Abg analysis from basics to clinicals
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks to write a thorough ABG guide. Let me compile the full answer.
Arterial Blood Gas (ABG) Analysis: Basics to Clinicals
1. What Is an ABG and What Does It Measure?
An arterial blood gas analysis is drawn from an arterial sample (most commonly the radial artery) and provides direct measurements of:
| Parameter | Normal Value | What It Reflects |
|---|---|---|
| pH | 7.35 - 7.45 | Overall acid-base status (H+ concentration) |
| PaCO2 | 35 - 45 mm Hg | Respiratory component (CO2 "respiratory acid") |
| HCO3- | 22 - 26 mEq/L | Metabolic component (calculated via Henderson-Hasselbalch) |
| PaO2 | 80 - 100 mm Hg | Arterial oxygenation |
| SaO2 | 95 - 100% | Hemoglobin oxygen saturation |
ABG is the gold standard for oxygenation assessment and the only test that simultaneously gives respiratory and metabolic acid-base data. - Murray & Nadel's Textbook of Respiratory Medicine
2. The Henderson-Hasselbalch Framework
The physiologic basis:
CO2 + H2O ⇌ H2CO3 ⇌ HCO3- + H+
- Increased PaCO2 drives the reaction right → more H+ → lower pH → respiratory acidosis
- Decreased PaCO2 drives the reaction left → less H+ → higher pH → respiratory alkalosis
- Increased HCO3- drives the reaction left → less H+ → higher pH → metabolic alkalosis
- Decreased HCO3- drives the reaction right → more H+ → lower pH → metabolic acidosis
- Symptom to Diagnosis, 4th Edition
3. Step-by-Step ABG Interpretation (6-Step Method)
Step 1: Determine Acidemia vs. Alkalemia
- pH < 7.35 = Acidemia
- pH > 7.45 = Alkalemia
- pH 7.35-7.45 = "Normal" (may still have a compensated or mixed disorder)
Step 2: Identify the Primary Disorder
