Colon diverticulitis
Reading File
Finding Sources
Searching PubMed
"diverticulitis" AND "colon"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive material across multiple textbooks plus recent PubMed evidence. Let me compile the full answer.
Colon Diverticulitis
Definition
Diverticulitis is inflammation and/or infection of a diverticulum (an outpouching of the colonic wall). It is classified as uncomplicated (localized inflammation without major sequelae) or complicated (associated with abscess, fistula, obstruction, or free perforation). Roughly 80% of first attacks are uncomplicated.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
Epidemiology
-
Diverticulitis develops in approximately 4% of patients with known diverticulosis over an 11-year period (older estimates of 10-25% risk are now considered overestimates).
-
Prevalence of diverticulitis hospitalizations in the USA peaked around 2008 and has since stabilized.
-
The proportion of patients requiring surgery decreased from ~25% to ~15% between 2000 and 2010.
-
In Western populations, ~95% of diverticula occur in the sigmoid/left colon. In Asian populations, right-sided diverticula predominate.
-
Sleisenger and Fordtran's
Pathophysiology
The mechanism parallels appendicitis: a fecalith obstructs the neck of a diverticular sac, abrading the mucosa and causing low-grade inflammation. This leads to:
- Increased local bacterial flora
- Diminished venous outflow and localized ischemia
- Altered mucosal defense (defective CD2-induced apoptosis in lamina propria lymphocytes, upregulating local immunity - similar to IBD)
- Possible CMV reactivation (found in >2/3 of affected bowel segments in diverticulitis)
- Transmural bacterial extension -> microperforation
Extent of perforation determines clinical behavior:
-
Microperforation - contained by pericolic fat -> small pericolic abscess
-
Larger perforation - extensive abscess, possible fistula or obstruction
-
Free perforation -> bacterial or fecal peritonitis (incidence ~4/100,000/year)
-
Sleisenger and Fordtran's
Hinchey Classification of Diverticular Perforation
| Stage | Definition |
|---|---|
| I | Confined pericolic abscess |
| II | Distant abscess (retroperitoneal or pelvic) |
| III | Generalized purulent peritonitis from rupture of pericolic/pelvic abscess (diverticular neck obliterated) |
| IV | Fecal peritonitis from free perforation of a diverticulum (communicating with colonic lumen) |
- Sleisenger and Fordtran's
Clinical Features
Uncomplicated diverticulitis:
- LLQ abdominal pain (constant or intermittent) - the hallmark
- Change in bowel habits (diarrhea or constipation)
- Low-grade fever
- Anorexia, nausea, vomiting
- "Sympathetic cystitis" - dysuria/urinary frequency from bladder irritation by inflamed sigmoid
- LLQ tenderness on exam; possible palpable mass; guarding/rebound
- Note: BRBPR is NOT seen in acute diverticulitis
Right-sided diverticulitis (more common in Asian patients): mimics appendicitis closely - RLQ pain and tenderness.
Complicated diverticulitis - additional features:
- Diffuse tenderness with rebound/guarding -> perforation or abscess rupture
- Dysuria + fecaluria -> colovesical fistula
- Feculent vaginal discharge -> colovaginal fistula
- Palpable mass -> localized abscess
- Vomiting + distension -> obstruction
- High fever / sepsis
Elderly and immunocompromised patients may present subtly despite severe disease; perforation is more frequent and carries high mortality.
- Sleisenger and Fordtran's; Rosen's Emergency Medicine
Diagnosis
Imaging
CT scan with IV contrast (and ideally oral/rectal contrast) is the standard of care - sensitivity 98%, specificity 99%.
