pancreatitis
pancreatitis etiology diagnosis classification severity
pancreatitis management treatment complications
pancreatitis CT imaging findings
Pancreatitis
Etiology
| Cause | Details |
|---|---|
| Gallstones | Most common overall; gallstone migrating through the ampulla of Vater causes transient obstruction |
| Alcohol | Second most common; typically requires years of heavy use |
| Hypertriglyceridemia | Usually >1000 mg/dL; third most common |
| ERCP | Post-procedural pancreatitis (3–5% of cases) |
| Drugs | Azathioprine, thiazides, furosemide, valproate, tetracyclines, etc. |
| Infections | Mumps, CMV, Coxsackievirus |
| Autoimmune | IgG4-related (Type 1) or IDCP (Type 2) |
| Hereditary | PRSS1, SPINK1, CFTR mutations |
| Idiopathic | ~10–20% of cases |
Clinical Presentation
- Pain: Epigastric, often radiating to the back; constant, boring in character; worsens supine, may improve leaning forward
- Nausea and vomiting: Almost universal
- Fever and tachycardia: Common in moderate-severe disease
- Grey Turner's sign (flank ecchymosis) and Cullen's sign (periumbilical ecchymosis): Rare but indicate hemorrhagic pancreatitis
Diagnosis
- Serum amylase >3× ULN or serum lipase >3× ULN (lipase is more sensitive and specific)
- Elevated WBC, CRP, LDH, bilirubin (if biliary cause)
- Elevated creatinine (if AKI develops)
- Ultrasound (US): First-line to identify gallstones and biliary dilation
- CT abdomen (contrast-enhanced): Gold standard for severity assessment; best performed 48–72 hours after symptom onset if diagnosis is unclear or severity is in question
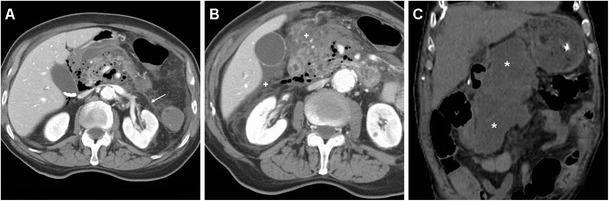
CT Imaging: Necrotizing Pancreatitis
Severity Classification (Revised Atlanta 2013)
| Category | Definition |
|---|---|
| Mild | No organ failure, no local/systemic complications; resolves within 1 week |
| Moderately Severe | Transient organ failure (<48 h) and/or local complications |
| Severe | Persistent organ failure (>48 h); single or multi-organ |
- Ranson criteria: Scored at admission + 48 h; ≥3 = severe
- Glasgow (Imrie) score: ≥3 at 48 h = severe
- APACHE II: Can be applied throughout admission
- CRP >150 mg/L at 48 h: Independent severity marker
- BMI >30: Higher risk of complications
Management
Mild Pancreatitis
- IV fluid resuscitation: Lactated Ringer's preferred over NS (reduces SIRS); 250–500 mL/hr initially
- NPO initially, then early oral feeding as tolerated (within 24–48 h if possible)
- Analgesia: IV opioids (morphine, hydromorphone); multimodal approaches preferred
- Monitoring: Vitals, urine output, labs (BMP, CBC)
Moderate-Severe / Severe Pancreatitis
- ICU-level care if persistent organ failure
- Aggressive fluid resuscitation with close monitoring
- Enteral nutrition (nasojejunal feeding) preferred over TPN; start within 24–72 h
- ERCP: Urgent (<24–72 h) if cholangitis or persistent biliary obstruction
- Antibiotics: NOT prophylactic; only indicated for confirmed infected necrosis
- Surgical/interventional: Step-up approach for infected or symptomatic necrosis — percutaneous drainage → endoscopic/surgical debridement (necrosectomy)
Local Complications
| Complication | Description |
|---|---|
| Acute peripancreatic fluid collection (APFC) | Early (<4 weeks), no defined wall |
| Pseudocyst | Fluid collection with defined wall, >4 weeks, no solid component |
| Acute necrotic collection (ANC) | Early necrosis with fluid and solid material |
| Walled-off necrosis (WON) | Mature, encapsulated necrosis, >4 weeks |
| Infected necrosis | Fever, elevated WBC, gas on CT; requires intervention |
Systemic Complications
- ARDS (most common cause of early death)
- AKI
- DIC
- Hypocalcemia (saponification of fat)
- Hyperglycemia
- Pleural effusions
Chronic Pancreatitis
- Triad: Chronic epigastric pain, steatorrhea, diabetes mellitus
- Imaging: Pancreatic calcifications (pathognomonic), dilated main pancreatic duct
- Management: Pain control (stepwise), pancreatic enzyme replacement therapy (PERT), treat diabetes, alcohol/smoking cessation, endoscopic or surgical decompression in selected cases
- Lipase is the preferred diagnostic enzyme
- Revised Atlanta 2013 guides severity stratification
- Most cases are mild and self-limiting; aggressive early fluids are the cornerstone of treatment
- Antibiotics are not routine; reserve for proven infected necrosis
- Early enteral nutrition is superior to TPN in severe disease
history: 50y male postptca patient ef 40% , k/c/o dm/htn , p/w h/o fever 5 days a/w chills and rigors , malaria falciparum antigen positive , on norad infusion single strength @5ml/hr nibp 112/80. hr 150 , tacypnea rr of 30-40 , abg s/o ph 7.462 pco2 25, po2 71 na 131 k 3.8 ca 1.16 glucose 207 so2 88.6 anion gap 3.7 , hfnc trial given switched to niv . differential , plan of treatment, tests ...
