Ecg reading for common arrhythmia s
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Now I have everything needed for a comprehensive, well-illustrated answer. Let me compile it.
ECG Reading for Common Arrhythmias
A structured guide to recognizing the key ECG features of the most frequently encountered arrhythmias, drawn from Tintinalli's Emergency Medicine, Harrison's Principles, and The Washington Manual of Medical Therapeutics.
How to Approach Any Rhythm Strip
Before identifying an arrhythmia, work through this sequence on every ECG:
- Rate - count R-R intervals (300 / number of large squares between R waves)
- Rhythm - regular, regularly irregular, or irregularly irregular?
- P waves - present? morphology? one before each QRS?
- PR interval - normal is 120-200 ms (3-5 small squares)
- QRS duration - normal is <120 ms (3 small squares); wide = >120 ms
- QT interval - corrected QTc normal <440 ms (men), <460 ms (women)
1. Sinus Tachycardia
| Feature | Finding |
|---|---|
| Rate | 100-180 bpm |
| P waves | Present, upright in I and II, one before each QRS |
| PR interval | Normal (120-200 ms) |
| QRS | Narrow (<120 ms), normal morphology |
| Rhythm | Regular |
Key point: Always look for a cause (pain, fever, hypovolemia, PE, thyrotoxicosis). It is a response, not a primary arrhythmia.
2. Atrial Fibrillation (AF)
ECG features (Tintinalli's Emergency Medicine):
- Absence of discernible P waves - flat or chaotic isoelectric baseline
