Tendons Achilles tenotomy
Reading File
Finding Sources
Finding Sources
Searching PubMed
Achilles tenotomy clubfoot Ponseti
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have all the content needed for a thorough answer. Here is the complete overview:
Achilles Tenotomy (Tendo-Achilles Tenotomy - TAT)
What Is It?
Achilles tenotomy is the surgical division (cutting) of the Achilles (calcaneal) tendon. In the context of the Ponseti method for clubfoot (CTEV - congenital talipes equinovarus), it refers specifically to a percutaneous tenotomy - a minimally invasive division performed through a tiny stab incision at the skin. It is one of the most common minor procedures in paediatric orthopaedics.
Primary Indication: Clubfoot (CTEV)
The Ponseti method corrects the four components of clubfoot in the sequence captured by the mnemonic CAVE:
| Step | Deformity Corrected |
|---|---|
| C | Cavus - elevation of first ray |
| A | Adduction - gradual forefoot abduction to 60° |
| V | Varus - correction of hindfoot varus |
| E | Equinus - corrected last, usually requiring Achilles tenotomy |
Equinus is addressed after the first three components because trying to dorsiflex the foot before correcting the varus and adduction causes a rocker-bottom deformity.
The Ponseti method is successful in ~95% of feet when success is defined as avoiding formal surgical release. (Bailey & Love's Surgery, 28th Ed)
When is Tenotomy Needed?
The majority of cases - approximately 70-80% of infants treated with the Ponseti method - require percutaneous Achilles tenotomy before application of the final (last) cast to:
- Achieve the goal of 15 degrees of ankle dorsiflexion
- Allow the foot to reach ~70 degrees of abduction
- Prevent a rocker-bottom deformity by achieving true ankle dorsiflexion (not through the midfoot)
"In most children, to be able to achieve maximal abducted position of the foot with the ankle dorsiflexed 15 degrees, a percutaneous Achilles tenotomy is necessary." - Campbell's Operative Orthopaedics, 15th Ed 2026
Other Indications
- Congenital Vertical Talus (CVT): Serial manipulation and casting followed by percutaneous Achilles tenotomy and minimal talonavicular capsulotomies and pin fixation (Miller's Review of Orthopaedics, 9th Ed)
- Recurrent clubfoot after Ponseti casting: Repeat casting with or without tenotomy
- Spasticity / upper motor neuron syndrome: Achilles tendon lengthening (more commonly Z-plasty or open lengthening rather than complete tenotomy in this context)
- Cerebral palsy / neuromuscular conditions: Tenotomy/lengthening as part of multi-level surgical correction
Percutaneous Achilles Tenotomy - Technique (Ponseti Method)
Setting
- Can be performed in the clinic under local skin anaesthesia (topical or injected), or in the operating room under sedation/general anaesthesia
- Clinic setting: avoids need for fasting and general anaesthesia
- OR setting: easier control of any excess bleeding
Steps
- The foot is held in maximum abduction and beginning dorsiflexion
- A small open incision (not purely "blind" percutaneous) is made directly over the medial border of the tendon, just proximal to its insertion on the calcaneus
- The tenotomy is performed from medial to lateral (Fig. 31.31 in Campbell's)
- A rounded Beaver eye blade is recommended to reduce risk of vascular injury
- A palpable / audible "snap" confirms complete division
- The final cast is then applied with the foot at ~70 degrees of abduction and 15 degrees of dorsiflexion and held for 3 weeks while the tendon regenerates
Key Safety Note
"Bleeding complications have been reported after percutaneous tenotomy from injury to the peroneal artery or the lesser saphenous vein. Make a small open incision directly over the tendon before severing it, making the tenotomy from medial to lateral." - Campbell's Operative Orthopaedics, 15th Ed 2026
Clubfoot Treatment Algorithm
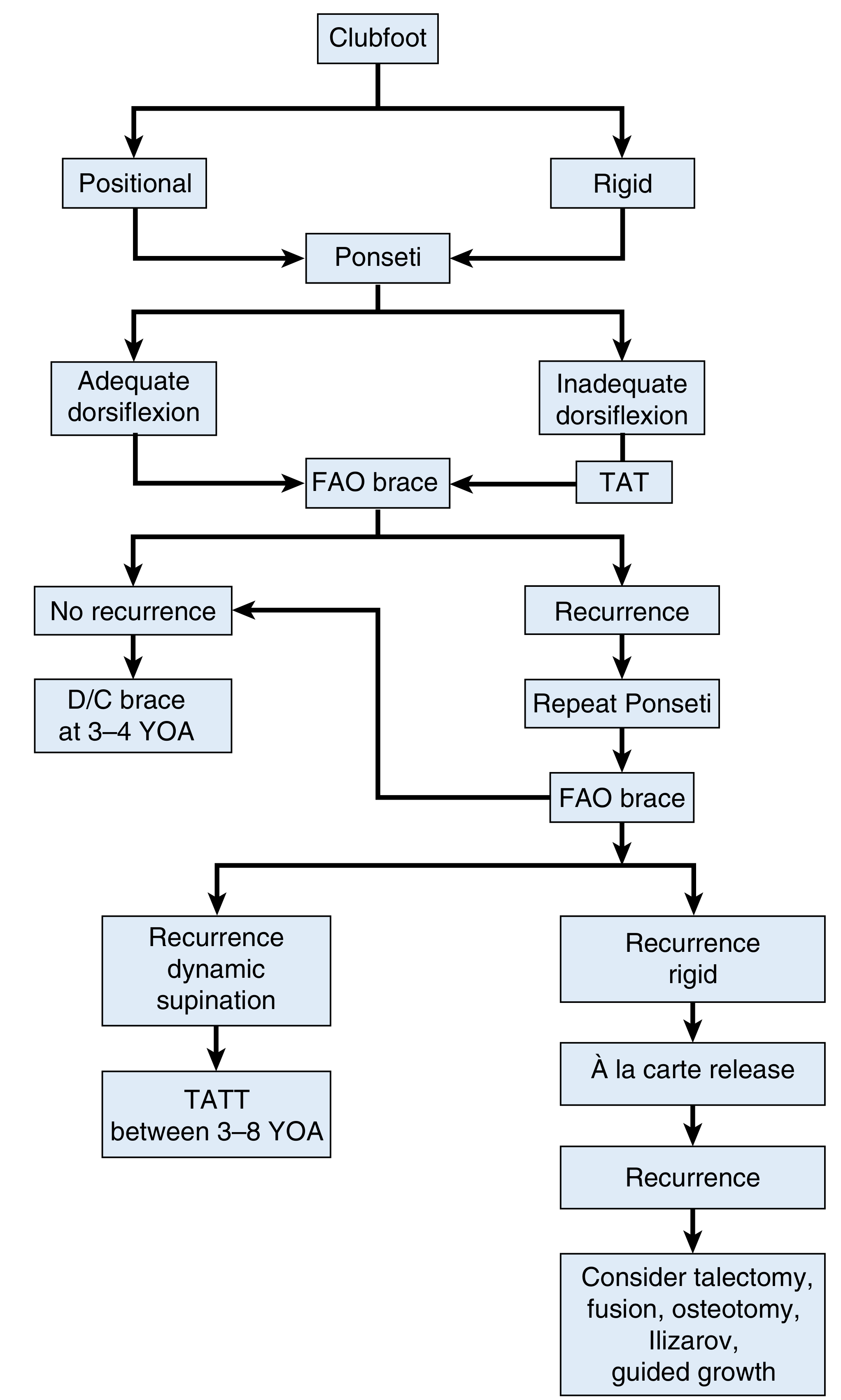
FIGURE 31.29 - Treatment algorithm for clubfoot deformity. FAO = Foot Abduction Orthosis; TAT = Tendo-Achilles Tenotomy; TATT = Tibialis Anterior Tendon Transfer; YOA = Years of Age. (Campbell's Operative Orthopaedics, 15th Ed 2026)
Post-Tenotomy Care (Maintenance Phase)
| Period | Brace Protocol |
|---|---|
| First 3 months after casting | 23 hours/day in foot abduction orthosis (FAO) |
| Up to 3-4 years of age | During sleep only |
| Beyond 4 years | Based on recurrence risk |
