Filariasis microbiology 10 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive information for a detailed 10-mark answer. Let me compile the full answer:
Filariasis - Microbiology (10 Marks)
1. Introduction
Filariasis is a parasitic infection caused by thread-like nematode worms (filariae) of the order Spirurida. The three most clinically important species causing lymphatic filariasis in humans are:
- Wuchereria bancrofti - responsible for ~90% of all cases
- Brugia malayi
- Brugia timori
Other filariae include Loa loa (loiasis), Onchocerca volvulus (river blindness), and Mansonella spp.
2. Causative Organisms
| Feature | W. bancrofti | B. malayi | B. timori |
|---|---|---|---|
| Geographic distribution | Pan-tropical (Africa, India, SE Asia, Americas, Pacific) | Rural coastal Asia, South Pacific | Lesser Sunda Archipelago (Indonesia) |
| Vector | Culex, Anopheles, Aedes spp. | Mansonia, Anopheles spp. | Anopheles spp. (night-feeding) |
| Adult female length | ~100 mm | ~50 mm | ~50 mm |
| Animal reservoir | Humans only | Domestic/wild cats, monkeys | None |
Source: Sherris & Ryan's Medical Microbiology, 8th Ed.
3. Life Cycle
The life cycle involves two hosts: a human (definitive host) and a mosquito (intermediate host/vector).
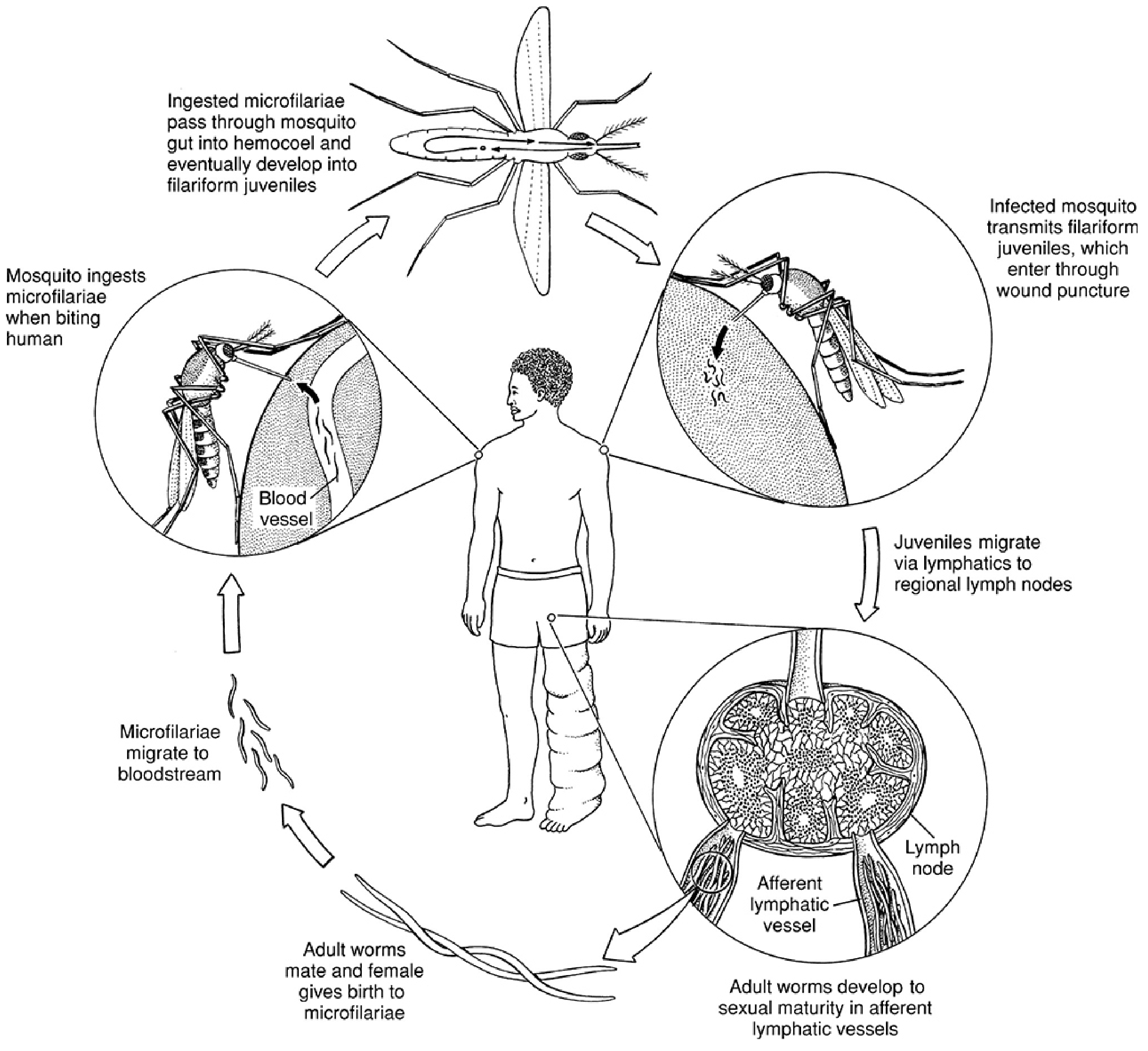
Life cycle of W. bancrofti - Sherris & Ryan's Medical Microbiology, 8th Ed.