Look at PaCO2 and HCO3- together:
| pH | Primary Driver | Disorder |
|---|---|---|
| Low | PaCO2 > 45 mm Hg | Respiratory acidosis |
| Low | HCO3- < 22 mEq/L | Metabolic acidosis |
| High | PaCO2 < 35 mm Hg | Respiratory alkalosis |
| High | HCO3- > 26 mEq/L | Metabolic alkalosis |
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
Step 3: Check for Appropriate Compensation
Compensation is never complete - it returns pH toward (not to) normal. The direction of compensation is always the same as the primary disorder.
| Primary Disorder | Compensation | Formula |
|---|---|---|
| Metabolic acidosis | ↓ PaCO2 | PaCO2 = (1.5 × HCO3-) + 8 ± 2 (Winter's formula) |
| Metabolic alkalosis | ↑ PaCO2 | PaCO2 ↑ 0.7 mm Hg per 1 mEq/L ↑ HCO3- |
| Respiratory acidosis (acute) | ↑ HCO3- | HCO3- ↑ 1 mEq/L per 10 mm Hg ↑ PaCO2 |
| Respiratory acidosis (chronic) | ↑ HCO3- | HCO3- ↑ 4 mEq/L per 10 mm Hg ↑ PaCO2 |
| Respiratory alkalosis (acute) | ↓ HCO3- | HCO3- ↓ 2 mEq/L per 10 mm Hg ↓ PaCO2 |
| Respiratory alkalosis (chronic) | ↓ HCO3- | HCO3- ↓ 4 mEq/L per 10 mm Hg ↓ PaCO2 |
Winter's formula tip: In metabolic acidosis, the expected PCO2 ≈ last two digits of the pH (e.g., if pH = 7.23, expected PCO2 ≈ 23). - Roberts and Hedges'
If compensation is more than expected → concurrent respiratory alkalosis (or metabolic alkalosis)
If compensation is less than expected → concurrent respiratory acidosis (or metabolic acidosis)
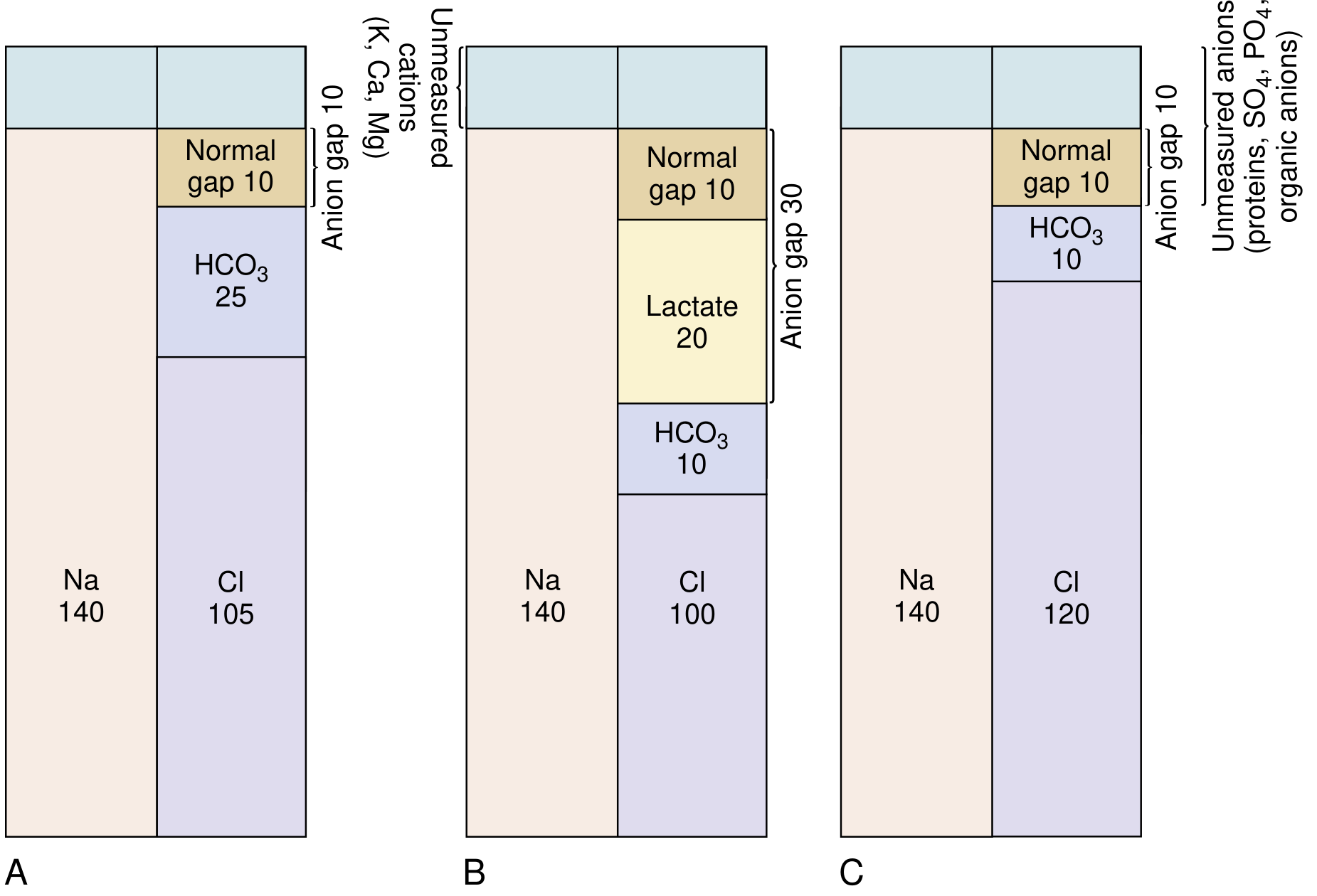
Step 4: Calculate the Anion Gap (if metabolic acidosis present)
AG = Na+ - (Cl- + HCO3-)
Normal AG = 8-12 mEq/L (some labs use 7-9 mEq/L)
The AG represents "unmeasured anions" - mainly albumin, phosphate, sulfate, and organic acids.
