Abdominal pain
Reading File
search_medical_text
abdominal pain causes differential diagnosis evaluation
search_medical_text
abdominal pain history physical examination management approach
search_medical_image
abdominal pain regions quadrants differential diagnosis
GradeResponse
GradeResponse
GradeResponse
Abdominal Pain
Abdominal pain is one of the most common presenting complaints in clinical medicine and ranges from benign, self-limiting conditions to life-threatening emergencies. Correctly identifying the cause requires careful history-taking, physical examination, and targeted investigations (Harrison's, p. 554).
Approach by Location
The anatomical location of pain is the single most important clue to its etiology.
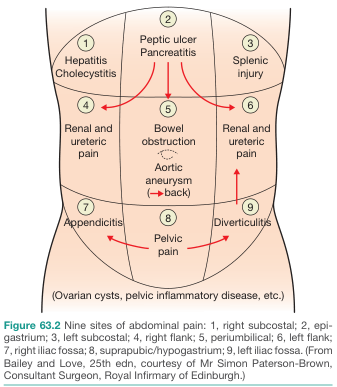
| Region | Key Diagnoses |
|---|---|
| Right subcostal (RUQ) | Cholecystitis, hepatitis, biliary colic, hepatic abscess |
| Epigastrium | Peptic ulcer disease, pancreatitis, GERD, gastritis, MI (referred) |
| Left subcostal (LUQ) | Splenic injury/infarct, gastric pathology, left lower lobe pneumonia |
| Right flank | Renal colic, ureteric stone, pyelonephritis |
| Periumbilical | Bowel obstruction, early appendicitis, aortic aneurysm, mesenteric ischemia |
| Left flank | Renal colic, ureteric stone, pyelonephritis |
| Right iliac fossa (RIF) | Appendicitis, ovarian pathology, Crohn's disease, ectopic pregnancy |
| Suprapubic/hypogastrium | UTI, pelvic inflammatory disease (PID), ovarian cysts, bladder pathology |
| Left iliac fossa (LIF) | Diverticulitis, sigmoid pathology, ovarian pathology |
Key History Features
- Onset: Sudden (perforation, vascular event) vs. gradual (inflammatory)
- Character: Colicky (obstruction, renal/biliary colic) vs. constant (peritonitis, ischemia)
- Radiation: To back (pancreatitis, AAA), to shoulder (diaphragmatic irritation), to groin (renal colic)
- Severity: 1–10 scale; severity alone does not predict seriousness
- Modifying factors: Worse with movement (peritonitis), relieved by vomiting (obstruction), related to meals (PUD, mesenteric angina)
- Associated symptoms: Fever, vomiting, diarrhea, constipation, dysuria, vaginal discharge, jaundice
- Menstrual history: Always essential in women of reproductive age (ectopic pregnancy, PID)
Physical Examination
Per Harrison's (p. 566), sufficient time must be spent in examination — abdominal signs may be minimal yet exceptionally meaningful. Key points:
- Inspection: Distension, visible peristalsis, scars, hernias, ecchymosis (Grey-Turner's/Cullen's signs in hemorrhagic pancreatitis)
- Palpation: Localized tenderness, guarding (voluntary/involuntary), rigidity, rebound (Blumberg's sign)
- Special signs:
- Murphy's sign — cholecystitis
- Rovsing's sign — appendicitis
- Psoas/obturator sign — retrocecal appendicitis
- Carnett's sign — abdominal wall pain
- Auscultation: Bowel sounds are the least revealing part of the exam; catastrophes (strangulated obstruction, perforated appendicitis) can occur with normal bowel sounds
- Pelvic and rectal exams are mandatory — pelvic peritonitis may present with minimal abdominal signs (Harrison's, p. 566)
Red Flags (Urgent/Surgical Causes)
| Feature | Consider |
|---|---|
| Sudden onset, "worst ever" pain | Aortic dissection/rupture, perforation |
| Peritoneal signs (rigidity, rebound) | Peritonitis from any cause |
| Hemodynamic instability | AAA rupture, ectopic pregnancy, mesenteric ischemia |
| Pain out of proportion to exam | Mesenteric ischemia |
| Pulsatile abdominal mass | AAA |
| Positive pregnancy test + pelvic pain | Ectopic pregnancy |
| High fever + jaundice + RUQ pain (Charcot's triad) | Ascending cholangitis |
Investigations
First-line:
- CBC, CMP (BMP + LFTs), lipase, lactate, urinalysis
- Urine/serum β-hCG in women of reproductive age
- ECG (exclude inferior MI as a cause of epigastric pain)
Imaging:
- Erect CXR: Free air under diaphragm (perforation)
- Abdominal X-ray: Obstruction (dilated loops, air-fluid levels)
- Ultrasound: First-line for RUQ pain (gallstones, cholecystitis), pelvic pathology