- The foot abduction orthosis (FAO) holds feet at 70° external rotation and 15° dorsiflexion
- Distance between shoes = ~1 inch wider than the child's shoulder width
- Bilateral bracing is superior to unilateral bracing
- Brace compliance is the single most important factor in preventing recurrence
Key Points Summary
- Tenotomy is performed at the end of casting (after CAVE correction), before the final cast
- Required in most (~80%) Ponseti-treated clubfeet
- Tendon regenerates within the 3-week final cast period - it does not leave a permanent gap
- The Achilles is associated with absence/diminution of the anterior tibial artery in clubfoot
- Recurrence rate with Ponseti: 10-30%; recurrent deformity is treated with repeat casting ± repeat tenotomy
- If recurrence is rigid and fails repeat casting: tibialis anterior tendon transfer (TATT) at 3-8 years of age, or à la carte surgical release
- Beyond that, options include talectomy, fusion, osteotomy, Ilizarov, or guided growth
Sources:
- Campbell's Operative Orthopaedics, 15th Ed 2026, Chapter 31 (Ponseti Technique 31.10)
- Miller's Review of Orthopaedics, 9th Ed, Section 5 - Foot (Clubfoot)
- Bailey & Love's Short Practice of Surgery, 28th Ed, Chapter 44 (Summary Box 44.13)
- Recent systematic review: Ponseti method in neurogenic clubfoot (2025, PMID 41272751) confirms broad applicability of the method including tenotomy
CTEV AND PONSETTI
Finding Sources
Finding Sources
Searching PubMed
congenital talipes equinovarus Ponseti method
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from the textbooks for a complete answer. Here is the full, structured overview:
Congenital Talipes Equinovarus (CTEV) and the Ponseti Method
Clinical Picture - Newborn Clubfoot

FIGURE 31.25 - Congenital clubfoot in newborn: inversion, plantarflexion, internal rotation of calcaneus, and cavus deformity with transverse plantar crease. (Campbell's Operative Orthopaedics, 15th Ed 2026)
1. Definition
Congenital Talipes Equinovarus (CTEV) is a complex three-dimensional foot deformity present at birth, characterized by four inseparable components summarized by the mnemonic CAVE:
| Letter | Deformity | Description |
|---|---|---|
| C | Cavus | High medial arch; first ray plantarflexed |
| A | Adductus | Forefoot adduction (medial deviation) |
| V | Varus | Hindfoot inverted/supinated |
| E | Equinus | Plantarflexion of the ankle (foot points downward) |
The deformity varies from mild and passively correctable (positional) to rigid and resistant.
2. Incidence
- 1 in 1000 live births (one of the most common congenital orthopaedic conditions)
- Bilateral in 50% of cases; severity is highly correlated between both feet in bilateral cases
- Unilateral cases are evenly distributed between right and left sides
- No proven association with developmental dysplasia of the hip (DDH)
- More common in males (2:1 ratio)
3. Aetiology
The exact cause remains unknown, but proposed theories include:
- Primary germplasm defect in the talus - causing continued plantarflexion and inversion, with secondary soft-tissue changes
- Primary soft-tissue/neuromuscular abnormality - causing secondary bony changes
- Vascular theory - many children with clubfoot have a hypertrophic anterior tibial artery or diminutive/absent anterior tibial artery; other vascular anomalies are common
- Muscle fibre abnormality - abnormal distribution of type I and type II muscle fibres documented
Risk factors / associations:
- Maternal and paternal smoking
- Maternal obesity
- Family history (autosomal dominant with incomplete penetrance)
- Amniocentesis
- Some SSRIs (selective serotonin reuptake inhibitors)
- Spina bifida, arthrogryposis, chromosomal abnormalities (non-idiopathic clubfoot)
4. Pathoanatomy
The primary bony deformity involves the talus:
- Talar neck is internally rotated relative to the ankle mortise
- Talar body is externally rotated in the mortise
- Calcaneus is significantly internally rotated
Soft-tissue contractures resist correction:
| Structure | Deformity resisted |
|---|---|
| Posterior tibial tendon, deltoid ligament, spring ligament, talonavicular capsule | Talonavicular subluxation |
| Calcaneofibular ligament, superior peroneal retinaculum | Talocalcaneal realignment |
| Long plantar ligament, bifurcated Y-ligament, plantar calcaneocuboid ligament | Calcaneocuboid joint rotation |
| Achilles tendon | Equinus |
If left untreated: fused joints, contractures, severe degenerative changes, and functional disability.
