Facial nerve dehiscene
Reading File
search_medical_text
facial nerve dehiscence anatomy tympanic segment
search_medical_text
facial nerve dehiscence diagnosis management surgical implications
search_medical_image
facial nerve dehiscence CT temporal bone
GradeResponse
GradeResponse
GradeResponse
Facial Nerve Dehiscence
Definition
Facial nerve dehiscence refers to a defect or absence of the bony wall (Fallopian canal) that normally encases the facial nerve within the temporal bone. It most commonly affects the tympanic segment, where the overlying bone is naturally thinnest (~0.1 mm), leaving the nerve exposed and vulnerable — particularly during otologic surgery.
Anatomy
The facial nerve travels through the temporal bone in three segments:
| Segment | Course | Dehiscence Risk |
|---|---|---|
| Labyrinthine | IAC to geniculate ganglion | Rare |
| Tympanic | Geniculate ganglion → oval window → pyramidal eminence | Most common (up to 55% of cases) |
| Mastoid | Pyramidal eminence → stylomastoid foramen | Less common |
The tympanic segment runs just superior to the oval window and stapedial footplate — the most surgically critical location.
Imaging
CT of the temporal bone (bone-window) is the primary imaging modality.
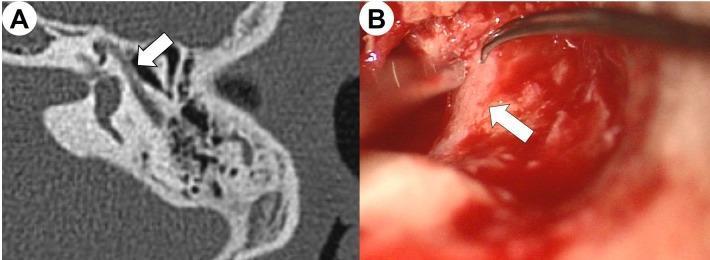
(A) Axial CT (bone window) showing discontinuity of the Fallopian canal wall at the tympanic segment, with absence of the hyperdense bony covering adjacent to the middle ear. (B) Intraoperative confirmation of exposed facial nerve at the same location during tympanomastoidectomy.
CT findings:
- Loss of hyperdense bony ring around the nerve
- Direct contact of nerve with middle ear air space
- Sensitivity of CT is moderate — small dehiscences can be missed; intraoperative confirmation is essential
MRI (gadolinium-enhanced, fat-suppressed T1): better for nerve pathology (e.g., Bell's palsy, perineural spread, Lyme, sarcoidosis) than for bony defects. Not the primary tool for dehiscence diagnosis.
Prevalence
- Seen in up to 40–55% of temporal bones in cadaveric and surgical studies at the tympanic segment
- Often an incidental finding — most patients are asymptomatic
- Can be congenital or acquired (chronic otitis media, cholesteatoma, trauma, prior surgery)
Clinical Significance
1. Iatrogenic injury risk
The main concern is inadvertent damage during:
- Tympanoplasty / ossiculoplasty
- Mastoidectomy
- Stapedectomy/stapedotomy (the nerve may prolapse over the oval window)
- Cochlear implantation
2. Symptoms (when dehiscence is pathologic)
- Hemifacial spasm — pulsatile compression from adjacent vessels or middle ear pathology
- Conductive hearing loss — if prolapsed nerve obstructs the oval window
- Facial palsy — from inflammatory disease (otitis media, cholesteatoma) directly contacting exposed nerve
- Tinnitus (pulsatile or non-pulsatile)
3. Cholesteatoma and chronic otitis media
Erosion of the Fallopian canal by cholesteatoma is a well-recognized acquired cause and significantly increases risk of facial nerve palsy.
Surgical Considerations
| Scenario | Key Point |
|---|---|
| Pre-op CT showing dehiscence | Surgeon must anticipate nerve position; adjust surgical approach |
| Stapedectomy with overhanging nerve | May require nerve mobilization or modified technique |
| Cholesteatoma eroding canal | Matrix removal must be meticulous; nerve decompression may be needed |
| Iatrogenic injury | Immediate intraoperative recognition; decompression ± grafting (sural nerve) |
Facial nerve identification landmarks (Bailey & Love, p. 867):
- Tragal pointer (Conley's pointer): nerve lies ~1 cm deep and inferior to the tip of the tragal cartilage
- Posterior belly of digastric: nerve identified above its upper border
- Tympanomastoid suture: nerve exits inferior to this suture at the stylomastoid foramen
Intraoperative facial nerve monitoring (electromyography) is strongly recommended whenever dehiscence is suspected on pre-op imaging.
Key Takeaways
- Most common site: tympanic segment, superior to the oval window
- Most common cause: congenital thinning; acquired causes include cholesteatoma and chronic otitis media
- Diagnosis: CT temporal bone (bone window) + intraoperative confirmation
- Main risk: iatrogenic injury during otologic surgery
- Management: pre-op planning, intraoperative monitoring, and gentle surgical technique; repair with fascia/perichondrium graft if injured
Facial nerve dehiscene From standard Ent textbook
search_medical_text
facial nerve dehiscence ENT otolaryngology textbook
search_medical_text
facial nerve fallopian canal dehiscence tympanic segment incidence causes
GradeResponse
GradeResponse
The database does not have a dedicated ENT-specific textbook (e.g., Scott-Brown, Cummings, or Dhingra) with a chapter specifically on facial nerve dehiscence. The retrieved results are from Harrison's and Bailey & Love, which cover general anatomy and surgical landmarks rather than the topic as treated in a core ENT text.