In the Human Host:
- Infective L3 larvae are deposited on the skin when an infected mosquito feeds
- Larvae penetrate the skin through the bite wound
- Larvae migrate to lymphatic vessels and undergo sequential molts (L3 → L4 → adult)
- Adults mature in 6-12 months and live in lymphatics for up to a decade
- Adult males (40 mm) and females (100 mm for W. bancrofti) lie coiled together in lymphatic vessels
- Gravid females produce embryonated eggs that uncoil into microfilariae (200-300 μm), retaining the egg shell as a thin sheath
- Microfilariae migrate into the bloodstream
In the Mosquito (Intermediate Host):
- Mosquito ingests microfilariae during a blood meal
- Microfilariae shed their sheaths and pass through the gut wall into thoracic flight muscles
- Undergo two molts: microfilariae → rhabditiform larvae → filariform (L3) larvae
- L3 larvae migrate to the proboscis of the mosquito
- Transmitted to new human host during next blood meal
4. Microfilariae - Key Differentiating Features
The microfilariae of different species are distinguished by size, sheath, tail nuclei, and periodicity:
| Feature | W. bancrofti | B. malayi | Loa loa | O. volvulus |
|---|---|---|---|---|
| Location | Blood | Blood | Blood | Skin |
| Sheath | Yes (transparent, Giemsa-negative) | Yes (deep pink on Giemsa) | Yes (transparent) | No |
| Size | 244-296 μm (stained) | ~220 μm | ~275 μm | ~300 μm |
| Tail nuclei | Absent (clear tip) | Two widely spaced nuclei | Continuous to tip | Absent |
| Periodicity | Nocturnal (peak 9 PM-2 AM) | Nocturnal | Diurnal (peak noon) | None |
| Polynesian strain | Subperiodic (early evening) | - | - | - |
Source: Sherris & Ryan's Medical Microbiology, 8th Ed., Table 55-2
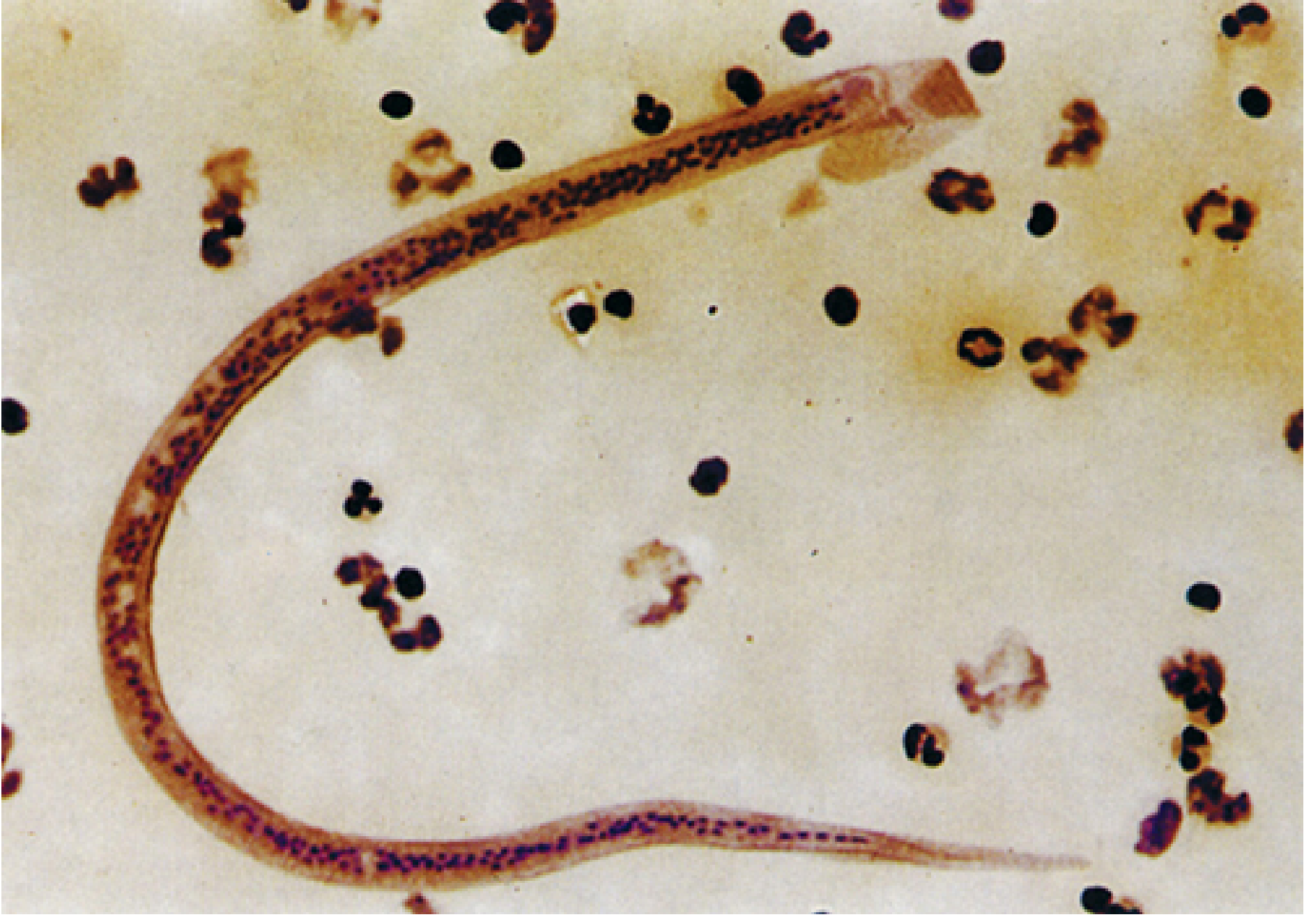
Microfilaria of W. bancrofti in blood film (Sherris & Ryan)
Rationale for nocturnal periodicity: Microfilariae accumulate in pulmonary vessels during the day. At night, in response to changes in oxygen tension, they spill into the peripheral circulation to coincide with the peak biting time of their mosquito vector - an evolutionary adaptation to maximize transmission.
5. Wolbachia Endosymbiont
A remarkable feature of Wuchereria and Brugia worms: they harbor intracellular bacteria of the genus Wolbachia in their gut. These bacteria:
- Are essential for worm fertility and health
- Release inflammatory lipopolysaccharide (LPS)-like molecules contributing to host tissue damage
- Are a therapeutic target: doxycycline kills Wolbachia, impairing worm reproduction
6. Pathogenesis & Pathology
Pathological changes are confined primarily to the lymphatic system and occur in two phases:
Acute Phase:
- Molting larvae and dying adult worms trigger:
- Lymphatic dilatation and endothelial hyperplasia
- Infiltration by lymphocytes, plasma cells, and eosinophils