CT findings:
- Colonic wall thickening
- Pericolic fat stranding
- Localized microperforation
- Abscess formation
- Free air or fluid (perforation)
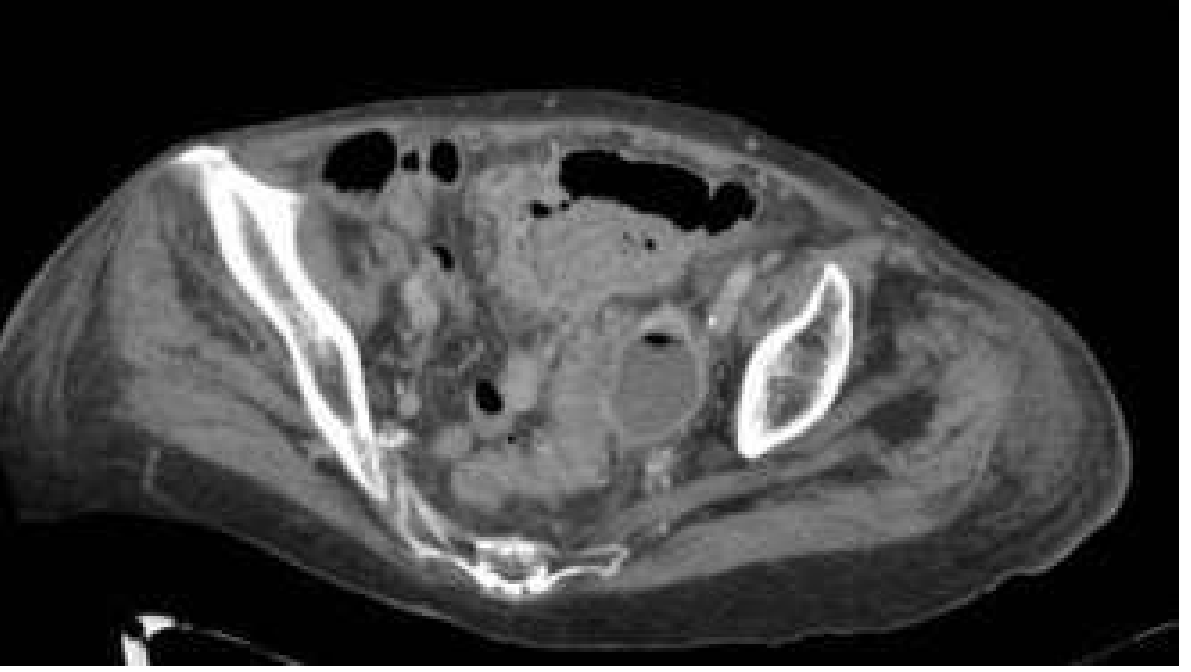
CT of uncomplicated diverticulitis - axial view showing air-filled diverticula along the left colon and hazy outer bowel wall (fat stranding):

CT of diverticulitis with abscess - axial view demonstrating a sigmoid abscess:
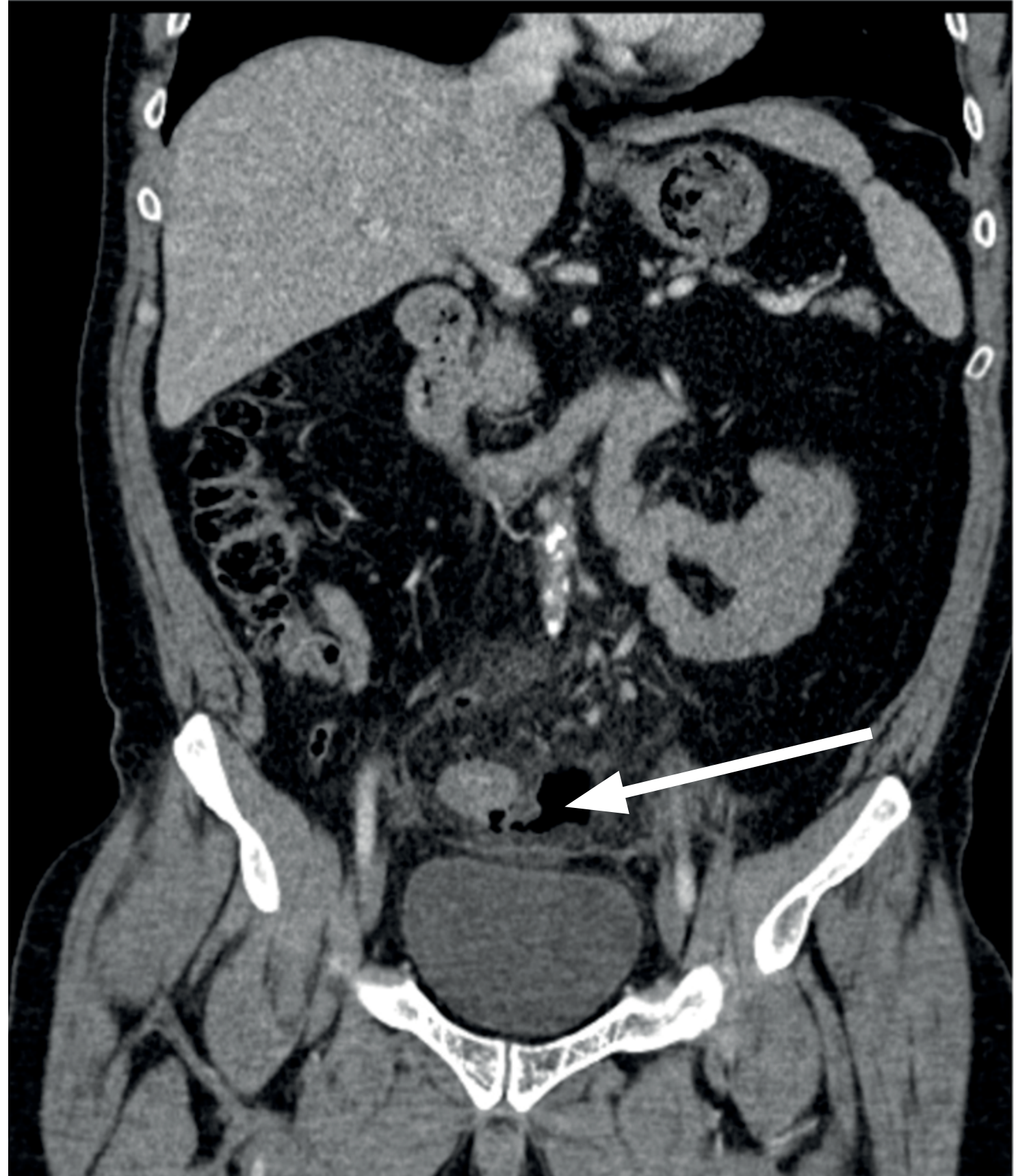
Coronal CT showing diverticular perforation with extraluminal gas track (arrow) and surrounding sigmoid stranding - note this is localized rather than generalized pneumoperitoneum:
Modalities no longer recommended: barium enemas, water-soluble contrast enemas, plain radiography, routine colonoscopy after each episode (now follow age-appropriate cancer screening guidelines).
Lab Work
-
WBC elevated in most but normal WBC in up to 46% - does not exclude diagnosis
-
Urinalysis when colovesical fistula suspected
-
Sleisenger and Fordtran's; Rosen's Emergency Medicine; Bailey and Love's Surgery
Differential Diagnosis
| Condition | Key distinguishing feature |
|---|---|
| Appendicitis | RLQ pain; most common misdiagnosis for right-sided diverticulitis |
| Colorectal cancer | Insidious onset; weight loss; evaluate after acute episode resolves |
| IBD (Crohn's/UC) | Younger patients; rectal involvement; histology |
| Ischemic colitis | Acute-onset rectal bleeding; vascular risk factors |
| Infectious colitis | Diarrhea, stool cultures |
| Pelvic pathology | Women: PID, ovarian cyst rupture, ectopic pregnancy |
| Ureteral stones | Colicky flank pain, hematuria |
Management
Uncomplicated Diverticulitis
Key paradigm shift: Current evidence (AGA guidelines 2015 onward) supports diverticulitis as primarily an inflammatory, not infectious process. Routine antibiotics are not required in uncomplicated cases - they are used selectively.