5. Clinical Assessment
Physical examination:
- Foot is small, stiff, held in equinus-varus-adductus position
- Transverse plantar crease
- Posterior skin crease
- Calf muscle wasting (smaller calf on affected side)
- Assess passivity / rigidity (distinguish positional from structural)
Scoring systems (no radiology needed for initial assessment):
| System | Parameters | Score range | Higher = worse |
|---|---|---|---|
| Pirani | 6 physical findings (hindfoot + midfoot contracture scores), each 0 / 0.5 / 1 | 0-6 | Yes |
| Diméglio | 4 parameters assessed by goniometer for reducibility + 4 additional points | 0-20 | Yes |
6. Radiographic Evaluation
Indicated when deformity is atypical, associated with neurological/genetic condition, or resistant to treatment.
Standard views: Simulated weight-bearing AP + stress dorsiflexion lateral
| Angle | Normal | Clubfoot |
|---|---|---|
| AP talocalcaneal angle | 30-55° | Decreases with varus (can reach 0° = parallelism) |
| Lateral talocalcaneal angle | 25-50° | Decreases toward 0° with severity |
| Tibiocalcaneal angle (lateral) | 10-40° | Negative (equinus of calcaneus) |
| Talus-1st metatarsal angle | 5-15° (AP) | Negative (forefoot adduction) |
7. The Ponseti Method
The gold standard of treatment. Success rate of ~95% in avoiding formal surgical release. (Bailey & Love's, 28th Ed)
Principles
- Begin as early as possible, ideally within the first 4 weeks of life
- Gentle manipulation followed by long leg plaster cast (above knee essential)
- The key manipulation: abduct the foot around the stable talar head (thumb on the lateral head of talus as the fulcrum)
- NEVER pronate the foot; never directly manipulate the heel
- NEVER try to dorsiflex first - correct CAVE in order
Order of Correction: C → A → V → E (CAVE sequence)
| Step | What is corrected | How |
|---|---|---|
| C | Cavus | Elevate the first ray (supinate forefoot to align with heel) |
| A | Adductus | Gradually abduct forefoot up to 60°, with thumb on talar head |
| V | Varus | Simultaneously corrects as foot is abducted; calcaneus everts |
| E | Equinus | Last - percutaneous Achilles tenotomy in ~80% cases |
The heel must NOT be directly manipulated. Forefoot derotation must occur about the talus, not the calcaneocuboid joint.
Number of Casts
- Typically 5-6 casts, each held for ~1 week (accelerated biweekly schedules are also acceptable)
- Long leg casts are essential to maintain external rotation force
- Plaster of Paris and fiberglass have similar outcomes
Step 6: Percutaneous Achilles Tenotomy
- Required in ~80% of infants to achieve 15° dorsiflexion
- Corrects the residual equinus that cannot be fully addressed by casting alone
- Can be done in clinic (local anaesthesia) or OR (sedation/GA)
- Technique: medial-to-lateral tenotomy through small incision over medial tendon border; Beaver eye blade recommended
- Risks: peroneal artery injury, lesser saphenous vein injury
- Final cast applied for 3 weeks at 70° abduction / 15° dorsiflexion
- Tendon regenerates during the 3-week cast period
8. Treatment Algorithm
Clubfoot treatment algorithm. FAO = Foot Abduction Orthosis; TAT = Tendo-Achilles Tenotomy; TATT = Tibialis Anterior Tendon Transfer; YOA = Years of Age. (Campbell's Operative Orthopaedics, 15th Ed 2026)
9. Maintenance Phase (Foot Abduction Orthosis - FAO)
After the final cast is removed:
| Period | Protocol |
|---|---|
| First 3 months | FAO worn 23 hours/day |
| Age 3-4 years | FAO worn during sleep only |
| Beyond 4 years | Discontinue (recent evidence supports extending to 4 years) |
FAO specifications:
- Shoes fixed to a bar at 70° external rotation and 15° dorsiflexion
- Bar width = ~1 inch wider than the infant's shoulder width
- Bilateral bracing is superior to unilateral
Brace compliance is the single most important factor in preventing recurrence. (Campbell's, 15th Ed)
10. Management of Recurrence
- Recurrence rate: 10-30% after initial Ponseti treatment
- First-line: Repeat manipulation and casting (+ repeat Achilles tenotomy if needed)
- Tibialis anterior tendon transfer (TATT): indicated at age 3-8 years for persistent dynamic supination (swing-phase inversion) with flexible plantigrade foot
- Rigid recurrence: à la carte surgical release (posteromedial release via Turco or Cincinnati incision)
- Subsequent rigidity after failed release: talectomy, fusion, osteotomy, Ilizarov frame, guided growth
11. Special Situations
| Condition | Role of Ponseti |
|---|---|
| Neurogenic clubfoot (spina bifida, arthrogryposis) | Ponseti can be used; higher recurrence rates; recent SR (PMID 41272751) confirms effectiveness |
| Myelodysplastic clubfoot | Systematic review (PMID 39365806) supports Ponseti method |
| Older children | Ponseti still applicable; success rates lower, more casts needed |
| Congenital Vertical Talus | Reverse-Ponseti casting + percutaneous Achilles tenotomy + talonavicular capsulotomy |
| Recurrent after initial Ponseti | Repeat casting ± tenotomy ± TATT |
12. Key Points Summary
| Fact | Detail |
|---|---|
| Incidence | 1:1000 live births |
| Bilateral | 50% |
| Mnemonic | CAVE (Cavus, Adductus, Varus, Equinus) |
| Order of correction | C → A → V → E |
| Average casts | 5-6 |
| Tenotomy rate | ~80% of cases |
| Final cast position | 70° abduction, 15° dorsiflexion, 3 weeks |
| Success rate | ~95% (avoiding formal surgical release) |
| Brace: 1st 3 months | 23 h/day |
| Brace: up to 3-4 yrs | Sleep only |
| Recurrence rate | 10-30% |
| Key to preventing recurrence | Brace compliance |
| Recurrent dynamic supination | TATT at 3-8 years |
| Vascular association | Absent/diminutive anterior tibial artery |
Sources:
- Campbell's Operative Orthopaedics, 15th Ed 2026, Chapter 31 (Ponseti Technique 31.10, pp. 1305-1310)
- Miller's Review of Orthopaedics, 9th Ed, Section 5 - Foot
- Schwartz's Principles of Surgery, 11th Ed, Chapter 43
- Bailey & Love's Short Practice of Surgery, 28th Ed, Chapter 44 (Summary Box 44.13)
- Recent meta-analysis: Accelerated vs standard Ponseti (2026, PMID 41549019) - confirms equivalent efficacy and safety of accelerated casting schedules
PONSETTI casting
Finding Sources
Finding Sources
Reading File
Searching PubMed
Ponseti casting clubfoot technique outcome
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have everything needed for a highly detailed, image-rich answer on the Ponseti casting technique.