Corrected AG for hypoalbuminemia:
AGcorrected = AG + 2.5 × (4 - serum albumin)
For each 1 g/dL drop in albumin below 4, add 2.5 mEq/L to the AG. Critically ill patients are almost always hypoalbuminemic - missing this masks a hidden AG acidosis. - National Kidney Foundation Primer on Kidney Diseases, 8e
Step 5: Differential Diagnosis by AG
Elevated AG metabolic acidosis - mnemonic GOLDMARK:
| Letter | Cause |
|---|---|
| G | Glycols (ethylene glycol, propylene glycol) |
| O | Oxoproline (pyroglutamic acid, acetaminophen toxicity) |
| L | L-Lactic acidosis (Type A: hypoperfusion; Type B: drugs/disease) |
| D | D-Lactic acidosis (short bowel syndrome) |
| M | Methanol |
| A | Aspirin (salicylates) |
| R | Renal failure (uremia) |
| K | Ketoacidosis (DKA, alcoholic, starvation) |
- National Kidney Foundation Primer on Kidney Diseases, 8e
Normal AG (hyperchloremic) metabolic acidosis - mnemonic DURHAM:
- Diarrhea
- Ureteral diversion (ureteroileostomy)
- Renal tubular acidosis (RTA)
- Hyperalimentation
- Acetazolamide (carbonic anhydrase inhibitors)
- Miscellaneous (dilutional, early renal failure)
Step 6: Calculate Delta-Delta (Δ/Δ) Ratio if AG is Elevated
This detects a mixed metabolic disorder hiding behind an AG acidosis.
Δ/Δ = (AG - 12) / (24 - HCO3-)
| Δ/Δ Ratio | Interpretation |
|---|---|
| < 1.0 | AG acidosis + concurrent non-AG (hyperchloremic) acidosis |
| 1.0 - 2.0 | Pure AG acidosis |
| > 2.0 | AG acidosis + concurrent metabolic alkalosis (or pre-existing high HCO3-) |
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e
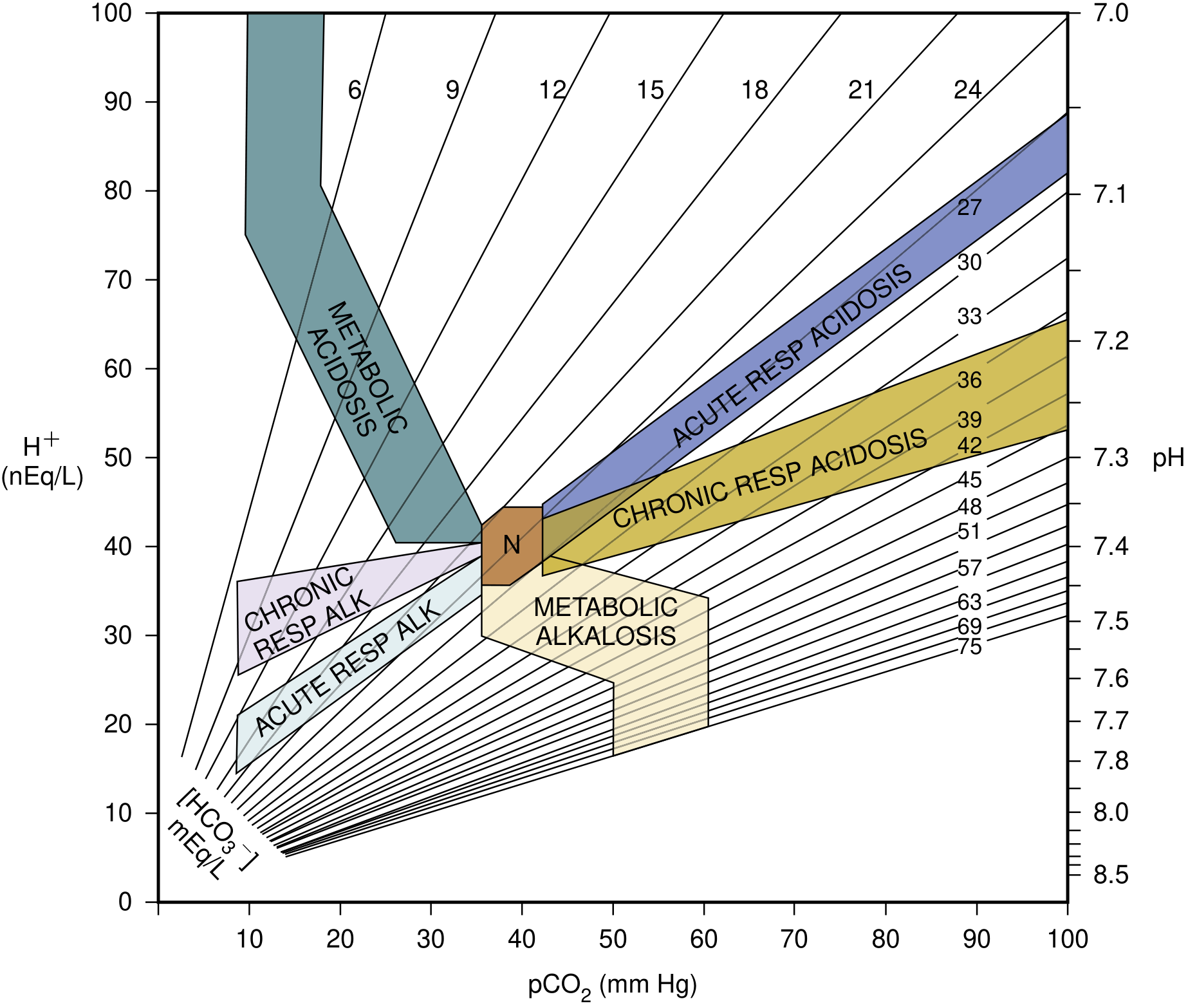
4. The Acid-Base Map
This map plots the 95% confidence bands for each simple disorder. If a patient's values fall outside a confidence zone, a mixed disorder is likely.
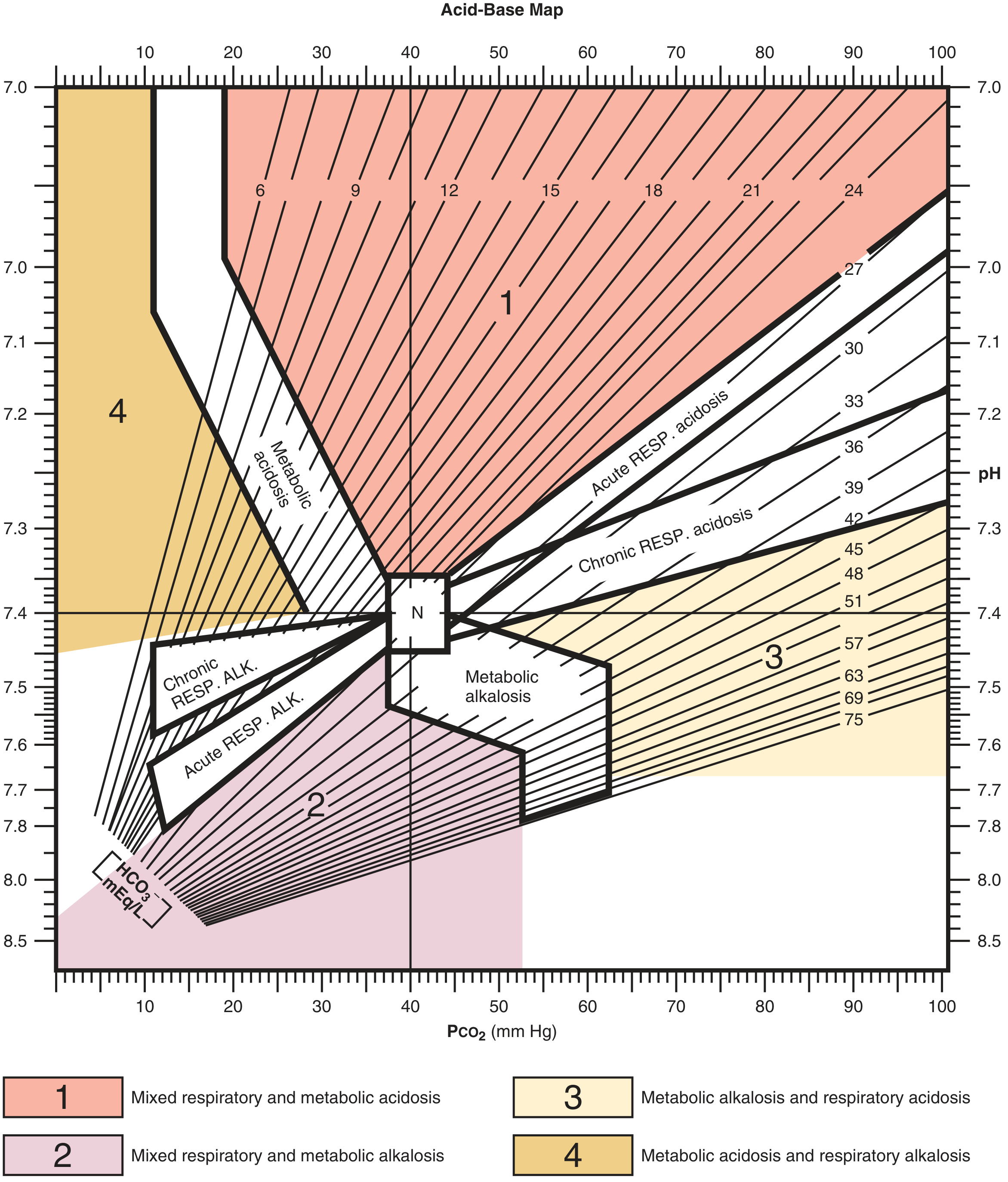