- Irregularly irregular ventricular rhythm (the classic hallmark)
- QRS complexes narrow unless pre-existing bundle branch block or pre-excitation syndrome
- Ventricular rate typically 100-180 bpm if uncontrolled
Causes: Ischemic/valvular heart disease, cardiomyopathy, thyrotoxicosis, alcohol ("holiday heart"), myocarditis, blunt chest trauma.
Types:
- Paroxysmal: terminates spontaneously within 7 days
- Persistent: sustained >7 days or requires treatment to terminate
- Long-standing persistent: continuous >1 year
- Permanent: decision made not to restore sinus rhythm
3. Atrial Flutter
ECG features (Tintinalli's Emergency Medicine):
| Feature | Finding |
|---|---|
| P waves | "Flutter waves" - single morphology, negative amplitude ("sawtooth pattern") best seen in inferior leads (II, III, aVF) and V1 |
| Atrial rate | Regular, ~300 bpm (range 250-350 bpm) |
| Ventricular rate | Often 150 bpm due to 2:1 AV nodal block (classic clue) |
| QRS | Narrow unless pre-existing bundle branch block |
| Rhythm | Ventricular rate regular; occasional irregularity possible |
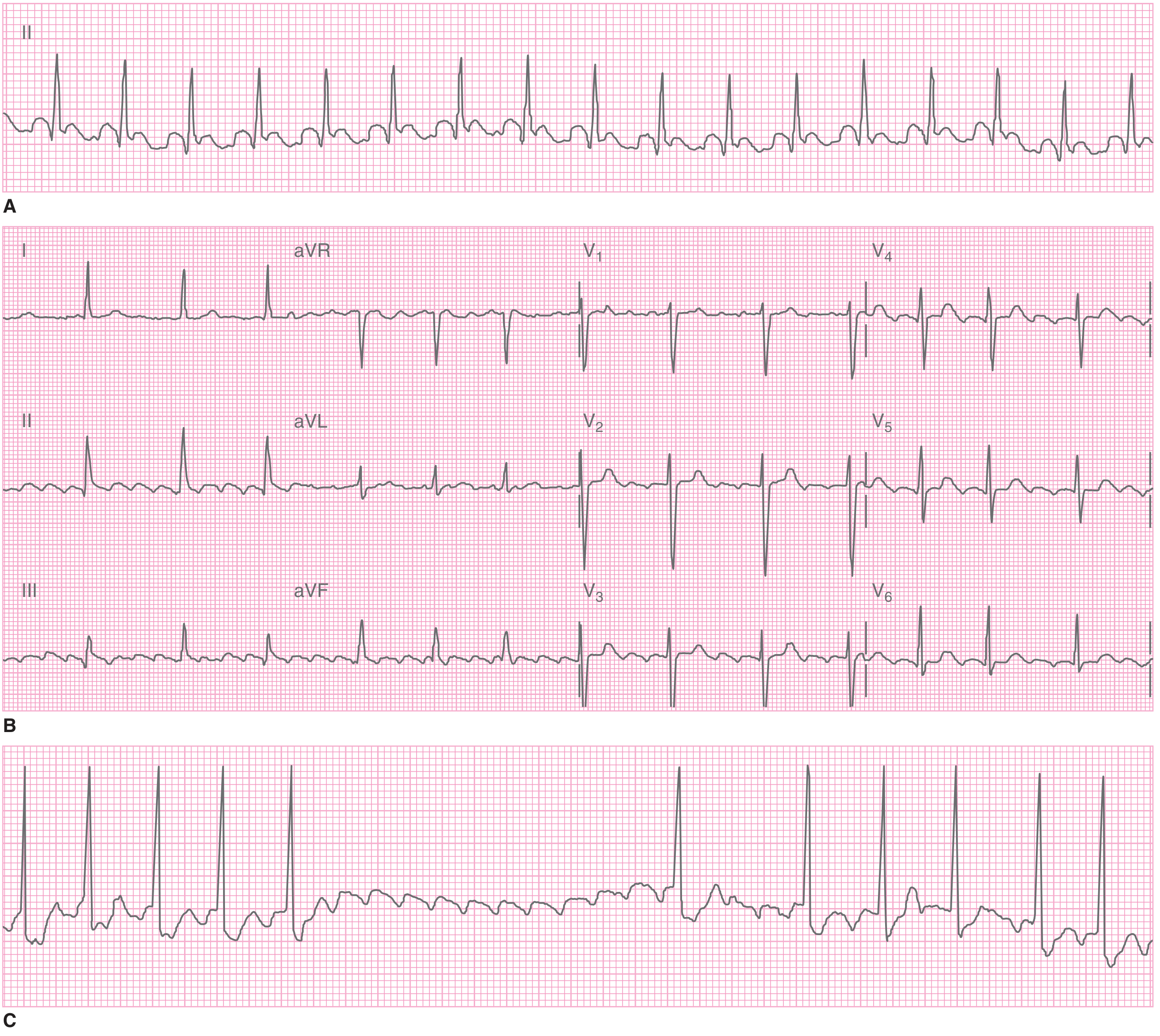
Atrial flutter. A: Regular narrow-complex tachycardia at 155 bpm. B: Flutter waves visible in inferior leads and V1. C: Carotid sinus massage inducing transient AV block and unmasking flutter waves. (Tintinalli's Emergency Medicine)
Tip: A narrow-complex tachycardia at exactly 150 bpm should make you think of atrial flutter with 2:1 block until proven otherwise.