- Thrombus formation (acute lymphangitis)
- Granuloma formation and fibrosis follow
- Bacterial/fungal superinfections of skin frequently supervene
Chronic Phase (with repeated infections):
- Permanent lymphatic obstruction
- Skin and subcutaneous tissues become edematous, thickened, and fibrotic
- Dilated lymphatics may rupture - spilling lymph into tissues or body cavities
- Leads to elephantiasis (massive lymphedema) over decades
- Lymph may spill into the urinary tract causing chyluria or into the peritoneum causing chylous ascites
7. Clinical Features
A. Asymptomatic Microfilaremia
- Most common presentation in endemic populations
- Some spontaneously clear infection
B. Acute Filarial Fever
- Begins 8-12 months post-exposure
- Fever (can reach 40°C), chills, myalgia
- Lymphadenitis - classically starts in the femoral region, spreads centrifugally down the leg
- Lymphangitis (retrograde - moves away from the node, unlike bacterial lymphangitis)
- In Bancroftian filariasis: orchitis, epididymitis, funiculitis due to involvement of testicular/spermatic cord lymphatics
- Episodes last a few days and recur over weeks to months
C. Chronic Lymphatic Obstruction
- Lymphedema of lower limbs (most common), genitalia
- Hydrocele (most common manifestation in men)
- Elephantiasis of legs, scrotum, or labia
D. Tropical Pulmonary Eosinophilia (TPE)
- Aberrant immune response, mainly in India, Pakistan, Sri Lanka, SE Asia
- Microfilariae trapped in pulmonary capillaries - destroyed by eosinophils
- Features: nocturnal wheeze, cough, fever, marked eosinophilia (>3000/μL), elevated IgE
- High filarial antibody titers, absent microfilaremia in blood
- Can cause permanent lung damage if untreated
8. Laboratory Diagnosis
Direct Methods:
- Peripheral blood smear (thick and thin films, Giemsa-stained) - collected between 10 PM and 2 AM due to nocturnal periodicity
- Membrane filtration of blood using Nucleopore polycarbonate membrane - concentrates microfilariae, increases sensitivity
- Knott's concentration technique - blood mixed with 2% formalin, centrifuged, sediment examined
- For O. volvulus and M. streptocerca: skin snips (not blood)
Indirect Methods:
- Serology: Filarial antibody detection - limited by cross-reactivity with other nematodes; cannot distinguish past from current infection
- Antigen detection (ICT card test): Detects circulating filarial antigen of W. bancrofti - high sensitivity; can be done at any time of day; not widely available in non-endemic settings
- Ultrasonography: "Filarial dance sign" - live adult worms in lymphatics visible on scrotal ultrasound as characteristic "dancing" movement
- PCR for species confirmation
9. Treatment
| Drug | Mechanism | Indication |
|---|---|---|