The Ponseti Casting Technique - Complete Guide
Overview
The Ponseti method is the gold standard for treating congenital clubfoot (CTEV). It consists of two phases:
- Treatment Phase - serial manipulation and casting
- Maintenance Phase - foot abduction orthosis (FAO) brace
Success rate: >90% correction in children under 2 years, even after previous failed nonoperative treatment. (Campbell's Operative Orthopaedics, 15th Ed 2026)
Assessment Before Casting: Pirani Scoring System
Before starting, score severity using the Pirani score (no X-rays needed for initial assessment):
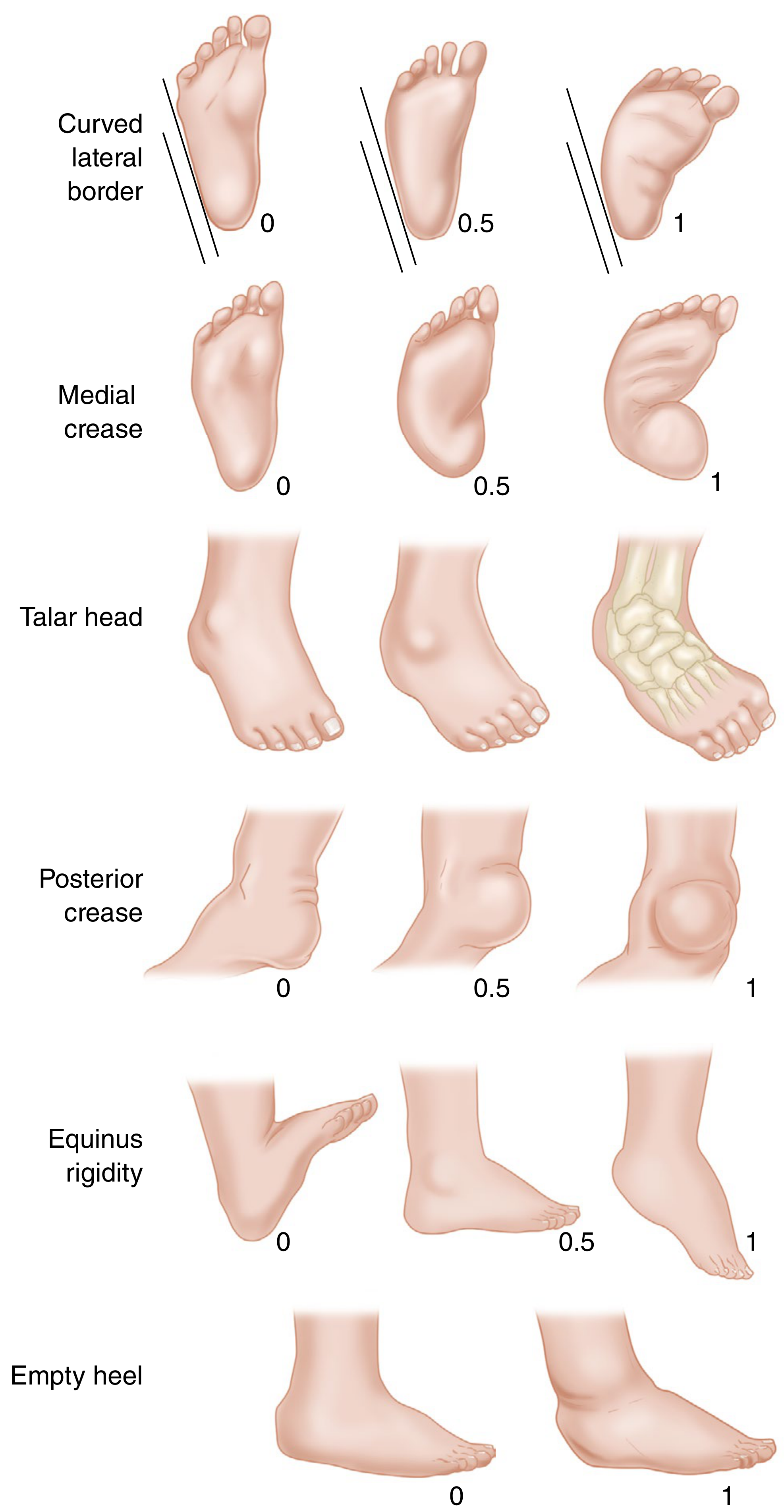
FIGURE 31.27 - Pirani classification. (Campbell's Operative Orthopaedics, 15th Ed 2026)
| Sign | 0 (Normal) | 0.5 (Moderate) | 1 (Severe) |
|---|---|---|---|
| Curved lateral border | Straight | Deviation at metatarsals | Deviation at calcaneocuboid joint |
| Medial crease | Several fine creases | 2-3 mild creases | 1 deep crease |
| Talar head coverage | Mobile (covered) | Partially mobile | Fixed/uncovered |
| Posterior crease | Several fine creases | 2-3 mild creases | 1 deep crease |
| Rigid equinus | Dorsiflexion possible | Dorsiflexion to neutral only | Rigid equinus |
| Empty heel | Calcaneus easily palpable | Palpable but deep | Not palpable |
Total score: 0-6 (higher = more severe). Midfoot score (first 3) + Hindfoot score (last 3).