Outpatient (majority of uncomplicated cases):
- Liquid/low-residue diet, advance as tolerated
- Oral analgesics
- Selective antibiotics (if used): cover Gram-negative aerobes AND anaerobes (e.g., metronidazole + ciprofloxacin; or amoxicillin-clavulanate)
- No benefit of IV over oral antibiotics for uncomplicated disease
Inpatient (IV antibiotics + bowel rest) indicated for:
- Elderly or immunocompromised patients
- Multiple comorbidities
- Unable to tolerate oral intake
- Failure of outpatient therapy
- First episode with diagnostic uncertainty
Recurrence risk: 15-30% after first attack; half of second attacks occur within 1 year.
Complicated Diverticulitis
Abscess (Hinchey I/II):
- Stage I (<3-4 cm): may resolve with antibiotics alone + bowel rest
- Stage II (>3-4 cm or pelvic): CT-guided percutaneous drainage - success rate 74-80% for patient stabilization, allowing later single-stage resection in 3-4 weeks
- 20-25% require urgent surgery (multiloculated, inaccessible, or non-resolving abscess)
Free Perforation (Hinchey III/IV):
- Emergency surgery required
- Options: Hartmann's procedure (sigmoid resection + end colostomy) vs. primary anastomosis (with or without protective stoma)
- A recent 2025 meta-analysis on primary anastomosis in emergency left colon surgery supports safety of primary anastomosis without protective stoma in selected patients
Fistula:
- Develops in <5% of all diverticulitis cases but ~20% of surgical cases
- Colovesical fistula is the most common (men > women due to uterus acting as barrier)
- Treatment: elective surgical resection after bowel prep and preoperative cystoscopy/urologic evaluation
Obstruction:
- Colonic obstruction from stricture or inflammatory mass
- Acute: IV fluids, bowel decompression, consider stenting vs. surgery
- Chronic stricture: elective resection
Elective Surgery - Indications
- Recovery from complicated diverticulitis (abscess/fistula/obstruction)
- Recurrent symptomatic disease significantly impairing quality of life
- Inability to exclude carcinoma
Approach: Elective laparoscopic sigmoid colectomy is the preferred approach (shorter hospital stay, lower costs than open colectomy; considered standard of care). A 2025 meta-analysis found no significant difference in quality of life between elective surgery and non-operative management for uncomplicated recurrent diverticulitis, reinforcing selective surgical referral.
- Sleisenger and Fordtran's; Rosen's Emergency Medicine; Bailey and Love's Surgery
Post-Acute Surveillance
- Colonoscopy is not routinely required after each episode
- Follow standard colorectal cancer screening intervals
- High-fiber diet post-recovery (reduces recurrence and symptom burden)
- Physical activity reduces risk of developing diverticulitis (mechanism unclear)
- Previously advised avoidance of nuts/seeds/popcorn has been discredited - no evidence base
Recent Evidence (PubMed 2024-2026)
- A 2025 systematic review and meta-analysis (Kahana et al., Surgery) found no significant QoL advantage of elective surgery over non-operative management for colonic diverticulitis - supports conservative management as first-line for most recurrent cases.
- A 2026 systematic review (Sassun et al., Colorectal Dis) found low rates of recurrent diverticulitis after sigmoid resection, supporting surgery in high-recurrence-risk patients.
- Genetic determinants of diverticulosis are increasingly recognized, with connective tissue genes implicated - relevant to younger patients with early-onset disease.
This is a shared conversation. Sign in to Orris to start your own chat.