And the clinical (Roberts and Hedges) version with mixed disorder zones labeled:
5. Oxygenation Parameters from the ABG
PaO2 and Hypoxemia
- Normal PaO2 on room air: 80-100 mm Hg
- Hypoxemia: PaO2 < 80 mm Hg (mild), < 60 mm Hg (moderate-severe)
- PaO2/FiO2 (P/F ratio): useful in ICU; < 300 = ALI, < 200 = ARDS
Alveolar Gas Equation
PAO2 = FiO2 × (PB - PH2O) - PaCO2/R
Simplified (room air, sea level):
PAO2 = 150 - (PaCO2 / 0.8)
Or even simpler: PAO2 ≈ 150 - 1.25 × PaCO2
A-a Gradient
A-a gradient = PAO2 - PaO2
- Normal: < 10-15 mm Hg (increases with age; rough formula: age/4 + 4)
- Widened A-a gradient = V/Q mismatch, shunt, or diffusion defect
- Normal A-a gradient with hypoxemia = hypoventilation or high altitude (the problem is low PAO2, not impaired gas exchange)
- Costanzo Physiology, 7th Edition; Medical Physiology
| Cause of Hypoxemia | A-a Gradient | Response to O2 |
|---|---|---|
| Hypoventilation | Normal | Good |
| High altitude | Normal | Good |
| V/Q mismatch | Widened | Good |
| Diffusion defect | Widened | Good |
| Shunt | Widened | Poor/no response |
6. Mixed Acid-Base Disorders
When compensation is inappropriate or the values fall outside the acid-base map confidence zones, consider a mixed disorder.
| Mixed Disorder | Classic Clinical Scenario |
|---|---|
| Metabolic acidosis + Respiratory alkalosis | Salicylate toxicity, sepsis, hepatic failure |
| Metabolic alkalosis + Respiratory alkalosis | Cirrhosis + vomiting; mechanically ventilated + diuretics |
| Metabolic alkalosis + Respiratory acidosis | COPD exacerbation with cor pulmonale; decompensated heart failure with aggressive diuresis |
| AG acidosis + non-AG acidosis | Δ/Δ < 1 (e.g., DKA + diarrhea; ketoacidosis recovering with saline) |
| AG acidosis + metabolic alkalosis | Δ/Δ > 2 (e.g., DKA + vomiting; DKA + pre-existing alkylosis) |
- Comprehensive Clinical Nephrology, 7th Edition