The Diméglio system scores 4 parameters by goniometer reducibility (each 0-4 points) + 4 bonus points for posterior crease, medial crease, rigid cavus, poor muscle condition. Max = 20.
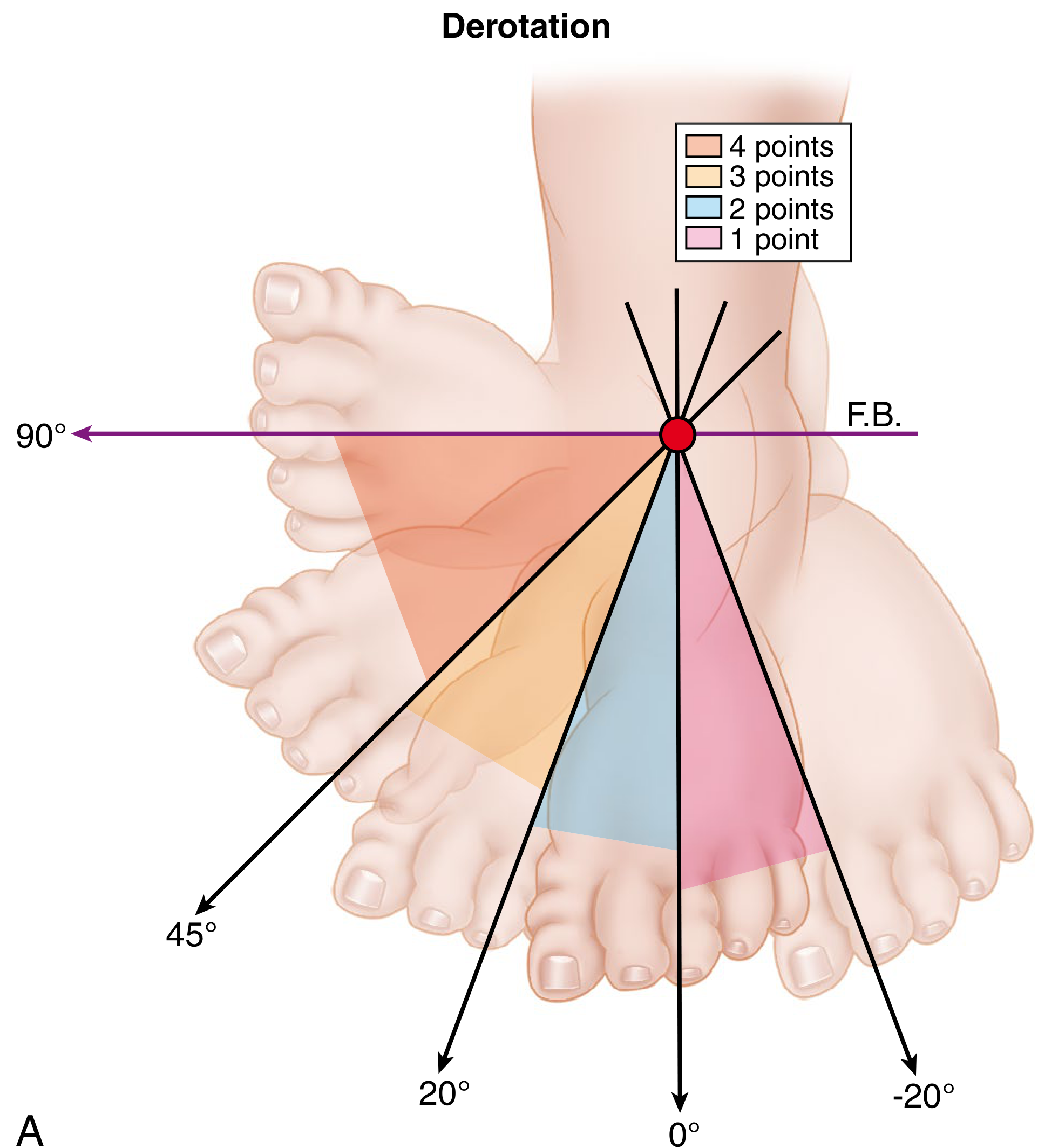
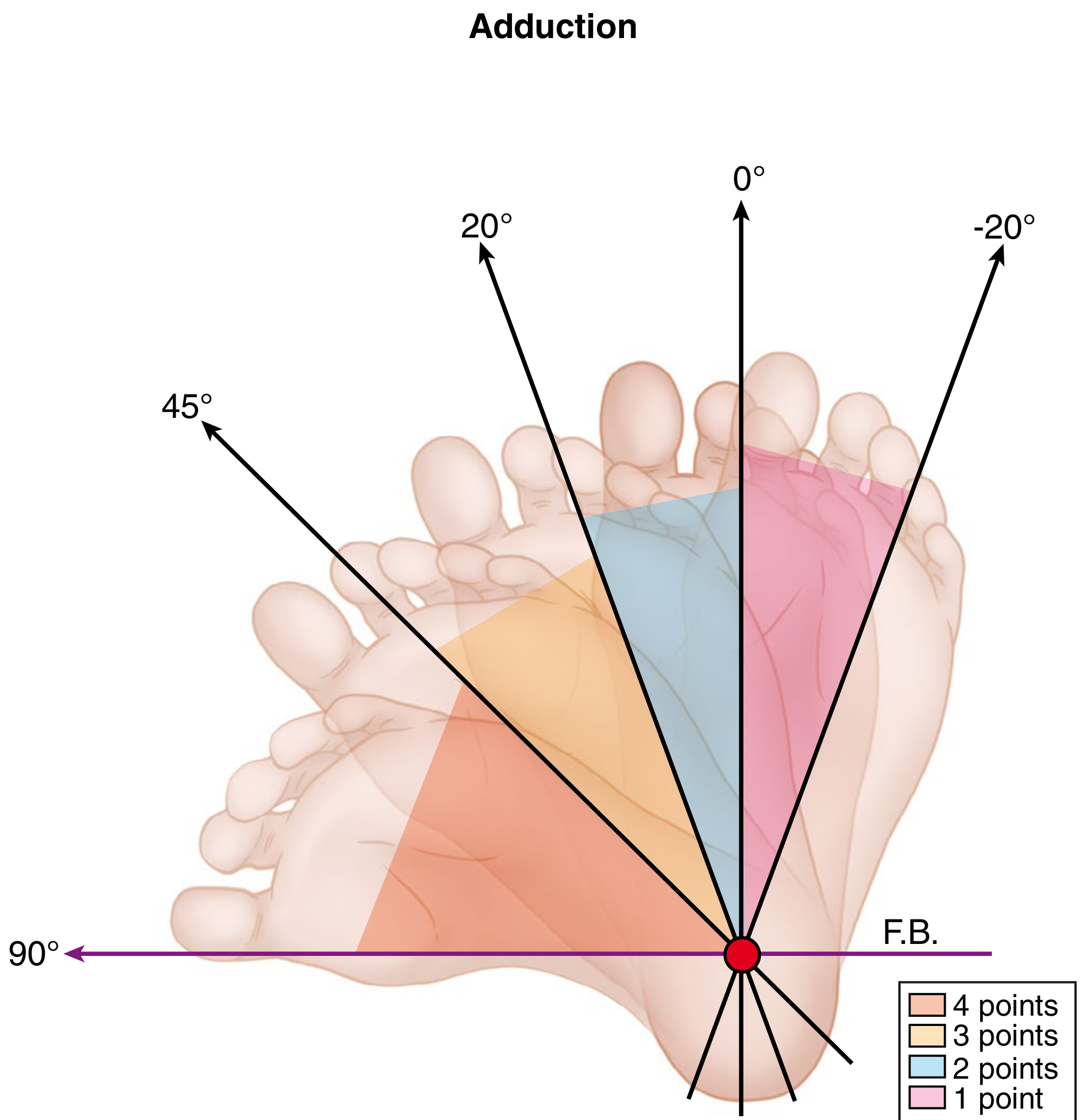
FIGURE 31.28 - Diméglio classification parameters measured by goniometer. (Campbell's, 15th Ed 2026)
PHASE 1: TREATMENT PHASE (Technique 31.10)
When to Start
- Ideally within the first 4 weeks of life
- Older children can also be treated but results are less reliable
- Casts changed weekly (accelerated biweekly schedules are also acceptable)
Order of Correction: C → A → V → E
Equinus MUST be corrected last. Attempting to dorsiflex before correcting varus causes a rocker-bottom deformity.
Step 1 - Setting
Create a warm, quiet, dimly lit room. Soothe the infant with a bottle, pacifier with sucrose solution, or soft music. A caregiver should help keep the child comfortable throughout.
Step 2 - First Cast: Correct Cavus
What is corrected: Forefoot cavus (high arch, plantarflexed first ray)
How:
- Supinate the forefoot to bring it in line with the heel
- Elevate (dorsiflex) the first metatarsal
- Align the forefoot with the hindfoot - do NOT pronate the foot
- Apply cast in two stages: short leg first (below the knee), then extend above the knee once plaster sets
Long leg (above-knee) casts are essential - they maintain the external rotation force on the foot beneath the talus, allow adequate stretching of medial structures, and prevent cast slippage.
Step 3 - First Cast Change (Week 1)
- Remove the first cast
- Perform ~1 minute of gentle manipulation
- Apply the next toe-to-groin (above-knee) cast
Step 4 - Key Manipulation Principle: Abduction Around the Talar Head
This is the central manoeuvre of the entire Ponseti technique:
- Place your thumb on the lateral head of the talus as a fulcrum
- Abduct the foot around the talar head - the navicular is felt reducing over the talar head
- Forefoot derotation must occur about the talus, NOT the calcaneocuboid joint
- NEVER directly manipulate the heel
