Facial nerve dehiscence
Reading File
search_medical_text
facial nerve dehiscence anatomy etiology clinical features management
search_medical_image
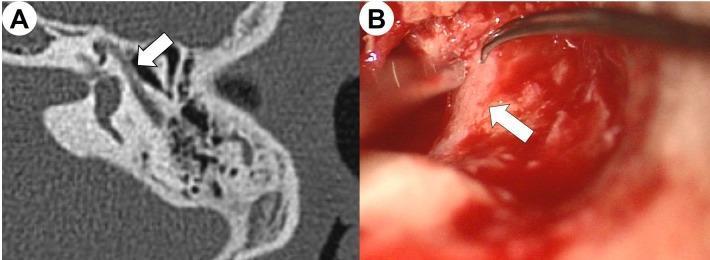
facial nerve dehiscence tympanic segment CT scan middle ear
GradeResponse
GradeResponse
Facial Nerve Dehiscence
Definition
Facial nerve dehiscence (FND) refers to the absence or deficiency of the bony wall (Fallopian canal) that normally encases the facial nerve as it courses through the temporal bone. The nerve is thus exposed — partially or completely — to the adjacent middle ear or mastoid spaces without its normal protective osseous covering.
Anatomy
The facial nerve traverses the temporal bone in three segments:
| Segment | Course | Vulnerability |
|---|---|---|
| Labyrinthine | From IAC fundus to geniculate ganglion | Narrowest segment |
| Tympanic (horizontal) | Geniculate ganglion → second genu (above oval window) | Most commonly dehiscent (~55–60% of cases) |
| Mastoid (vertical) | Second genu → stylomastoid foramen | Less common |
The tympanic segment, particularly just superior to the oval window and stapes, is the most frequent site of dehiscence. The nerve may even herniate into the middle ear space in severe cases.
Etiology & Prevalence
- Congenital/developmental: Most common cause. The bony canal fails to ossify fully; the overlying bone may be as thin as 0.1 mm or altogether absent.
- Prevalence: Cadaveric and CT studies report dehiscence in 6–50% of temporal bones, with significant variation based on methodology. Clinically significant dehiscence is far less common.
- Acquired causes:
- Chronic otitis media (erosion by cholesteatoma, granulation tissue)
- Temporal bone trauma/fracture
- Iatrogenic injury (prior surgery)
- Otosclerosis surgery
- Malignant otitis externa
- Radiation
Clinical Significance
Most cases of FND are asymptomatic and discovered incidentally. Clinical significance arises in two main contexts:
1. Iatrogenic Risk During Surgery
- The dehiscent nerve is vulnerable to injury during tympanoplasty, stapedectomy, cochlear implantation, mastoidectomy, and cholesteatoma surgery.
- An exposed nerve can be mistaken for a soft tissue structure and inadvertently damaged.
- Post-operative facial nerve palsy in the setting of ear surgery should prompt consideration of unrecognized dehiscence.
2. Association with Pathology
- Cholesteatoma: Can cause or worsen FND by eroding the Fallopian canal.
- Conductive hearing loss: A dehiscent nerve herniated over the oval window can impair stapes movement.
- Pulsatile tinnitus: Rare, from transmitted vascular pulsations directly to the exposed nerve.
- Spontaneous facial nerve palsy: In some cases of dehiscence, minor inflammation or middle ear effusion can compress the exposed nerve segment.
Imaging
HRCT (High-Resolution CT) of the temporal bone is the primary imaging modality.
- Look for: discontinuity or absence of the hyperdense bony covering of the Fallopian canal, best seen on axial and coronal bone-window cuts.
- CT has limited sensitivity for thin bony dehiscences (<0.5 mm); false negatives occur.
- MRI is complementary when soft tissue extension, perineural disease, or nerve enhancement is suspected.
Management
Preoperative
- HRCT review of all patients before ear surgery to identify dehiscence and plan accordingly.
- Neurotologic referral for complex cases.
Intraoperative
- Careful surgical technique near the oval window and tympanic segment.
- Identify the nerve early and trace its course before drilling or manipulating ossicles.
- If dehiscence is encountered incidentally and the nerve is intact, it can be left alone or the defect covered with fascia/cartilage.
When the Nerve is Symptomatic or Injured
| Scenario | Management |
|---|---|
| Incidental finding, no symptoms | Observation; counsel patient pre-/post-operatively |
| Conductive hearing loss from nerve herniation over oval window | Surgical decompression + repositioning; Gelfoam or fascial barrier placed between nerve and stapes |
| Facial palsy from cholesteatoma erosion | Cholesteatoma removal + nerve decompression |
| Iatrogenic injury (transection/crush) | Immediate neurorrhaphy or cable graft if > 50% disruption; decompression if intact but compressed |
| Delayed post-op palsy | Steroids, close monitoring; re-exploration if no recovery at 6 weeks |
Surgical Repair Options
- Fascial sheath repair: Temporalis fascia or perichondrium placed over the dehiscent segment.
- Nerve decompression: Opening the Fallopian canal proximal and distal to the injury site to relieve pressure.
- Nerve grafting: Greater auricular or sural nerve used for segmental defects > 1 cm.
Key Pearls
- The tympanic segment above the oval window is the most vulnerable and most commonly dehiscent portion.
- Dehiscence is often subclinical but becomes critical in the surgical context — always review HRCT before otologic surgery.
- A dehiscent facial nerve can mimic soft tissue (polyp, granulation) intraoperatively.
- Cholesteatoma is the most important acquired cause of progressive dehiscence.
- Post-operative facial palsy after ear surgery should raise suspicion for pre-existing unrecognized dehiscence.
This is a shared conversation. Sign in to Orris to start your own chat.