- CT abdomen/pelvis with contrast: Broad, high-yield for acute abdomen — appendicitis, diverticulitis, pancreatitis, obstruction, vascular
- CT angiography: Mesenteric ischemia, AAA
Management Principles
- Stabilize — IV access, fluids, analgesia (adequate analgesia does not mask signs; withholding it is not recommended)
- Surgical consultation for peritoneal signs, obstruction, suspected ischemia/perforation
- Treat the underlying cause — antibiotic therapy, endoscopy, interventional radiology, or surgery as indicated
- Reassess frequently — the picture can evolve rapidly, especially in elderly or immunocompromised patients
Special Populations
- Elderly: Presentations are often atypical; pain may be blunted; mortality from surgical causes is higher
- Immunocompromised: Broader differential (opportunistic infections, typhlitis); peritoneal signs may be absent
- Pregnant: Appendix is displaced superiorly; ectopic pregnancy must be excluded early
- Children: Intussusception, Meckel's diverticulum, mesenteric adenitis prominent in differentials
Clinical pearl: The most catastrophic conditions may initially appear with subtle symptoms. A meticulous history and examination — including pelvic and rectal exams — are the cornerstone of evaluation (Harrison's, p. 554, 566).
Doxycycline
Reading File
search_medical_text
doxycycline mechanism of action pharmacology tetracycline
search_medical_text
doxycycline indications dosing clinical uses infections
GradeResponse
GradeResponse
Doxycycline
Doxycycline is a second-generation tetracycline antibiotic and one of the most broadly used antimicrobials in clinical medicine, valued for its oral bioavailability, broad spectrum, and activity against intracellular and atypical organisms.
Mechanism of Action
Doxycycline binds reversibly to the 16S rRNA of the 30S ribosomal subunit, blocking aminoacyl-tRNA from binding to the ribosomal A site and thereby inhibiting peptide elongation and protein synthesis. The drug is bacteriostatic. Selective active transport into bacterial (but not mammalian) cells underpins its selectivity (Harrison's, p. 4317).
Spectrum of Activity
| Category | Organisms |
|---|---|
| Gram-positive | Staph. aureus (including MRSA), Streptococcus spp. |
| Gram-negative | H. influenzae, Brucella, Francisella tularensis, Vibrio cholerae, Yersinia pestis |
| Atypicals | Mycoplasma pneumoniae, Chlamydia spp., Legionella |
| Spirochetes | Borrelia burgdorferi (Lyme), Treponema pallidum (syphilis), Leptospira |
| Rickettsial | Rickettsia (RMSF, typhus), Ehrlichia, Anaplasma, Coxiella (Q fever) |
| Parasitic | Plasmodium falciparum (malaria prophylaxis/treatment) |
| Other | Actinomyces, Nocardia, Tropheryma whipplei (Whipple's disease) |
Clinical Indications
Per Harrison's (p. 4347), doxycycline has wide clinical uses:
Infectious Diseases
- STIs: Chlamydia trachomatis, lymphogranuloma venereum, granuloma inguinale; nongonococcal urethritis/cervicitis
- Lyme disease: Drug of choice for early localized and disseminated disease (except CNS/cardiac involvement in some cases)
- Rickettsial infections: Drug of choice for Rocky Mountain spotted fever, scrub typhus, ehrlichiosis, anaplasmosis
- Atypical pneumonia: Mycoplasma, Chlamydia pneumoniae, Legionella
- Community-acquired pneumonia (CAP): Monotherapy for outpatient treatment in otherwise healthy adults
- Skin & soft tissue infections: Including MRSA (in combination) and animal bites
- Syphilis: Alternative to penicillin in non-pregnant penicillin-allergic patients
- Brucellosis: With rifampin (6 weeks)
- Tularemia: With streptomycin or gentamicin in severe disease
- Malaria prophylaxis: 100 mg daily, starting 1–2 days before travel; treatment adjunct with quinine/artemisinin
- Anthrax (post-exposure prophylaxis and treatment)
- Whipple's disease
- Pelvic inflammatory disease (PID): With ceftriaxone ± metronidazole
Non-Infectious Uses
- Acne vulgaris: Anti-inflammatory and antibacterial properties
