Name |
|---|---|
| Omeprazole | Prilosec |
| Esomeprazole (S-isomer of omeprazole) | Nexium |
| Lansoprazole | Prevacid |
| Dexlansoprazole (R-enantiomer of lansoprazole) | Dexilant |
| Pantoprazole | Protonix |
| Rabeprazole | Aciphex |
All PPIs have equivalent efficacy at comparable doses.
Mechanism of Action
PPIs are prodrugs - they require acid activation to work.
Step-by-step activation:
- Administered as acid-labile prodrugs (enteric-coated or delayed-release to survive stomach transit)
- Absorbed in the small intestine → enter systemic circulation
- Diffuse into parietal cell secretory canaliculi (the most acidic compartment in the body, pH ~1)
- Protonation converts the prodrug into a tetracyclic sulfenamide (active form)
- The sulfenamide forms covalent disulfide bonds with cysteine residues on the α-subunit of H⁺/K⁺-ATPase
- This irreversibly inactivates the proton pump
Because the bond is irreversible, acid suppression persists until new pump protein is synthesized (~18-24 hours). This is why the duration of action far exceeds the plasma half-life (t½ ~1-2 hours, but effect lasts ~24 hours).
"The most potent suppressors of gastric acid secretion are inhibitors of the gastric H⁺,K⁺-ATPase or proton pump. These drugs diminish the daily production of acid (basal and stimulated) by 80% to 95%." - Goodman & Gilman's
Pharmacokinetics (ADME)
| Property | Detail |
|---|---|
| Absorption | Small intestine (enteric coating protects from gastric acid) |
| Timing | Give 30 min before the first meal - food stimulates acid which activates PPIs; fasting increases H⁺/K⁺-ATPase expression |
| Protein binding | Highly protein-bound |
| Metabolism | Extensively by hepatic CYP2C19 and CYP3A4 |
| Half-life | ~1-2 hours (much shorter than duration of action) |
| CYP2C19 genetics | Asians/Oceanians: 25-60% are poor metabolizers → heightened efficacy/toxicity; Caucasians/Africans: ~15% |
| Second-generation PPIs | Dexlansoprazole, esomeprazole, and rabeprazole have less dependence on CYP2C19 |
| IV forms | Esomeprazole sodium, omeprazole sodium, pantoprazole |
Therapeutic Uses
- Peptic ulcer disease (PUD) - duodenal and gastric ulcers; also used in H. pylori triple/quadruple therapy regimens
- GERD and erosive esophagitis - first-line agent
- Zollinger-Ellison syndrome - hypersecretory state; high-dose PPIs are required
- NSAID-induced ulcer prevention - superior to H2 blockers
- Stress ulcer prophylaxis in ICU
- GI bleeding - IV PPIs used to stabilize clots by raising gastric pH
- Barrett's esophagus - long-term maintenance
Adverse Effects
| Effect | Mechanism / Notes |
|---|---|
| Headache, diarrhea, nausea | Most common GI side effects |
| Hypomagnesemia | Long-term use; monitor Mg²⁺, especially with diuretics |
| Vitamin B12 deficiency | Reduced gastric acid impairs B12 absorption (especially long-term, high-dose) |
| Iron, Ca²⁺ malabsorption | Reduced acid decreases solubility of non-heme iron and Ca²⁺ salts |
| Bone fractures (increased risk) | Multifactorial; Ca²⁺ malabsorption plays a role |
| Clostridium difficile infection | Reduced acid removes a barrier against ingested bacteria |
| Hypergastrinemia | Acid suppression removes negative feedback on gastrin release → rebound hypersecretion on stopping |
| ECL cell hyperplasia / fundic gland polyps | Consequence of hypergastrinemia |
| Community-acquired pneumonia | Reduced gastric acid may allow colonization |
| Rebound acid hypersecreretion | Occurs on discontinuation after prolonged use |
| Interstitial nephritis | Rare; all PPIs |
Drug Interactions
| Interaction | Mechanism |