| Diethylcarbamazine (DEC) | Kills microfilariae and adult worms | Drug of choice for lymphatic filariasis; also used in TPE |
| Ivermectin | Kills microfilariae (does not kill adults) | Used in mass drug administration programs; drug of choice for onchocerciasis |
| Albendazole | Microfilaricidal, some adulticidal activity | Used in combination with DEC or ivermectin |
| Triple therapy (DEC + albendazole + ivermectin) | Outstanding efficacy in clearing microfilariae | Recent trials - highly effective single-dose regimen for W. bancrofti and Loa loa |
| Doxycycline | Kills Wolbachia endosymbiont | Impairs adult worm fertility; adjunctive treatment |
- Chronic elephantiasis and scarring are not reversible - managed with supportive care (elevation, hygiene, compression)
- WHO Global Programme to Eliminate Lymphatic Filariasis (GPELF): Annual mass drug administration (MDA) with DEC + albendazole (or ivermectin in onchocerciasis co-endemic areas)
10. Epidemiology & Control
- ~120 million people infected worldwide; ~40 million with symptomatic lymphedema
- W. bancrofti is cosmopolitan in poorly sanitized, densely crowded tropical/urban areas
- Classified by WHO as a Neglected Tropical Disease (NTD)
- Control strategies: MDA, vector control (insecticide-treated bed nets, larval source reduction), morbidity management
- Elimination target: microfilarial carrier rate <1% and no new infections in children
Key Points to Remember:
- W. bancrofti - nocturnal microfilaremia, no tail nuclei, Giemsa-negative sheath
- B. malayi - nocturnal, two discrete tail nuclei, pink Giemsa-staining sheath
- Life cycle: L3 larvae → lymphatics → adult worms → microfilariae → mosquito → L3 (6-12 months to mature)
- Diagnosis: blood film at 10 PM-2 AM; ICT antigen test; filarial dance sign on USG
- Treatment: DEC (drug of choice); triple therapy for mass elimination; doxycycline targets Wolbachia
Sources: Sherris & Ryan's Medical Microbiology, 8th Edition; Tietz Textbook of Laboratory Medicine, 7th Edition; Henry's Clinical Diagnosis & Management, 24th Edition
Filariasis microbiology 10 marks refer to apurba shastry
Finding Sources
Finding Sources
Searching the Web
Apurba Shastry microbiology filariasis Wuchereria bancrofti life cycle pathogenesis
Finding Sources
Reading Web Page
https://www.slideshare.net/slideshow/lymphatic-filariasis-pp…
Reading File
Searching the Web
Apurba Sastry filariasis laboratory diagnosis treatment DEC clinical features lymphatic tropical eosinophilia
Reading File
Loading Image
Loading Image
Note: Apurba Sastry's Essentials of Medical Microbiology is not available in the digital textbook library. The answer below is structured exactly as per Apurba S Sastry's chapter on Lymphatic Filariasis (sourced from official Jaypee Brothers slides based on the book), supplemented by Sherris & Ryan's Medical Microbiology where needed.
