Obstructive and restrictive as per GK PAL
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have excellent content. Let me note that GK Pal's textbook is not in the library, but I have comprehensive coverage from Ganong's (physiology), Robbins (pathology), and Barash (anesthesia/clinical). These cover the same content as GK Pal since the physiology principles are universal. Let me compose a thorough answer.
Note: GK Pal's Textbook of Medical Physiology is not in the available library. The content below is drawn from equivalent authoritative physiology and pathology texts (Ganong's Review of Medical Physiology and Robbins Basic Pathology) covering the same topic. The principles are identical.
Obstructive vs. Restrictive Lung Disease - Spirometry & PFT Patterns
Definitions
| Type | Core Defect |
|---|---|
| Obstructive | Increased resistance to airflow - partial or complete obstruction at any airway level |
| Restrictive | Reduced expansion of lung parenchyma - decreased total lung capacity |
- Robbins Basic Pathology, p. 447
Spirometry (FEV1/FVC) - The Key Diagnostic Test
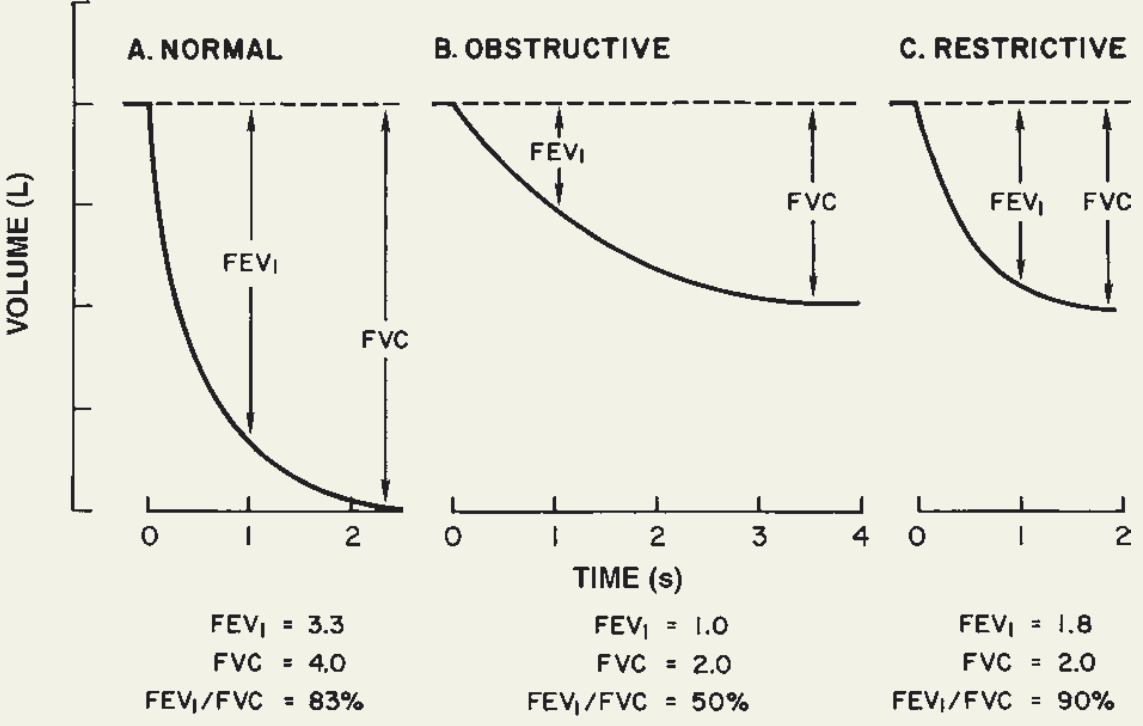
The spirogram above (from Ganong's Review of Medical Physiology, 26th ed.) shows the hallmark differences:
| Parameter | Normal | Obstructive | Restrictive |
|---|---|---|---|
| FEV1 | ~3.3 L | ~1.0 L (markedly ↓) | ~1.8 L (↓ but less so) |
| FVC | ~4.0 L | ~2.0 L (↓) | ~2.0 L (↓) |
| FEV1/FVC | ~80-83% | ~50% (↓↓↓) | ~90% (normal or ↑) |
- Ganong's Review of Medical Physiology, 26th Ed.
Key Distinguishing Logic
Obstructive disease:
- The expiratory curve shows a slow, steady slope - airflow is impeded throughout expiration
- FEV1 is markedly reduced (small amount exhaled in first second due to obstruction)
- FVC is also reduced (patients cannot fully empty even with prolonged effort) or slightly decreased
- FEV1/FVC < 0.70 is the hallmark (cutoff for obstructive diagnosis)
- The curve takes >4 seconds to approach FVC
Restrictive disease:
- The expiratory curve shows rapid initial flow that quickly plateaus - the lungs are small but airways are open
- FEV1 is reduced proportionally
- FVC is markedly reduced (small lung volumes)
- FEV1/FVC is normal or even elevated (both fall proportionately, ratio preserved)
- The curve reaches FVC quickly (~2 seconds), just at a lower total volume
Full PFT Comparison Table
(from Barash Clinical Anesthesia, 9th ed.)
| Parameter | Restrictive Disease | Obstructive Disease |
|---|---|---|
| Definition | Proportional decreases in all lung volumes | Small airway obstruction to expiratory flow |
| FVC | ↓↓↓ | Normal or slightly ↑ |
| FEV1 | ↓↓↓ | Normal or slightly ↓ |
| FEV1/FVC | Normal | ↓↓↓ |
| FEF25-75% | Normal | ↓↓↓ |
| FRC | ↓↓↓ | Normal or ↑ (gas trapping) |
| TLC | ↓↓↓ | Normal or ↑ (gas trapping) |
Causes
Obstructive (major 4):
- Emphysema - loss of elastic recoil, air trapping, enlarged air spaces
- Chronic bronchitis - mucus hypersecretion, airway narrowing
- Asthma - bronchoconstriction, airway hyperresponsiveness (partially reversible)
- Bronchiectasis - irreversible bronchial dilation, chronic infection
Emphysema + chronic bronchitis together = COPD (most common combination; cigarette smoking is the major cause)
Restrictive (two broad categories):
- Chest wall/extrapulmonary - severe obesity, pleural diseases, neuromuscular disorders (e.g., Guillain-Barre syndrome)
- Intrinsic lung parenchymal:
- Acute: ARDS (classic acute restrictive disease)
- Chronic: pneumoconioses, idiopathic pulmonary fibrosis (IPF), sarcoidosis, other interstitial lung diseases
Pathophysiology of Ventilation Nonuniformity
-
Restrictive: Decreased static compliance (e.g., fibrosis) halves the ΔV of affected alveoli for the same pressure change - less ventilation delivered locally
-
Obstructive: Increased airway resistance raises the time constant (τ = R × C) for filling/emptying. With short breath cycles (increased respiratory rate), affected alveoli cannot fully fill or empty, worsening ventilation/perfusion mismatch
-
Medical Physiology (Boron & Boulpaep), p. 1009
Summary Mnemonics
| Obstructive | Restrictive | |
|---|---|---|
| FEV1/FVC | Low (<0.70) | Normal/High |
| TLC | ↑ (air trapping) | ↓ |
| Airway resistance | ↑↑ | Normal |
| Compliance | ↑ (emphysema) or normal | ↓ (fibrosis) |
| Reversibility | Partial (asthma) | No |
This is a shared conversation. Sign in to Orris to start your own chat.