hii
Hi! How can I help you today?
i want know abate the coronary heart disese
Reading File
Finding Sources
Searching PubMed
"coronary heart disease"[MeSH Terms] AND "review"[pt]
Reading File
Finding Sources
Searching Images
coronary heart disease anatomy diagram
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
I now have comprehensive material from multiple authoritative textbooks to give you a thorough answer. Let me compile this into a clear overview.
Coronary Heart Disease (CHD)
Also called Coronary Artery Disease (CAD) or Ischaemic Heart Disease (IHD), CHD is the leading cause of death worldwide, responsible for roughly 2/3 of all cardiovascular deaths.
🫀 What Is It?
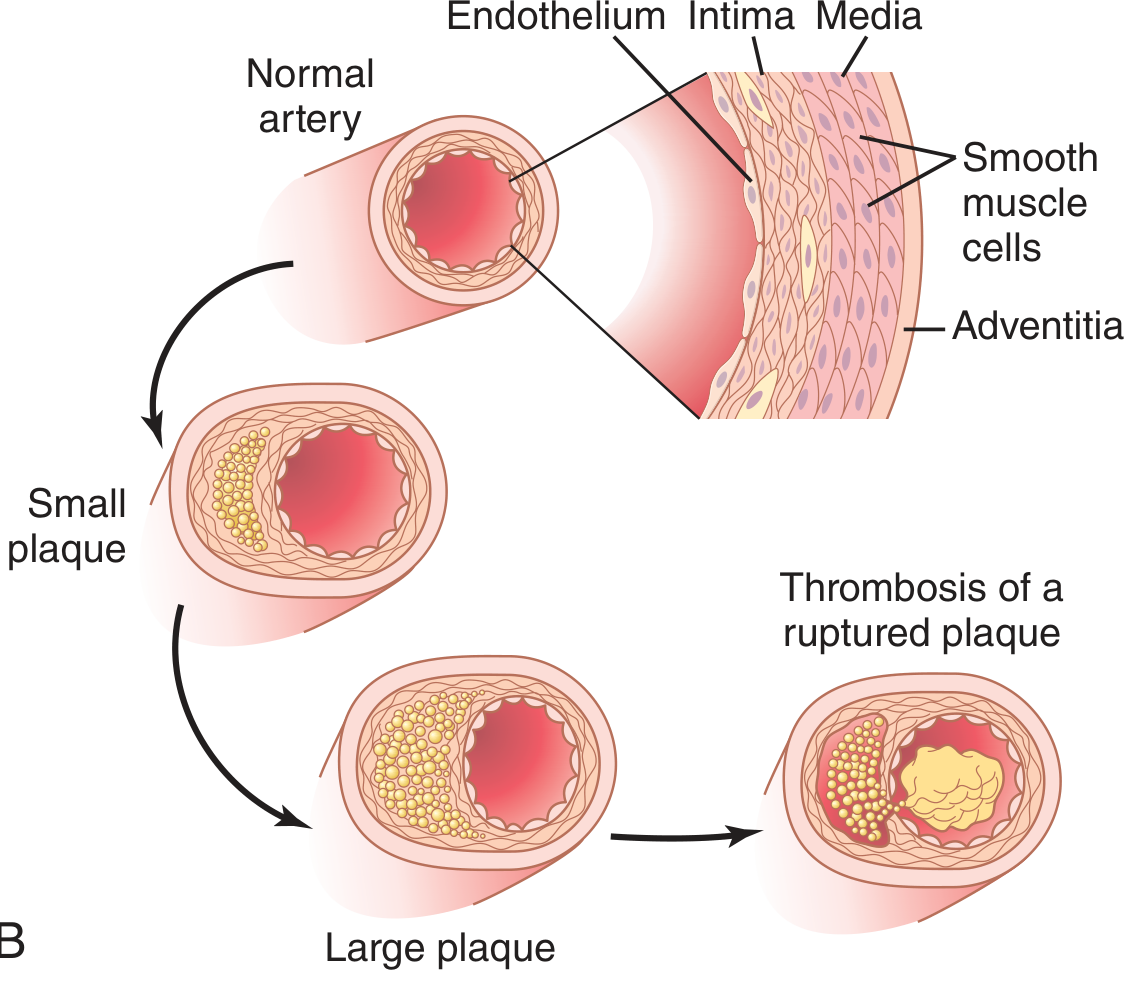
CHD occurs when atherosclerotic plaques (deposits of cholesterol, fats, and inflammatory cells) build up inside the walls of the coronary arteries — the vessels that supply blood and oxygen to the heart muscle. Over time, these plaques:
- Narrow the artery → reducing blood flow → causing angina (chest pain)
- Rupture → trigger a blood clot → suddenly block the artery → heart attack (myocardial infarction)
"Atheromatous plaques are raised lesions composed of soft friable lipid cores covered by fibrous caps. As they enlarge, they may mechanically obstruct vascular lumina... of greater concern is that they are prone to rupture, resulting in thrombosis and sudden occlusion of the vessel." — Robbins & Kumar Basic Pathology
🔬 How Atherosclerosis Develops
- Endothelial injury (from hypertension, smoking, high cholesterol, diabetes) damages the inner lining of coronary arteries
- LDL cholesterol enters the arterial wall and gets oxidized
- Monocytes migrate in, become macrophages, engulf oxidized LDL → form foam cells (fatty streaks)
- Smooth muscle cells proliferate and deposit fibrous tissue → forming a plaque
- Plaque grows, calcium deposits → artery stiffens ("hardening of the arteries")
- Plaque ruptures → clot forms → artery blocked → heart attack
⚠️ Risk Factors
Non-Modifiable
| Factor | Impact |
|---|---|
| Age | Risk increases with age |
| Sex | Men affected earlier; post-menopausal women catch up |
| Family history | Strong genetic component |
Modifiable (Most Important)
| Risk Factor | Notes |
|---|---|
| Smoking | 2–4× higher risk; 30% of all CHD deaths |
| High LDL cholesterol | Most directly linked to plaque formation |
| Hypertension | Damages endothelium, accelerates atherosclerosis |
| Diabetes mellitus | Damages vessels and nerves |
| Obesity | Promotes hypertension, diabetes, and dyslipidemia |
| Physical inactivity | Lowers HDL, raises LDL |
| Unhealthy diet | High saturated fats → high LDL |
"When hypertension, diabetes mellitus, and hyperlipidemia are all present, the risk for atherosclerotic coronary artery disease is increased almost 20-fold." — Guyton and Hall Textbook of Medical Physiology
🩺 Symptoms
| Symptom | Description |
|---|---|