|---|---|
| Clopidogrel | Omeprazole and esomeprazole inhibit CYP2C19, reducing clopidogrel activation → reduced antiplatelet effect. Boxed warning: avoid omeprazole/esomeprazole with clopidogrel. Use pantoprazole or an H2 blocker instead |
| Warfarin | Esomeprazole, lansoprazole, omeprazole, rabeprazole inhibit CYP-mediated warfarin clearance |
| Methotrexate | PPIs competitively inhibit methotrexate renal elimination → toxic levels |
| Atazanavir/nelfinavir | Reduced absorption due to raised pH |
| Ketoconazole, ampicillin esters, iron salts | Require acid for optimal absorption |
| Diazepam | Esomeprazole and omeprazole inhibit metabolism |
| Theophylline, imipramine | Omeprazole induces CYP1A2 → increased clearance |
| Phenytoin, disulfiram | Omeprazole inhibits CYP2C19 → decreased clearance |
PART 2: H2 RECEPTOR ANTAGONISTS (H2 Blockers)
Drugs in Class
| Generic Name | Brand Name | Status |
|---|---|---|
| Famotidine | Pepcid | Available |
| Cimetidine | Tagamet | Available (limited use) |
| Nizatidine | Axid | Limited availability |
| Ranitidine | Zantac | Withdrawn from market (NDMA contamination) |
"Cimetidine was the first H2 receptor antagonist. However, its utility is limited by its adverse effect profile and drug-drug interactions." - Lippincott Illustrated Reviews
Mechanism of Action
H2 blockers are competitive, reversible antagonists at histamine H2 receptors located on the basolateral membrane of parietal cells.
- Block the H2 receptor → reduce cAMP production → reduce protein kinase A activation → reduced H⁺/K⁺-ATPase stimulation
- They are selective for H2 receptors; no effect on H1 receptors
- Because histamine acts as a "permissive" stimulant that amplifies acetylcholine and gastrin signaling, H2 blockade dampens responses to all three stimuli (not just histamine alone)
- Suppress basal and nocturnal acid secretion most effectively (~70% reduction over 24 hours)
- Less potent than PPIs at suppressing meal-stimulated acid
Pharmacokinetics (ADME)
| Property | Cimetidine | Ranitidine | Famotidine | Nizatidine |
|---|---|---|---|---|
| Onset (oral) | ~1-3 h | ~1-3 h | ~1-3 h | ~1-3 h |
| Duration | 4-5 h (IV) | 6-8 h (IV) | 10-12 h (IV) | ~10 h |
| t½ | ~1-2 h | ~2-3 h | ~2.5-3.5 h | ~1-2 h |
| Elimination | Mainly renal (filtration + tubular secretion) | Renal | Renal | Renal |
| Protein binding | Low | Low | Low | Low |
| Hepatic metabolism | 25-35% | <20% | <10% | <15% |
Key point: Dose reduction required in renal impairment for all agents. Neither hemodialysis nor peritoneal dialysis significantly clears these drugs. Liver disease is generally NOT an indication for dose adjustment.
IV dosing (from Goodman & Gilman's Table 53-1):
| Route | Cimetidine | Famotidine |
|---|---|---|
| Intermittent bolus | 300 mg every 6-8 h | 20 mg every 12 h |
| Continuous infusion | 37.5-100 mg/h | 1.7 mg/h |
Therapeutic Uses
- Peptic ulcer disease: All H2 blockers equally effective for duodenal and gastric ulcers. Evening dosing adequate for most cases (because nocturnal acid suppression is key for duodenal ulcer healing). Must combine with antibiotics if H. pylori present - H2 blockers alone do not prevent recurrence.
- GERD / Heartburn: Effective for mild-moderate GERD; slower onset than antacids (up to 45 minutes). PPIs are now preferred.
- Acute stress ulcer prophylaxis: IV infusion in ICU patients. Tolerance may develop with continuous use.
- Zollinger-Ellison syndrome: Less effective than PPIs; rarely used now.
- Over-the-counter heartburn: Still widely available OTC (particularly famotidine).