4. Supraventricular Tachycardia (SVT)
Generic ECG features:
- Rate: 150-250 bpm
- P waves: often buried in or just after the QRS, may be retrograde (negative in II, III, aVF)
- QRS: narrow (<120 ms) unless aberrant conduction
- Rhythm: regular
Types include:
- AVNRT (AV nodal re-entry tachycardia): most common; P waves hidden in or pseudo-R' at end of QRS
- AVRT (accessory pathway): includes WPW; delta wave visible in sinus rhythm
- Atrial tachycardia: distinct P wave morphology different from sinus P
Vagal maneuvers (carotid sinus massage, Valsalva): may terminate AVNRT/AVRT or transiently slow rate to reveal flutter waves
5. Ventricular Tachycardia (VT)
ECG features:
- Rate: 100-250 bpm
- Wide QRS (>120 ms) - this is the defining feature
- AV dissociation - P waves march through independently of QRS (pathognomonic for VT)
- Fusion beats and capture beats - prove AV dissociation
- Monomorphic: all QRS complexes have same morphology
- Polymorphic: QRS morphology varies (includes Torsades de Pointes)
Distinguishing VT from SVT with aberrancy (Harrison's Principles, 22nd Ed.):
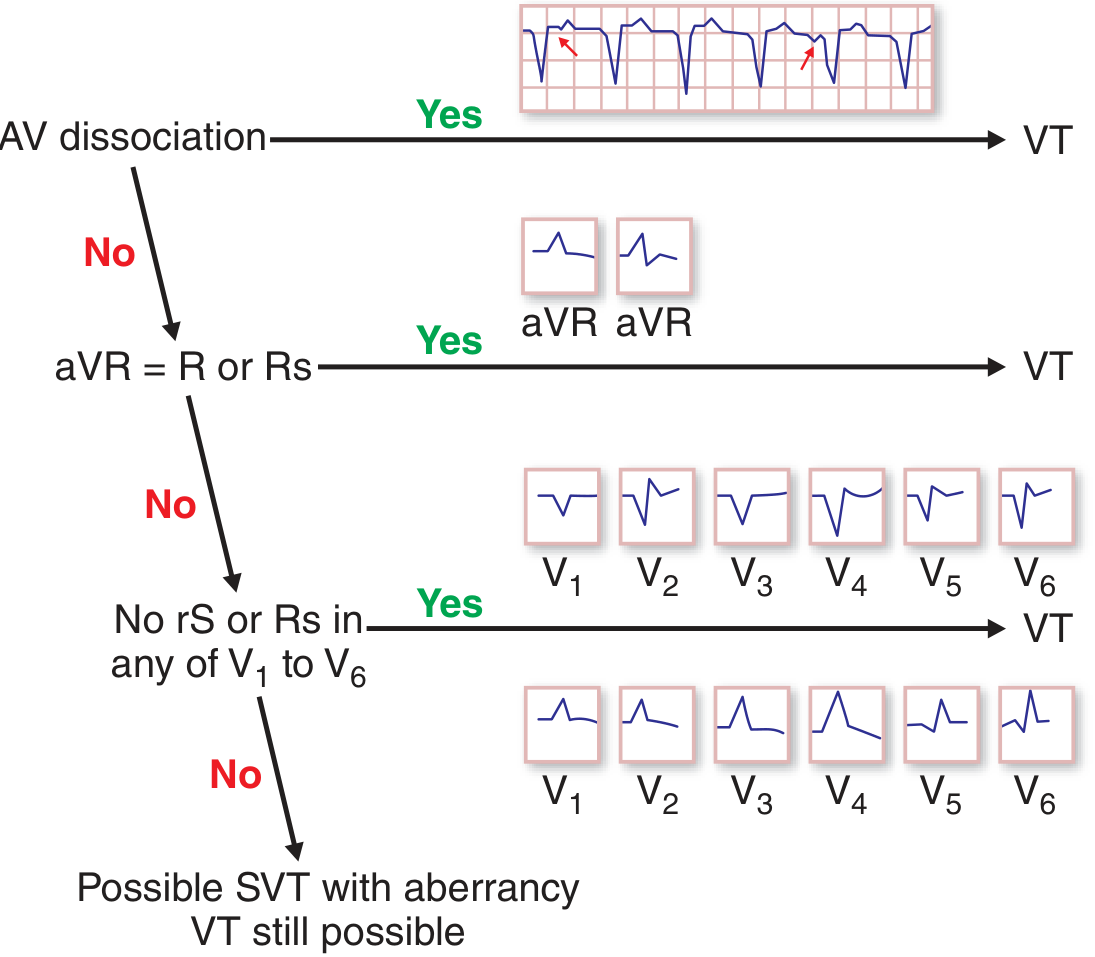
Algorithm: Step 1 - AV dissociation? → VT. Step 2 - monophasic R or Rs in aVR? → VT. Step 3 - concordance (all positive or all negative) V1-V6? → VT. (Harrison's 22nd Ed.)