FILARIASIS - Microbiology (10 Marks)
As per Apurba S Sastry - Essentials of Medical Microbiology
1. Introduction
Filariasis is a parasitic infection caused by nematodes (roundworms) belonging to the superfamily Filarioidea. The most important human filarial parasites causing lymphatic filariasis are:
- Wuchereria bancrofti - accounts for >90% of cases
- Brugia malayi
- Brugia timori
Other filariae: Loa loa, Onchocerca volvulus, Mansonella spp.
2. Wuchereria bancrofti (Bancroftian Filariasis)
Morphology
| Form | Description |
|---|---|
| Adult female | 80-100 mm long, 0.24-0.30 mm wide; filariform (thread-like) |
| Adult male | 40 mm long |
| Microfilaria | 244-296 μm long; sheathed; nuclei do NOT extend to tail tip |
Adults reside coiled in lymphatic vessels and lymph nodes.
3. Life Cycle
The life cycle involves two hosts: humans (definitive host) and a mosquito (intermediate host/vector).
Life cycle of W. bancrofti (Sherris & Ryan's Medical Microbiology, 8th Ed.)
A. In Humans (Definitive Host)
- Infective stage: L3 (filariform) larvae - deposited on skin at mosquito bite site
- L3 larvae penetrate the bite wound and migrate to lymphatic vessels
- Undergo molts: L3 → L4 → adult (takes 6-12 months to reach sexual maturity)
- Adult male and female worms live together in lymphatics for 5-10 years
- Mated females are viviparous - produce sheathed microfilariae directly (ovo-viviparous)
- Microfilariae enter the peripheral blood - show nocturnal periodicity (peak: 10 PM - 2 AM), except in Pacific Islands where they are subperiodic
- Microfilariae accumulate in pulmonary capillaries during the day; at night they spill into peripheral blood to coincide with peak vector-biting time
B. In Mosquito (Intermediate Host / Vector)
- Primary vector: Culex quinquefasciatus (in India and most tropical areas)
- Anopheles and Aedes also transmit in some regions
- Mosquito ingests microfilariae during blood meal
- Microfilariae shed their sheath, penetrate gut wall, and reach thoracic flight muscles
- Develop through two molts: microfilariae → rhabditiform (L1) → sausage-form (L2) → filariform (L3) larvae
- L3 larvae migrate to the head and proboscis
- Transmitted to new human host during next blood meal (the mosquito does NOT inject larvae - they escape onto the skin at the bite wound)
4. Microfilaria - Key Features
Microfilaria of W. bancrofti in blood film
Differences Between Microfilariae of W. bancrofti and B. malayi
| Feature | W. bancrofti | B. malayi |
|---|---|---|
| Sheath | Present; does not stain with Giemsa (negative outline) | Present; stains deep pink with Giemsa |
| Size | 244-296 μm (stained film) | ~220 μm |
| Tail nuclei | Absent - nuclei do NOT reach tail tip | Two distinct widely-spaced nuclei in tail tip |
| Cephalic space | Short | Long (longer than wide) |
| Periodicity | Nocturnal (subperiodic in Pacific) | Nocturnal |
| Location | Blood | Blood |
| Genital involvement | Yes (orchitis, hydrocele, chyluria) | No |
| Elephantiasis | Whole leg, genitalia | Only below the knee |
5. Pathogenesis and Pathology
(As per Apurba S Sastry)
Tissue damage results from four mechanisms:
- Migration of live adult worms - causes lymphatic dilatation and thickening of vessel walls; as long as the worm remains viable, lymphatics are damaged but remain patent
- Death of adult worm - triggers enhanced granulomatous reaction and fibrosis of lymph vessels, leading to permanent obstruction
- Antigens and toxic metabolites released from dead adult worms - amplify inflammatory response
- Secondary bacterial and fungal infections - perpetuate tissue damage
Host Immune Response (Apurba Sastry)
- Both cellular (TH1) and humoral (TH2) responses are altered