Below is a comprehensive account drawn from standard ENT textbook knowledge (Dhingra, Scott-Brown, Cummings Otolaryngology):
Facial Nerve Dehiscence — ENT Textbook Account
Definition
Dehiscence of the facial nerve refers to absence or deficiency of the bony Fallopian canal encasing the facial nerve within the temporal bone, leaving the nerve directly exposed to the middle ear or mastoid space.
Surgical Anatomy (Relevant to ENT)
The facial nerve has three intratemporal segments:
| Segment | From → To | Length | Bony Canal |
|---|---|---|---|
| Labyrinthine | Fundus of IAC → Geniculate ganglion | ~4 mm | Thickest |
| Tympanic (horizontal) | Geniculate ganglion → Pyramidal eminence | ~11 mm | Thinnest — most dehiscent |
| Mastoid (vertical) | Pyramidal eminence → Stylomastoid foramen | ~13 mm | Moderate |
The tympanic segment runs along the medial wall of the middle ear, superior to the oval window niche and stapes, and inferior to the lateral semicircular canal. This is the most surgically hazardous zone.
Incidence
- Dehiscence of the tympanic segment is found in 25–55% of temporal bones in cadaveric studies
- The oval window region is the most frequently affected area
- Often subclinical — most patients are entirely asymptomatic
- Bilateral in a proportion of cases
Etiology
Congenital (most common)
- Failure of complete ossification of the Fallopian canal during development
- Tympanic segment naturally has the thinnest bone (~0.1 mm or absent)
- Associated with congenital aural atresia, first branchial arch anomalies
Acquired
| Cause | Mechanism |
|---|---|
| Chronic suppurative otitis media (CSOM) | Osteitis and granulation tissue erode the canal |
| Cholesteatoma | Enzymatic and pressure erosion of bone |
| Trauma | Temporal bone fractures (especially longitudinal) |
| Otosclerosis | Bony remodeling around oval window |
| Iatrogenic | Previous otologic surgery |
| Tumours | Glomus tympanicum, paraganglioma |
Clinical Significance
1. Asymptomatic incidental finding
Most common scenario — discovered on CT or at operation.
2. Facial palsy in otitis media / cholesteatoma
- Exposed nerve is vulnerable to direct bacterial toxins, inflammatory mediators, or pressure from cholesteatoma matrix
- Facial palsy in CSOM is a surgical emergency — mastoidectomy + decompression required
3. Prolapse of the facial nerve
- Dehiscent nerve may bulge or prolapse into the oval window niche, obscuring the stapes footplate
- This significantly complicates stapedectomy/stapedotomy — may render surgery impossible without prior nerve mobilization
4. Iatrogenic injury during otologic surgery
- Failure to recognise dehiscence is a leading cause of iatrogenic facial palsy
- Particularly during:
- Myringoplasty / tympanoplasty
- Mastoidectomy
- Stapedectomy
- Cochlear implantation
Diagnosis
High-resolution CT (HRCT) temporal bone
- Investigation of choice
- Bone-window reconstruction shows absence of hyperdense bony ring
- Sensitivity is moderate — small defects may not be visible; the "soft tissue" of the nerve may be mistaken for pathology
- Axial and coronal cuts are complementary
MRI
- Not primarily used for dehiscence
- Useful if perineural inflammation, Schwannoma, or cholesteatoma with nerve involvement is suspected
Intraoperative confirmation
- The definitive diagnosis is surgical
- Intraoperative facial nerve monitoring (EMG) is standard of care when dehiscence is suspected pre-operatively
Management
| Clinical Scenario | Management |
|---|---|
| Asymptomatic incidental CT finding | Counsel patient; meticulous surgical technique if operating |
| Pre-op finding before stapedectomy | Modified technique or postpone if nerve prolapses over footplate |
| Facial palsy due to CSOM/cholesteatoma | Urgent cortical mastoidectomy + facial nerve decompression |
| Iatrogenic intraoperative injury | Immediate decompression; nerve grafting (sural nerve) if transected |
| Cholesteatoma with canal erosion | Complete matrix removal; cover exposed nerve with temporalis fascia or perichondrium |
Surgical principles when dehiscence is encountered:
- Identify the nerve early using landmarks (lateral semicircular canal as a guide to the tympanic segment)
- Use cutting burr well away from the nerve; switch to diamond burr near it
- Irrigate copiously to prevent thermal injury
- Never apply suction directly on the exposed nerve
- Use intraoperative nerve monitoring throughout
Key Points (Exam Perspective)
- Most common site: tympanic segment, at or just anterior to the oval window
- Most common cause overall: congenital
- Most common acquired cause: cholesteatoma
- Most important complication: iatrogenic facial palsy during ear surgery
- Facial palsy in CSOM = surgical emergency = mastoidectomy + decompression
- Nerve prolapse over oval window = major complication during stapedectomy
- Investigation: HRCT temporal bone (bone window); confirmed intraoperatively
This is a shared conversation. Sign in to Orris to start your own chat.