severe malaria falciparum management ICU treatment artemisinin
malaria falciparum respiratory failure ARDS hypoxemia mechanical ventilation
septic shock norepinephrine hemodynamic management low EF cardiac dysfunction
Critical Illness Summary
ABG Interpretation
| Parameter | Value | Interpretation |
|---|---|---|
| pH | 7.462 | Alkalotic |
| pCO₂ | 25 mmHg | Low → respiratory alkalosis |
| PaO₂ | 71 mmHg | Hypoxemia |
| Na | 131 | Hyponatremia |
| K | 3.8 | Normal |
| Ca (ionized) | 1.16 | Low-normal |
| Glucose | 207 | Hyperglycemia |
| SpO₂ | 88.6% | Significant hypoxemia |
| Anion Gap | 3.7 | Low (hypoalbuminemia likely) |
Differentials for Fever + Respiratory Failure in This Context
| Diagnosis | Likelihood | Key Pointer |
|---|---|---|
| Severe Falciparum Malaria (ARDS + Shock) | ✅ Primary | Positive antigen, multi-organ involvement |
| Superimposed Bacterial Sepsis / CAP | ✅ High | Fever, chills, rigors, shock, tachypnea |
| Malaria-induced Myocarditis / Cardiac Decompensation | ✅ Moderate | EF 40%, post-PTCA, HR 150 |
| Falciparum Malaria Pulmonary Edema | ✅ Moderate | Distinct from ARDS; fluid overload risk high in low-EF |
| HCAP / Ventilator-associated | Moderate | Nosocomial risk |
| COVID-19 / Viral co-infection | Lower | Worth excluding |
| Hyperglycemic crisis contribution | Present | Glucose 207, osmotic effects |
Criteria for Severe Malaria (this patient meets multiple):
- ✅ Respiratory distress / ARDS
- ✅ Circulatory collapse (on norepinephrine)
- ✅ Impaired consciousness (assess GCS)
- Hyperparasitemia (>5%) — check smear urgently
- Hypoglycemia — monitor closely (glucose 207 currently, but can drop rapidly with artesunate + quinine)
- Renal failure — check creatinine
- Jaundice — check bilirubin
- Abnormal bleeding — check PT/aPTT
Investigations — Urgent
Immediate (Stat)
| Test | Purpose |
|---|---|
| Peripheral smear (thick + thin) | Confirm species, quantify parasitemia % |
| Serum lactate | Unmask occult metabolic acidosis, severity |
| CBC with differential | Hemolytic anemia, thrombocytopenia (hallmark of falciparum) |
| LFTs + bilirubin | Jaundice, hepatic malaria |
| Serum creatinine, BUN, urine output | Acute kidney injury (major complication) |
| PT/aPTT/INR, fibrinogen, D-dimer | Coagulopathy, DIC |
| Serum albumin | Correct anion gap, guide nutrition |
| Blood cultures ×2 | Gram-negative bacteremia co-infection |
| Procalcitonin | Bacterial co-infection |
| NT-proBNP / BNP | Cardiac function, volume status |
| Repeat ABG in 1–2 hrs | NIV response monitoring |
| CXR (portable) | Bilateral infiltrates (ARDS vs pulmonary edema) |
| Serum glucose Q2H | Hypoglycemia risk (especially with quinine) |
| Urine RE/ME | Hemoglobinuria ("blackwater fever") |
Within 12–24 Hours
| Test | Purpose |
|---|---|
| ECHO (bedside) | EF reassessment, RV strain, volume status |
| Malaria parasitemia Q12H | Treatment response |
| Repeat electrolytes | Hyponatremia, K+ monitoring |
| G6PD deficiency screen | Before primaquine/radical cure |
| HIV, HBsAg | Baseline immune/co-infection workup |
| Chest HRCT (if CXR equivocal) | ARDS characterization |
| Urinary catheter + strict I/O | Volume management critical in low EF |
Treatment Plan
1. Anti-malarial (Priority 1)
- Dose: 2.4 mg/kg IV at 0, 12, 24 hours, then once daily until oral therapy possible
- Transition to oral Artemisinin-based Combination Therapy (ACT) once tolerating orals:
- Artemether-Lumefantrine (Coartem) OR
- Artesunate + Mefloquine / Doxycycline
- Monitor glucose Q2H — artesunate-associated delayed hemolysis can occur; watch Hb from day 7–28
- Avoid quinine if possible (QTc prolongation risk in post-PTCA patient)
2. Respiratory Management
| Parameter | Target |
|---|---|
| SpO₂ | ≥94% |
| RR | <25/min |
| Work of breathing | Decreasing |
| GCS | ≥12 (NIV safety threshold) |
- NIV settings: IPAP 12–16 cmH₂O, EPAP 8–10 cmH₂O, FiO₂ titrate to SpO₂
- Reassess in 1–2 hours — if no improvement (SpO₂ <90%, RR unchanged, worsening sensorium) → early intubation with lung-protective ventilation