- Antigens of adult worms and microfilariae are processed by macrophages (APCs) and presented to TH cells
- TH cells differentiate into TH1 (cellular immunity) and/or TH2 cells (humoral - IgE, eosinophilia)
- The balance between TH1 and TH2 responses determines clinical outcome
6. Clinical Features
(Incubation period: 8-16 months per Apurba Sastry)
Clinical manifestations are divided into three categories:
A. Lymphatic Filariasis (Classical/Symptomatic)
Acute phase:
- Adenolymphangitis (ADL): Recurrent episodes of fever, lymphadenitis, and lymphangitis - characteristically retrograde (spreads centrifugally away from the lymph node, unlike bacterial lymphangitis which is centripetal)
- Femoral lymph nodes classically involved first
- In Bancroftian filariasis: orchitis, epididymitis, funiculitis (testicular/spermatic cord involvement)
Chronic phase (repeated infections):
- Permanent lymphatic obstruction and progressive lymphedema
- Elephantiasis - gross swelling of lower limbs, scrotum/labia
- Hydrocele (most common manifestation in males)
- Chyluria - leakage of milky lymph into urine (rupture of intra-abdominal lymphatics)
- Chylous ascites, pleural effusion
B. Tropical Pulmonary Eosinophilia (TPE) - Occult Filariasis
- A hypersensitivity (TH2-mediated) reaction to microfilariae trapped in pulmonary capillaries
- Microfilariae are absent from peripheral blood (hence "occult")
- Common in India, Pakistan, Sri Lanka, SE Asia
- Features:
- Nocturnal cough and wheeze (symptoms worse at night - correlating with nocturnal periodicity)
- Low-grade fever, weight loss, lymphadenopathy
- Marked eosinophilia (>3000/μL, often much higher)
- Markedly elevated serum IgE and anti-filarial antibody titers
- Differential diagnosis: Asthma, ABPA, Löffler's syndrome, Churg-Strauss syndrome
- Treatment: DEC 6 mg/kg for 14-21 days
C. Immune Complex-Mediated Manifestations
- Glomerulonephritis, proteinuria, hematuria
- From deposition of immune complexes (filarial antigen-antibody) in kidneys
7. Laboratory Diagnosis
A. Microscopy (Definitive/Direct)
| Method | Details |
|---|---|
| Peripheral blood smear | Thick and thin films, Giemsa-stained; blood collected between 10 PM and 2 AM (nocturnal periodicity) |
| Knott's concentration | 1 mL blood + 9 mL 2% formalin → centrifuge → examine sediment; increases sensitivity |
| Membrane filtration | Blood filtered through polycarbonate membrane (3 μm pore size) - highest sensitivity |
| Examination of hydrocele fluid / chylous urine | May also show microfilariae |
B. Antigen Detection
- Immunochromatographic test (ICT / Og4C3 ELISA): Detects circulating filarial antigen (CFA) of W. bancrofti
- Can be done at any time of day (does not depend on periodicity)
- High sensitivity and specificity; WHO-recommended for field surveys
C. Antibody Detection
- ELISA - detects anti-filarial IgG/IgG4 antibodies; confirmation test
- Brugia Rapid (ICT) - detects parasite-specific IgG4 antibodies against recombinant BmR1 antigen of B. malayi; used for brugian filariasis
- Limitation: cannot distinguish active infection from past exposure; cross-reactivity with other helminths
D. Imaging
- Ultrasonography (scrotal/inguinal): Detects live adult worms in lymphatics - show characteristic "filarial dance sign" (serpentine movement of live worms in dilated lymphatics)
- Lymphoscintigraphy: Assesses lymphatic dysfunction in established disease
E. Molecular Methods
- Real-time PCR: Detects filarial DNA - genes such as SspI repeat, pWb12 repeat, pWb-35
- Useful for species confirmation and in low-microfilaremia cases
F. Other supportive findings
- Eosinophilia (often >3000/μL in TPE)