7. Worked Clinical Examples
Example A: Pure Metabolic Acidosis (DKA)
- Values: pH 7.10, PaCO2 20, HCO3- 6, Na 138, Cl 100
- Step 1: pH < 7.35 → acidemia
- Step 2: HCO3- low → metabolic acidosis
- Step 3: Winter's formula: expected PaCO2 = (1.5 × 6) + 8 = 17 ± 2. Actual = 20 → within range, appropriate compensation
- Step 4: AG = 138 - (100 + 6) = 32 (elevated AG acidosis)
- Δ/Δ = (32-12)/(24-6) = 20/18 = 1.1 → pure AG acidosis → DKA, lactic acidosis, uremia, or toxin
Example B: Respiratory Alkalosis (Sepsis)
- Values: pH 7.49, PaCO2 25, HCO3- 22
- Step 1: pH > 7.45 → alkalemia
- Step 2: PaCO2 low → respiratory alkalosis
- Step 3: Expected decrease in HCO3-: 2 mEq/L per 10 mm Hg decrease in PaCO2. PaCO2 fell 15 mm Hg → expected HCO3- fall = 3 mEq/L → expected HCO3- = 25 - 3 = 22 → actual 22 → appropriate acute respiratory alkalosis
- Clinical context: Sepsis, fever, pain, anxiety → hyperventilation
Example C: Mixed AG Acidosis + Respiratory Alkalosis (Salicylate Toxicity)
- Values: pH 7.42 (near normal), PaCO2 15, HCO3- 10
- Step 2: HCO3- low → metabolic acidosis. PaCO2 also low, would expect acidosis but pH is near normal
- Step 3: Winter's: expected PaCO2 = (1.5 × 10) + 8 = 23 ± 2. Actual PaCO2 = 15 → lower than expected → concurrent respiratory alkalosis
- AG: Elevated → MUDPILES/GOLDMARK → consider salicylate poisoning (classic mixed pattern)
8. ABG in Special Clinical Contexts
| Context | Key ABG Findings |
|---|---|
| COPD exacerbation | Respiratory acidosis (acute-on-chronic); HCO3- elevated from chronic compensation; never normalize CO2 acutely |
| Pulmonary embolism | Respiratory alkalosis (hyperventilation), hypoxemia, widened A-a gradient |
| DKA | High AG metabolic acidosis, Kussmaul respirations (compensatory hyperventilation) |
| Lactic acidosis/sepsis | High AG metabolic acidosis ± respiratory alkalosis |