- Rosacea: Low-dose doxycycline (40 mg modified-release)
- Periodontal disease: Low-dose adjunctive therapy
- Pleurodesis: IV/intrapleural for malignant effusions
Dosing
| Indication | Dose | Duration |
|---|---|---|
| Community-acquired pneumonia | 100 mg PO BID | 5–7 days |
| Chlamydia | 100 mg PO BID | 7 days |
| Lyme disease (early) | 100 mg PO BID | 10–21 days |
| RMSF / rickettsial | 100 mg PO/IV BID | Minimum 3 days after defervescence (typically 5–7 days) |
| Malaria prophylaxis | 100 mg PO daily | Start 1–2 days before, continue 4 weeks after |
| MRSA SSTI | 100 mg PO BID | 5–10 days |
| Acne | 50–100 mg PO daily or BID | Long-term |
| Rosacea (sub-antimicrobial) | 40 mg PO daily (modified-release) | Long-term |
- Renal dose adjustment is generally not required (hepatically eliminated)
- Hepatic impairment: Use with caution; consider dose reduction in severe disease
Pharmacokinetics
| Parameter | Detail |
|---|---|
| Bioavailability | ~93% oral (superior to tetracycline) |
| Food effect | Can be taken with food (reduces GI upset without significantly reducing absorption) |
| Protein binding | ~90% |
| Half-life | 16–22 hours (allows once or twice daily dosing) |
| Distribution | Wide — penetrates bone, lung, CSF (moderate), prostate |
| Elimination | Primarily fecal; renal excretion minor (~40%) |
Adverse Effects
| System | Effect |
|---|---|
| GI | Nausea, vomiting, esophageal irritation/ulceration (take upright with full glass of water) |
| Dermatologic | Photosensitivity (counsel sun avoidance), drug-induced lupus (rare) |
| Dental/skeletal | Permanent tooth discoloration and enamel hypoplasia if used in children <8 years or in pregnancy (2nd/3rd trimester) |
| Hepatotoxicity | Rare; dose-related at very high doses |
| Intracranial hypertension | Pseudotumor cerebri — especially with concurrent isotretinoin |
| Vestibular | Less common than with minocycline, but possible |
| Clostridioides difficile | Colitis risk (lower than broad-spectrum agents, but real) |
Drug Interactions
| Interacting Agent | Effect | Management |
|---|---|---|
| Antacids, calcium, magnesium, iron, zinc | Chelation reduces absorption by up to 90% | Take doxycycline 2 hours before or 6 hours after |
| Dairy products | Mild chelation (less than with tetracycline) | Can be taken with food; avoid large quantities of dairy |
| Warfarin | Potentiates anticoagulant effect | Monitor INR closely |
| Retinoids (isotretinoin) | Additive risk of intracranial hypertension | Contraindicated together |
| Oral contraceptives | Theoretical reduction in efficacy (evidence weak) | Counsel patients; use backup contraception |
| Barbiturates, phenytoin, carbamazepine | Induce hepatic metabolism, reducing doxycycline levels | Consider dose increase or alternative |
| Penicillins | Bacteriostatic action may antagonize bactericidal penicillins | Avoid combining when bactericidal action is critical |
| Methoxyflurane | Fatal nephrotoxicity reported | Contraindicated |
Contraindications & Special Populations
- Pregnancy: Avoid — causes fetal tooth discoloration and bone growth inhibition (category D); exception: RMSF in pregnancy where benefit may outweigh risk
- Children <8 years: Avoid unless benefits clearly outweigh risks (e.g., RMSF, anthrax) — permanent dental staining
- Breastfeeding: Avoid
- Esophageal disease: Use with caution; instruct patients to remain upright for 30 minutes after ingestion and take with a full glass of water
Key Clinical Pearls
- Doxycycline is the drug of choice for all rickettsial diseases, including in children when benefits outweigh risks (RMSF has a high mortality if untreated)
- Unlike tetracycline, it can be taken with food, making it better tolerated
- It does not require renal dose adjustment, making it useful in patients with renal impairment
- Sub-antimicrobial dosing (40 mg/day) provides anti-inflammatory effects without meaningful selective antibiotic pressure — used in rosacea and periodontitis
This is a shared conversation. Sign in to Orris to start your own chat.