Additional VT clues:
- In known heart disease, any wide-complex tachycardia is VT until proven otherwise
- Hemodynamic stability does NOT exclude VT
- Same QRS morphology as known bundle branch block in sinus rhythm suggests SVT with aberrancy
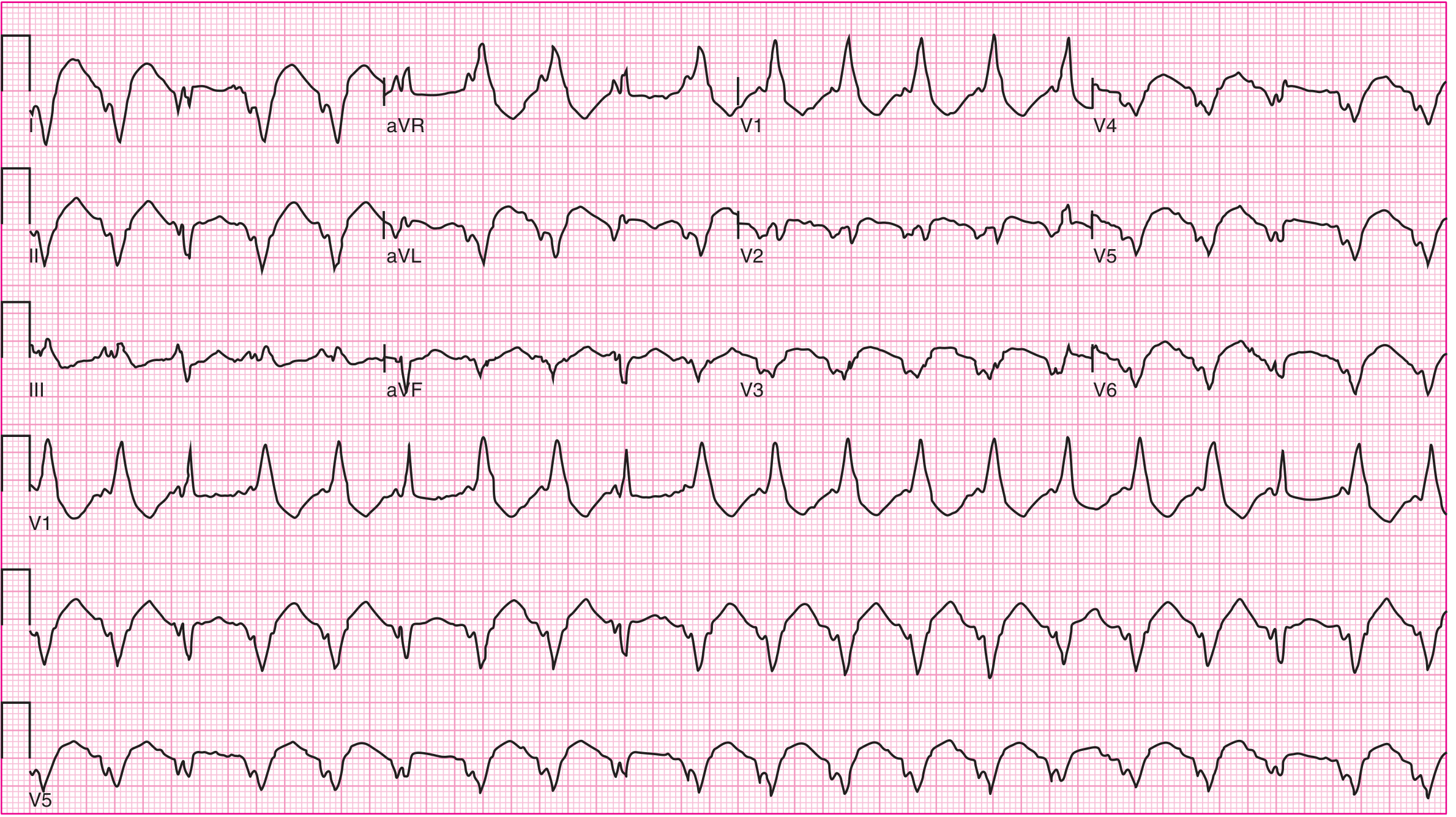
Monomorphic VT in a patient with prior MI. Complexes 3, 9, and 18 are narrower fusion beats, proving AV dissociation. (Harrison's Principles 22nd Ed.)