- Maintain forefoot supination throughout - never actively pronate
- Gradually decrease the amount of supination over successive casts until the forefoot is in neutral
Correctly correcting the talonavicular subluxation (without rocker-bottom) causes the calcaneus to automatically abduct and evert - do not force the heel separately.
Step 5 - Subsequent Casts (Weeks 2-4): Progressive Abduction

Serial casts documenting stepwise correction - uncorrected foot (right) progressively correcting to fully corrected (left). (Bailey & Love's Surgery, 28th Ed)
- Continue weekly manipulation and casting for 2-3 more weeks
- Each cast abducts the foot progressively further around the talar head
- Gradually decrease supination toward neutral
- Cast is removed just before each manipulation and recasting session
Bilateral casts in progress:

Bilateral above-knee Ponseti casts. (Campbell's, 15th Ed 2026)
Step 6 - Percutaneous Achilles Tenotomy (in ~80% of cases)
When the foot cannot achieve 15° of dorsiflexion with maximal abduction, the residual equinus requires tenotomy:
| Feature | Detail |
|---|---|
| Indication | Residual equinus preventing 15° dorsiflexion |
| Rate | ~80% of cases |
| Setting | Clinic (local anaesthesia) or OR (sedation/GA) |
| Technique | Small open incision medial to tendon; cut medial to lateral |
| Blade | Beaver eye blade (rounded - reduces vascular risk) |
| Risk | Peroneal artery injury, lesser saphenous vein injury |
| Tendon fate | Regenerates within the 3-week final cast |
NOTE: "Bleeding complications have been reported after percutaneous tenotomy from injury to the peroneal artery or the lesser saphenous vein. Make a small open incision directly over the tendon before severing it, making the tenotomy from medial to lateral." - Campbell's, 15th Ed 2026
Step 7 - Final Cast
Applied immediately after tenotomy:
| Parameter | Value |
|---|---|
| Abduction | ~70 degrees |
| Dorsiflexion | 15 degrees |
| Duration | 3 weeks |
| Type | Above-knee long leg cast |
| Casts total | Usually 5-6 in whole course |
The foot is held in this overcorrected position while the Achilles tendon regenerates.