Adverse Effects
H2 blockers have an excellent safety record overall.
Cimetidine-specific adverse effects (most problematic of the class):
- Antiandrogenic effects: Inhibits dihydrotestosterone binding to androgen receptors → gynecomastia, impotence, decreased libido in men; galactorrhea in women
- CNS effects: Confusion, dizziness, headache (especially in elderly and critically ill)
- Elevated serum creatinine: Blocks tubular secretion of creatinine (does not reflect true GFR change)
- Most drug interactions of all H2 blockers (CYP inhibition)
Class effects:
- Tolerance: Tachyphylaxis develops within days to weeks of continuous use (receptor upregulation/desensitization) - a limitation for long-term efficacy
- Headache, diarrhea (uncommon)
- Thrombocytopenia (rare)
- Interstitial nephritis (rare)
Drug Interactions
Cimetidine is by far the most problematic:
- Inhibits CYP1A2, CYP2C9, CYP2D6, CYP3A4 → reduces metabolism of:
- Warfarin, theophylline, phenytoin, carbamazepine, lidocaine, quinidine, beta-blockers, tricyclic antidepressants, calcium channel blockers, opioids
- Inhibits renal tubular secretion of creatinine, procainamide, metformin
All H2 blockers:
- May reduce absorption of drugs requiring acidic pH (ketoconazole, itraconazole)
- Antacids can reduce absorption of H2 blockers if taken simultaneously (separate by at least 1 hour)
Tolerance (Tachyphylaxis)
A clinically important limitation: tolerance develops to H2 blockers within days of regular use. This does NOT occur with PPIs. The mechanism involves compensatory upregulation of H2 receptors and/or enhanced responsiveness to gastrin and acetylcholine pathways. This is why PPIs are now preferred for healing ulcers and erosive GERD.
PART 3: ANTACIDS
Drugs in Class
| Drug | Formula | Key Properties |
|---|---|---|
| Aluminum hydroxide | Al(OH)₃ | Causes constipation; slower onset |
| Magnesium hydroxide ("Milk of Magnesia") | Mg(OH)₂ | Causes diarrhea |
| Calcium carbonate ("Tums") | CaCO₃ | Fast onset; also used as Ca²⁺ supplement |
| Sodium bicarbonate | NaHCO₃ | Fast but transient; NOT recommended (systemic alkalosis, Na load) |
| Combined Al(OH)₃ + Mg(OH)₂ (Maalox, Mylanta) | Mix | Balances bowel effects |
Mechanism of Action
Antacids work by direct chemical neutralization of hydrochloric acid in the gastric lumen - they do not affect acid secretion.
Key reactions:
- Al(OH)₃ + 3 HCl → AlCl₃ + 3 H₂O
- Mg(OH)₂ + 2 HCl → MgCl₂ + 2 H₂O
- CaCO₃ + 2 HCl → CaCl₂ + H₂O + CO₂
- NaHCO₃ + HCl → NaCl + H₂O + CO₂ (produces gas/belching)
The efficacy depends on:
- Acid-neutralizing capacity of the formulation
- Fed vs. fasted state: Food delays gastric emptying → prolongs antacid contact time and duration of action. Antacids taken after meals last 2-3 hours vs. ~30 min if taken fasting.
Therapeutic Uses
- Symptomatic relief of heartburn, GERD, peptic ulcer disease
- Rapid onset - work within minutes; therefore useful for on-demand symptom relief
- Give after meals for maximum duration of effect
- Calcium carbonate preparations also used as calcium supplements for osteoporosis prevention
- Anesthesia premedication (sodium citrate) to raise gastric pH before emergency surgery
Adverse Effects
| Antacid | Main Adverse Effect | Notes |
|---|---|---|
| Aluminum hydroxide | Constipation | Also binds dietary phosphate → hypophosphatemia with long-term use (used therapeutically in dialysis patients) |
| Magnesium hydroxide | Diarrhea | Mg²⁺ accumulation in renal failure → hypermagnesemia |
| Calcium carbonate | Constipation, acid rebound, hypercalcemia | Milk-alkali syndrome with excessive use |
| Sodium bicarbonate | Metabolic alkalosis, sodium load, CO₂ bloating | Contraindicated in hypertension, heart failure, renal failure |
| Combined Al/Mg | Neutralizes bowel effects | Still risk of ion accumulation in renal impairment |
Renal impairment: Accumulation of Mg²⁺, Al³⁺, and Ca²⁺ cations can cause toxicity. Use with caution or avoid in patients with renal failure.