6. Ventricular Fibrillation (VF)
ECG features:
- Chaotic, irregular undulations of varying amplitude and frequency
- No identifiable QRS complexes, P waves, or T waves
- Coarse VF: larger amplitude deflections; fine VF: low-amplitude undulations (can mimic asystole)
- No organized cardiac output - immediate defibrillation required
7. AV Conduction Blocks
First-Degree AV Block
- PR interval >200 ms (>5 small squares) on every beat
- All P waves conduct - no dropped beats
- QRS narrow and normal
- Usually benign
Second-Degree AV Block
Mobitz Type I (Wenckebach) (Washington Manual):
- Progressive PR prolongation with each successive beat
- Shortening of each subsequent RR interval before dropped beat
- A "grouped beating" pattern (regularly irregular)
- The blocked beat has no QRS after the P wave
- Usually at the AV node level; relatively benign; rarely progresses to complete block
Mobitz Type II:
- PR intervals are constant (no lengthening before the dropped beat)
- Abrupt, unexpected dropped QRS
- Often has bundle branch block
- More sinister - can progress suddenly to complete heart block
- Requires pacemaker consideration
2:1 AV Block:
- Every other P wave is not conducted
- Cannot be classified as Wenckebach vs. Mobitz II from a single strip
- Clues: if PR is prolonged and no BBB → more likely Wenckebach; if QRS is wide or BBB present → more likely Mobitz II
Third-Degree (Complete) AV Block
- Complete AV dissociation - atria and ventricles beat independently
- P-P intervals regular; R-R intervals regular; but no fixed PR relationship
- Atrial rate > ventricular rate
- Ventricular rate determined by escape rhythm:
- Junctional escape: 40-60 bpm, narrow QRS
- Ventricular escape: 20-40 bpm, wide QRS (worse prognosis)
8. Torsades de Pointes (TdP)
ECG features:
- Polymorphic VT where QRS axis appears to "twist" around the isoelectric line
- QRS complexes change in amplitude and polarity cyclically
- Preceded by prolonged QTc on baseline ECG
- Often initiated by a "short-long-short" RR sequence
- Rate: 200-250 bpm
Common causes of long QT: Hypomagnesemia, hypokalemia, class Ia/III antiarrhythmics (quinidine, sotalol, amiodarone), antipsychotics, macrolides.
Treatment: IV magnesium sulfate 2g, correct electrolytes, remove offending drug.
Quick Reference Summary Table
| Arrhythmia | Rate (bpm) | P waves | PR interval | QRS | Rhythm |
|---|---|---|---|---|---|
| Sinus tachycardia | 100-180 | Normal, 1:1 | Normal | Narrow | Regular |
| Atrial fibrillation | Variable | Absent/chaotic | None | Narrow* | Irreg. irreg. |
| Atrial flutter | ~300 atrial, ~150 ventricular | Sawtooth | Variable | Narrow* | Regular |
| SVT (AVNRT) | 150-250 | Buried/retrograde | Short/none | Narrow | Regular |
| VT (monomorphic) | 100-250 | Dissociated | None | Wide | Regular |
| VF | N/A | None | None | Chaotic | Chaotic |
| 1° AV block | Normal | Normal | >200 ms | Narrow | Regular |
| Wenckebach | Normal | Normal | Progressive ↑ | Narrow | Group beats |
| Mobitz II | Normal | Normal | Constant | Narrow/Wide | Regular + drops |
| 3° AV block | Slow (20-60) | Dissociated | None | Narrow/Wide | Regular (escape) |
| Torsades | 200-250 | None visible | Prolonged QT | Twisting wide | Irregular |
Unless pre-existing bundle branch block or pre-excitation
Sources:
- Tintinalli's Emergency Medicine, Table 18-8 and 18-9
- Harrison's Principles of Internal Medicine, 22nd Edition, Ch. 261
- The Washington Manual of Medical Therapeutics, Ch. 7
This is a shared conversation. Sign in to Orris to start your own chat.