Technique of Ponseti casting - cast progression diagram
FIGURE 31.30 description (Campbell's): A = First cast: forefoot aligned with heel, outer edge still tilted downward (Achilles tightness). B = Second cast: outer edge still down, forefoot moved slightly outward. C = Third cast: Achilles stretched, outer edge moving toward normal, forefoot turned further outward. D = Final cast: Achilles fully stretched, foot pointed upward at 70°/15°.
PHASE 2: MAINTENANCE PHASE (Foot Abduction Orthosis)
After the final cast is removed:
| Period | Protocol |
|---|---|
| First 3 months | FAO worn 23 hours/day |
| Age ~3-4 years | FAO worn during sleep only |
| Beyond 4 years | Discontinue (extending to 4 years superior to stopping at 3) |
FAO specifications:
- Shoes on a bar at 70° external rotation and 15° dorsiflexion
- Bar width = ~1 inch wider than infant's shoulder width
- Bilateral bracing is superior to unilateral
- Compliance is the #1 factor preventing recurrence
Key "Do's and Don'ts" (Campbell's Concepts)
| ✅ DO | ❌ DON'T |
|---|---|
| Apply long leg (above-knee) casts | Use short leg casts only |
| Supinate forefoot throughout process | Pronate the foot at any stage |
| Abduct around the head of the talus | Directly manipulate the heel |
| Correct C → A → V → E in order | Try to dorsiflex early (causes rocker-bottom) |
| Use rounded Beaver blade for tenotomy | Make a blind stab tenotomy |
| Remove cast just before re-manipulation | Leave cast on for more than 1 week (usually) |
| Encourage strict brace compliance | Discontinue brace early |
Modifications Proven Equivalent
| Modification | Evidence |
|---|---|
| Accelerated (biweekly) casting | Same outcomes, faster correction; confirmed by 2026 meta-analysis (PMID 41549019) |
| Fiberglass casts | Similar results to plaster of Paris; confirmed by 2026 SR (PMID 40888800) |
| Bracing to 4 years | Superior to stopping at 3 years |
| Various providers (nurses, PTs, cast technicians) | Equivalent results to surgeon-only casting |
Recurrence and What to Do
- Recurrence rate: 10-30%
- Most recurrences: equinus + heel varus (early, mild)
- First line: repeat manipulation and casting
- Repeat Achilles tenotomy if dorsiflexion insufficient
- TATT (tibialis anterior tendon transfer): for persistent dynamic supination (swing-phase inversion) in a flexible foot; performed between ages 3-8 years
- Rigid recurrence: à la carte posteromedial surgical release (Turco/Cincinnati incision)
- Rate of surgical procedures beyond tenotomy: ~35% in recent studies
Sources:
- Campbell's Operative Orthopaedics, 15th Ed 2026, Technique 31.10 (pp. 1307-1310)
- Bailey & Love's Short Practice of Surgery, 28th Ed, Chapter 44 (Summary Box 44.13)
- Miller's Review of Orthopaedics, 9th Ed, Section 5
- Network meta-analysis of RCTs - optimal clubfoot treatment (PMID 38015923) - confirms Ponseti as first-line
- Accelerated vs standard Ponseti 2026 SR/MA (PMID 41549019) - biweekly casting is safe and effective
Intra articular injection for osteoarthritis
Finding Sources
Finding Sources
Searching PubMed
intraarticular injection osteoarthritis
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading Article
PMID: 38037038
Reading Article
PMID: 39751394
Excellent - I now have comprehensive content from all sources. Here is the full answer:
Intra-articular Injections for Osteoarthritis
Overview
Intra-articular (IA) injections are a key component of the non-operative management ladder for osteoarthritis (OA), used when oral analgesics, physiotherapy, and lifestyle modification provide insufficient relief, and before surgical options are considered. The main injectable agents are:
- Corticosteroids (CSC)
- Hyaluronic acid / viscosupplementation (HA)
- Platelet-rich plasma (PRP)
- Bone marrow aspirate concentrate (BMAC)
1. Corticosteroid Injections
Mechanism
- Suppress synovial inflammation by inhibiting phospholipase A2, reducing prostaglandins, leukotrienes, and cytokines
- Combined with a local anaesthetic (e.g., lidocaine) for immediate diagnostic and therapeutic effect
- Diagnostic value: Immediate pain relief after injection localises the source of pain to the joint (useful in distinguishing hip OA from lumbar spine pathology)
Common Agents Used
| Agent | Type | Duration of action |
|---|---|---|
| Methylprednisolone acetate | Depot ester | 4-6 weeks |
| Triamcinolone acetonide | Depot ester | 4-8 weeks |
| Betamethasone | Soluble + depot | Variable |
| Dexamethasone | Soluble | Short-acting |
Efficacy
- Hip OA: Transient (~1 month) pain relief in up to 90% of patients with mild arthritis; only 9-20% benefit with severe arthritis (Campbell's, 15th Ed 2026)
- Knee OA: Short-term pain relief and improved function; well-established for acute flares
- Shoulder, small joints (CMC thumb, etc.): Benefit supported by evidence
Frequency / Limits
- Generally no more than 3-4 injections per year per joint
- Repeated corticosteroid injections destroy remaining cartilage over time and should be avoided in posttraumatic arthritis (Rockwood & Green, 10th Ed 2025)
- Recent MRI studies have raised concerns about accelerated cartilage loss, subchondral insufficiency fractures, and osteonecrosis with repeated use
Complications
| Complication | Notes |
|---|---|
| Infection (septic arthritis) | ~1 in 1,000,000 injections; risk ↑ with immunosuppression |
| Post-injection flare | Transient worsening of pain 12-24h after injection |
| Cartilage damage | From the needle or from repeated steroid exposure |
| Tendon rupture | If injected into or near a tendon |
| Hyperglycaemia | Common in diabetics; short-term glucose elevation; warn patients |
| Skin depigmentation / fat atrophy | At injection site |
| Hypothalamic-pituitary-adrenal (HPA) axis suppression | After intraarticular methylprednisolone (documented by Mader et al.) |
| Anaphylaxis | Rare; reported with methylprednisolone acetate |
| Haemarthrosis | From needle trauma |
Contraindications