Drug Interactions (Antacids)
Antacids affect absorption of many drugs by:
- Raising gastric pH → reducing dissolution of weak bases (ketoconazole, itraconazole, atazanavir)
- Chelation / adsorption: Al³⁺ and Mg²⁺ bind to and reduce absorption of:
- Tetracyclines, fluoroquinolones (ciprofloxacin), iron supplements, digoxin, levothyroxine, azithromycin
- Separate antacids from these drugs by at least 2 hours
COMPARATIVE SUMMARY TABLE
| Feature | PPIs | H2 Blockers | Antacids |
|---|---|---|---|
| Mechanism | Irreversible inhibition of H⁺/K⁺-ATPase | Competitive H2 receptor blockade | Direct acid neutralization |
| Acid suppression | 80-95% | ~70% | No effect on secretion |
| Onset of action | 30-60 min (takes days for full effect with new pumps) | 45-60 min | Within minutes |
| Duration | ~24 h (outlasts plasma t½) | 6-12 h | 30 min (fasting) to 2-3 h (postprandial) |
| Tolerance | No | Yes (tachyphylaxis) | No |
| Best for | GERD, erosive esophagitis, ZE syndrome, H. pylori eradication | Mild GERD, nocturnal acid, ICU stress ulcer | Rapid symptom relief only |
| Requires acid for activation | Yes (prodrug) | No | No |
| Timing | 30 min before first meal | Can be taken any time | After meals |
| Key adverse effects | Hypomagnesemia, B12 deficiency, C. diff, bone fractures | Antiandrogenic (cimetidine), CNS effects (elderly) | Constipation (Al), diarrhea (Mg), alkalosis (NaHCO₃) |
| CYP interactions | Clopidogrel (omeprazole) | Many (cimetidine) | Absorption chelation |
| Renal dosing | Not required | Required (all agents) | Caution (ion accumulation) |
CLINICAL PEARLS
-
PPIs must be taken before eating - food stimulates acid production, activating newly synthesized pumps, making PPIs more effective. The first dose never achieves maximal effect; it takes 3-4 days of regular dosing to inhibit ~70% of pumps.
-
Stopping PPIs suddenly can cause rebound hypersecretion due to hypergastrinemia - taper when discontinuing after prolonged use.
-
Cimetidine is the worst for drug interactions - its broad CYP inhibition and antiandrogenic effects make it the least preferred H2 blocker.
-
Ranitidine was withdrawn worldwide due to NDMA (N-Nitrosodimethylamine) contamination.
-
Al hydroxide causes constipation; Mg hydroxide causes diarrhea - combining them balances bowel effects.
-
The clopidogrel-omeprazole interaction carries a boxed warning. Pantoprazole is the preferred PPI in patients on clopidogrel.
-
H2 blockers in renal failure require dose adjustment; PPIs do not (they are hepatically cleared).
-
Antacids are NOT long-term solutions - they provide no mucosal healing and relief is short-lived.
-
CYP2C19 poor metabolizers (common in East Asians) achieve higher plasma PPI levels → better acid suppression but also greater risk of adverse effects.
-
PPIs reduce Clostridium difficile defense - by raising gastric pH, they remove an important barrier to ingested spores. Limit use to lowest effective dose and duration.
Sources: Goodman & Gilman's The Pharmacological Basis of Therapeutics, 14e (Chapter 53); Lippincott Illustrated Reviews: Pharmacology, 8e (Chapter 42); Katzung's Basic and Clinical Pharmacology, 16e (Chapter 62)
This is a shared conversation. Sign in to Orris to start your own chat.