| Vomiting/NG suction | Metabolic alkalosis (loss of HCl) |
| Diarrhea | Normal AG (hyperchloremic) metabolic acidosis (loss of HCO3-) |
| Renal tubular acidosis | Normal AG metabolic acidosis (urine AG helps distinguish types) |
| Methanol/Ethylene glycol | High AG acidosis + elevated osmolal gap |
Osmolal gap check for toxic ingestions:
Osmolal gap = Measured serum osmolality - Calculated osmolality Calculated Osm = 2×Na + BUN/2.8 + Glucose/18 Normal gap < 10 mOsm/kg. An elevated gap + elevated AG = methanol or ethylene glycol until proven otherwise.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
9. Quick Reference Card
Normal ABG: pH 7.35-7.45 | PaCO2 35-45 | HCO3- 22-26 | PaO2 80-100
Acidemia (pH < 7.35):
PaCO2 ↑ → Respiratory acidosis
HCO3- ↓ → Metabolic acidosis
Alkalemia (pH > 7.45):
PaCO2 ↓ → Respiratory alkalosis
HCO3- ↑ → Metabolic alkalosis
Compensation rules (never overcorrects):
Met acidosis → PCO2 = (1.5 × HCO3) + 8 ± 2 [Winter's]
Met alkalosis → PCO2 ↑ 0.7 per 1 HCO3 ↑
Resp acidosis acute → HCO3 ↑ 1 per 10 CO2 ↑
Resp acidosis chronic → HCO3 ↑ 4 per 10 CO2 ↑
Resp alkalosis acute → HCO3 ↓ 2 per 10 CO2 ↓
Resp alkalosis chronic→ HCO3 ↓ 4 per 10 CO2 ↓
AG = Na - (Cl + HCO3) → normal 8-12
Correct for albumin: AG + 2.5 × (4 - albumin)
Δ/Δ = (AG-12)/(24-HCO3): <1 mixed; 1-2 pure AG; >2 concurrent alkalosis
A-a gradient = PAO2 - PaO2 (normal < 15 mm Hg)
PAO2 = 150 - 1.25 × PaCO2 (room air, sea level)
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine | Symptom to Diagnosis, 4th Ed. | National Kidney Foundation Primer on Kidney Diseases, 8e | Comprehensive Clinical Nephrology, 7th Ed. | Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e | Costanzo Physiology, 7th Ed. | Medical Physiology (Boron & Boulpaep) | Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.