- Active local or systemic infection
- Prosthetic joint (relative - specialist injection only)
- Overlying skin infection or psoriasis at injection site
- Uncontrolled coagulopathy
- Known hypersensitivity to steroid preparation
2. Viscosupplementation (Hyaluronic Acid - HA)
Rationale
- In OA, synovial fluid loses its normal viscoelastic properties (reduced molecular weight and concentration of hyaluronan)
- Exogenous HA aims to restore lubrication and shock absorption
- Mechanism not fully understood; may also have anti-inflammatory and analgesic effects beyond viscosity alone
Products
- Multiple preparations available: single-injection (e.g., Synvisc-One), 3-injection (e.g., Supartz), or 5-injection courses
- Molecular weight varies (low vs high MW products)
Efficacy by Joint - Guideline Positions
| Joint | Recommendation |
|---|---|
| Knee | Frequently used; efficacy questioned by AAOS guidelines; some benefit in mild-moderate OA; still widely offered (Schwartz's Principles of Surgery, 11th Ed) |
| Hip | Strongly recommended AGAINST by ACR/Arthritis Foundation guidelines (Campbell's, 15th Ed 2026) |
| Shoulder, ankle | Limited/inconclusive evidence |
| Haemophilic arthropathy (knee) | HA used in milder disease before progressing to TKA (Campbell's) |
"The efficacy of hyaluronic acid injections has been questioned by recent evidence summarised in the American Academy of Orthopaedic Surgeons' Clinical Practice Guidelines." - Schwartz's Principles of Surgery, 11th Ed
Complications
- Joint infection
- Cartilage injury from the needle
- Haemarthrosis
- Post-injection pain flare ("pseudoseptic" reaction - more common with some products)
- Failure to benefit
3. Platelet-Rich Plasma (PRP)
Rationale
- Autologous blood is centrifuged to concentrate platelets (containing growth factors: PDGF, TGF-β, VEGF, IGF-1, EGF)
- Aims to stimulate tissue repair, modulate inflammation, and potentially promote chondroprotection
Preparation
- Venous blood drawn, centrifuged, platelet-rich layer isolated
- Platelet concentration matters: high-platelet PRP (≥1,000,000 platelets/μL) is more effective than low-platelet PRP
Efficacy - Best Current Evidence
A 2023 network meta-analysis of 35 RCTs (3104 patients) found: (PMID 38037038)
| Timepoint | Best WOMAC (function) | Best VAS (pain) |
|---|---|---|
| 3 months | PRP > PRP+HA > HA > placebo > CSC | PRP+HA > PRP > CSC > HA > placebo |
| 6 months | PRP = CSC = HA = placebo | PRP+HA best |
| 12 months | PRP > PRP+HA > HA > placebo > CSC | PRP best |
PRP and PRP+HA were the most successful in improving function and alleviating pain at 3, 6, and 12 months. No therapy increased treatment-related adverse events compared to placebo.
A 2025 meta-analysis of 18 RCTs (1995 patients) confirmed: (PMID 39751394)
- PRP exceeds the Minimal Clinically Important Difference (MCID) for functional improvement (WOMAC) at all timepoints and for pain (VAS) at 3-6 months
- High-platelet PRP provides superior and more durable pain relief vs low-platelet PRP; the benefit for pain is maintained to 12 months with high-platelet, but not low-platelet PRP
Key Points on PRP
- Considered safe; no increase in adverse events vs placebo
- Results depend on platelet concentration - standardisation of preparation is important
- More durable benefit than corticosteroids, but onset may be slower
- Not universally covered by insurance/NHS; evidence still evolving
4. Bone Marrow Aspirate Concentrate (BMAC)
- Contains mesenchymal stem cells, growth factors, and anti-inflammatory cytokines
- Used in posttraumatic arthritis and early OA as a biological bridge before arthroplasty
- May "carry the patient for a period of time" when viscosupplementation or PRP has been tried (Rockwood & Green, 10th Ed 2025)
- Less evidence than PRP; currently considered investigational in most guidelines
Comparative Summary
| Feature | Corticosteroid | Hyaluronic Acid | PRP | BMAC |
|---|---|---|---|---|
| Onset of effect | Rapid (days) | Slow (weeks) | Slow (weeks) | Slow (weeks) |
| Duration of effect | Short (~1-3 months) | Moderate (3-6 months) | Longer (6-12 months) | Variable |
| Best evidence | Strong (short-term) | Moderate (knee only) | Growing (strongest for knee) | Limited |
| Cost | Low | Moderate | Higher | Highest |
| Repeat injections | Limited (cartilage risk) | Can repeat courses | Can repeat | Limited data |
| Guideline support | Yes (all joints, short-term) | Knee only; not hip (ACR) | Increasingly supported | Investigational |
| Cartilage concern | Yes (repeated use) | No | No | No |
| Hyperglycaemia risk | Yes | No | No | No |
Practical Considerations
- Ultrasound guidance improves accuracy of injection and reduces pain, especially for hip and shoulder joints; superior to palpation-guided for some joints (Rheumatology, Elsevier 2022)
- Pre-arthroplasty injections: Intraarticular steroid injection within 3 months of arthroplasty may increase infection risk - counsel patients accordingly
- Diabetic patients: Warn about transient blood glucose elevation lasting 24-72 hours after corticosteroid injection
- Frequency: No more than 3-4 corticosteroid injections per joint per year; repeated steroid injections are cartilage-destructive and should be discouraged in young patients with remaining cartilage
Sources:
- Campbell's Operative Orthopaedics, 15th Ed 2026, Chapter 7 (Hip Osteoarthritis)
- Schwartz's Principles of Surgery, 11th Ed, Chapter 43 (Joint Injections)
- Rockwood & Green's Fractures in Adults, 10th Ed 2025, Chapter 64 (Posttraumatic Arthritis)
- Rheumatology, 2-Volume Set (Elsevier, 2022), Chapter references for IA injections
- Network MA: CSC vs HA vs PRP for knee OA - Qiao et al. 2023 (PMID 38037038) - PRP + PRP+HA best at 3, 6, 12 months
- Meta-analysis PRP for knee OA - Bensa et al. 2025 (PMID 39751394) - high-platelet PRP clinically significant benefit to 12 months
This is a shared conversation. Sign in to Orris to start your own chat.