- Tidal volume 6 mL/kg IBW
- PEEP 8–12 cmH₂O (titrate via P-V tool or empiric)
- Plateau pressure <30 cmH₂O
- Prone positioning if PaO₂/FiO₂ <150 despite optimization
- Caution with fluids: EF 40% + ARDS = high risk of flash pulmonary edema; target conservative fluid strategy guided by BNP + ECHO
3. Hemodynamic / Vasopressor Management
- Norepinephrine already running — titrate to MAP ≥65 mmHg (or ≥70 mmHg given EF 40%)
- If norad >0.25 mcg/kg/min → add Vasopressin 0.03 units/min (vasopressor-sparing, reduces norad dose)
- Dobutamine: Consider if low cardiac output state (post-PTCA, EF 40%, cold peripheries, high lactate) — start 2.5–5 mcg/kg/min
- Avoid volume loading — high risk of pulmonary edema in EF 40%
- Check ECHO urgently to differentiate:
- Distributive shock (warm, low SVR) — malaria/sepsis
- Cardiogenic component (cold, low CO) — EF 40% decompensation
4. Fluid & Electrolyte Management
| Issue | Action |
|---|---|
| Hyponatremia (Na 131) | Likely dilutional/SIADH in severe malaria; restrict free water; correct slowly; avoid aggressive NS (hyperchloremia risk) |
| Hypocalcemia (Ca 1.16) | Replace IV calcium gluconate if symptomatic or worsening; monitor ECG |
| Hyperglycemia (207) | IV insulin infusion targeting 140–180 mg/dL; avoid hypoglycemia aggressively |
| Hypokalemia risk | K⁺ 3.8 currently — monitor closely, replace if drops <3.5 |
| Fluids | Use balanced crystalloids (LR preferred); strict I/O; urine output target >0.5 mL/kg/hr |
5. Antibiotic Cover
- Start empiric broad-spectrum antibiotics given septic shock picture (cannot exclude bacterial co-infection):
- Piperacillin-Tazobactam 4.5g IV Q6H (or Meropenem if high ESBL risk)
- +/- Azithromycin (covers atypicals, also has anti-malarial properties)
- De-escalate based on cultures at 48–72 hours
6. Cardiac Monitoring & Protection
- Continuous ECG monitoring (QTc — especially relevant for any anti-malarial)
- Avoid QTc-prolonging drugs wherever possible
- Statin continuation (if on one for post-PTCA)
- Hold ACE inhibitor / ARB if hypotensive
- Aspirin: Continue if on it post-PTCA, assess bleeding risk vs. thrombotic risk
- Beta-blocker: Hold or reduce if hemodynamically unstable / HR 150 with shock; re-evaluate once stable
- HR 150 — rule out AF with RVR (common in sepsis + malaria): 12-lead ECG urgently; if AF → rate control cautiously (amiodarone preferred in low EF)
7. Additional Supportive Care
| Issue | Intervention |
|---|---|
| DVT prophylaxis | Mechanical (pneumatic compression) initially; anticoagulate once bleeding risk assessed |
| Stress ulcer prophylaxis | IV PPI (pantoprazole) |
| Glycemic control | IV insulin infusion; Q1–2H glucose monitoring |
| Nutrition | Early enteral nutrition via NG once hemodynamically stable |
| Renal monitoring | Foley catheter in-situ; if AKI develops → consider RRT early |
| Transfusion | If Hb <7 g/dL (or <8 in cardiac patient); falciparum causes significant hemolysis |
| Platelet transfusion | If <10k (or <50k with active bleeding); thrombocytopenia expected |
Red Flags to Watch — Deterioration Triggers
| Sign | Action |
|---|---|
| SpO₂ <90% on NIV / worsening WOB | Intubate immediately |
| GCS drop | Cerebral malaria — intubate, urgent CT head |
| Urine output <0.5 mL/kg/hr | Aggressive AKI workup, early RRT |
| Glucose <70 mg/dL | IV dextrose bolus; adjust insulin |
| MAP <65 on ≥0.25 mcg/kg/min norad | Add vasopressin ± dobutamine |
| Worsening coagulation | Manage DIC — FFP, cryoprecipitate |
| New hemoglobinuria (dark urine) | Blackwater fever — aggressive hydration, avoid quinine |
Summary of Immediate Priorities
- IV Artesunate — start immediately (do not delay for investigations)
- Peripheral smear — confirm parasitemia %
- Serum lactate + cultures + CBC — stat
- NIV optimization — reassess in 1–2 hrs; low threshold to intubate
- Bedside ECHO — differentiate distributive vs. cardiogenic shock
- Broad-spectrum antibiotics — empiric cover
- 12-lead ECG — rule out AF, QTc monitoring
- Strict glycemic control and I/O monitoring