- Elevated serum IgE
8. Treatment
(As per Apurba S Sastry)
A. Diethylcarbamazine (DEC) - Drug of Choice
- Dose: 6 mg/kg/day for 12 days (for lymphatic filariasis)
- 14-21 days for tropical pulmonary eosinophilia
- Can kill both adult worms and microfilariae - adult worms are more susceptible
- Mechanism: immobilizes microfilariae → facilitates immune-mediated killing; alters microfilaria surface making them susceptible to host immune attack
- Side effects: Mazzotti-like reaction (fever, headache, myalgia) from dying parasites
B. Ivermectin
- Kills microfilariae only (does not kill adult worms)
- Used in mass drug administration (MDA) programs, especially where Loa loa is co-endemic (DEC contraindicated there due to encephalopathy risk)
- Also first-line for Onchocerca volvulus
C. Albendazole
- Has microfilaricidal and some adulticidal activity
- Used in combination with DEC or ivermectin for MDA (WHO recommended)
D. Triple Therapy
- DEC + Albendazole + Ivermectin in a single dose - outstanding efficacy in clearing microfilariae (recent trials)
E. Doxycycline
- Targets intracellular Wolbachia endosymbiont bacteria inside adult worms
- Depleting Wolbachia impairs worm fertility and survival - macrofilaricidal effect
- Dose: 100-200 mg/day for 4-6 weeks
- Important adjunct for adulticidal therapy
Note: Chronic elephantiasis is NOT reversible - managed with elevation, compression bandaging, hygiene, and surgical debulking.
9. Brugian Filariasis (B. malayi / B. timori) - Key Differences
| Feature | Bancroftian (W. bancrofti) | Brugian (B. malayi) |
|---|---|---|
| Vector | Culex, Anopheles, Aedes | Mansonia (nocturnal strains); Coquillettidia, Mansonia (subperiodic) |
| Reservoir | Humans only | Humans; subperiodic strains also in monkeys, cats, dogs |
| Genital involvement | Yes - orchitis, hydrocele, chyluria | No |
| Elephantiasis | Whole leg + genitalia | Only below the knee |
| Microfilaria sheath | Non-staining (Giemsa) | Deep pink (Giemsa) |
| Tail nuclei | None at tip | Two distinct nuclei at tip |
10. Prevention and Control
- Mass Drug Administration (MDA): Annual single dose of DEC + Albendazole to entire at-risk population - WHO GPELF (Global Programme to Eliminate Lymphatic Filariasis) strategy
- Vector control: Insecticide-treated bed nets, indoor residual spraying, larval source management (Culex breeds in stagnant, polluted water)
- Morbidity management: Limb hygiene, wound care to prevent secondary infections
- India: Highly endemic states - UP, Jharkhand, Bihar, West Bengal (account for ~2/3 of India's burden); India accounts for ~40% of global burden
- Elimination target: Microfilaria rate <1%; interruption of transmission
Summary Table: Important Points for Exams
| Point | Fact |
|---|---|
| Causative agent | W. bancrofti (>90%), B. malayi, B. timori |
| Infective stage | L3 (filariform) larvae |
| Diagnostic stage | Microfilariae in peripheral blood |
| Vector for W. bancrofti | Culex quinquefasciatus (main), also Anopheles, Aedes |
| Vector for B. malayi | Mansonia spp. |
| Periodicity | Nocturnal (10 PM-2 AM); Subperiodic in Pacific; Diurnal for Loa loa |
| Microfilaria sheath staining | W. bancrofti: negative; B. malayi: deep pink (Giemsa) |
| Drug of choice | DEC 6 mg/kg for 12 days |
| Filarial dance sign | USG showing serpentine movement of live adult worms |
| Occult filariasis | Tropical Pulmonary Eosinophilia - absent microfilaremia, high IgE |
| Wolbachia | Endosymbiont of adult worms; target of doxycycline |
Sources: Essentials of Medical Microbiology - Apurba S Sastry (Jaypee Brothers); Sherris & Ryan's Medical Microbiology, 8th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.