| Angina pectoris | Chest tightness/pressure, often triggered by exertion or stress, relieved by rest |
| Shortness of breath | From reduced heart pumping ability |
| Heart attack (MI) | Severe chest pain, sweating, nausea, arm/jaw pain — a medical emergency |
| Silent ischemia | No symptoms, especially common in diabetics |
🔍 Diagnosis
- ECG (electrocardiogram) — detects ischemia or MI
- Stress testing — exercise treadmill/bicycle, nuclear imaging, stress echocardiography
- Coronary CT Angiography (CCTA) — preferred for younger patients / lower-risk cases
- Cardiac catheterization (coronary angiogram) — gold standard, directly visualizes blockages
- Blood tests: Troponin (for MI), lipid panel, blood glucose, CRP
💊 Treatment
Lifestyle Changes (First Line)
- Quit smoking — risk drops by ~50% in the first year; returns to near-normal after 15 years
- Heart-healthy diet — low saturated fat, more vegetables, fish, whole grains
- Regular exercise — at least 150 minutes/week moderate intensity
- Weight loss, stress reduction
Medications
| Drug Class | Purpose |
|---|---|
| Statins (e.g., atorvastatin) | Lower LDL cholesterol, stabilize plaques |
| Aspirin / antiplatelets | Prevent blood clots |
| Beta-blockers | Lower heart rate and blood pressure |
| ACE inhibitors / ARBs | Protect heart and vessels |
| Nitrates | Relieve angina |
| Calcium channel blockers | Dilate arteries, reduce workload |
Procedures
| Procedure | When Used |
|---|---|
| PCI (Percutaneous Coronary Intervention / Stenting) | Preferred for acute heart attacks; opens blocked artery |
| CABG (Coronary Artery Bypass Grafting) | Surgery to bypass blocked arteries; preferred for complex/multi-vessel disease |
"Refractory angina and acute coronary syndromes are best treated with physical revascularization, i.e., PCI with stents, or CABG." — Katzung's Basic and Clinical Pharmacology, 16th Ed.
🛡️ Prevention Summary
| Action | Benefit |
|---|---|
| Quit smoking | Most impactful single change |
| Control blood pressure | Reduces CHD events significantly |
| Lower LDL with statins | Reduces plaques and heart attacks |
| Control blood sugar | Slows vascular damage |
| Exercise regularly | Improves HDL, lowers blood pressure |
| Maintain healthy weight | Reduces all major risk factors |
Sources: Robbins & Kumar Basic Pathology; Guyton and Hall Textbook of Medical Physiology; Goldman-Cecil Medicine; Braunwald's Heart Disease; Katzung's Basic and Clinical Pharmacology, 16th Ed.
coronary circulation
Finding Sources
Searching Images
coronary circulation arteries anatomy diagram
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Here is a comprehensive overview of the coronary circulation, drawn from Guyton & Hall, Costanzo, Barash, Katzung, and Medical Physiology textbooks.
Coronary Circulation
The coronary circulation is the blood supply system of the heart itself — it delivers oxygen and nutrients to the myocardium (heart muscle) and removes waste products.
🫀 Anatomy of the Coronary Arteries
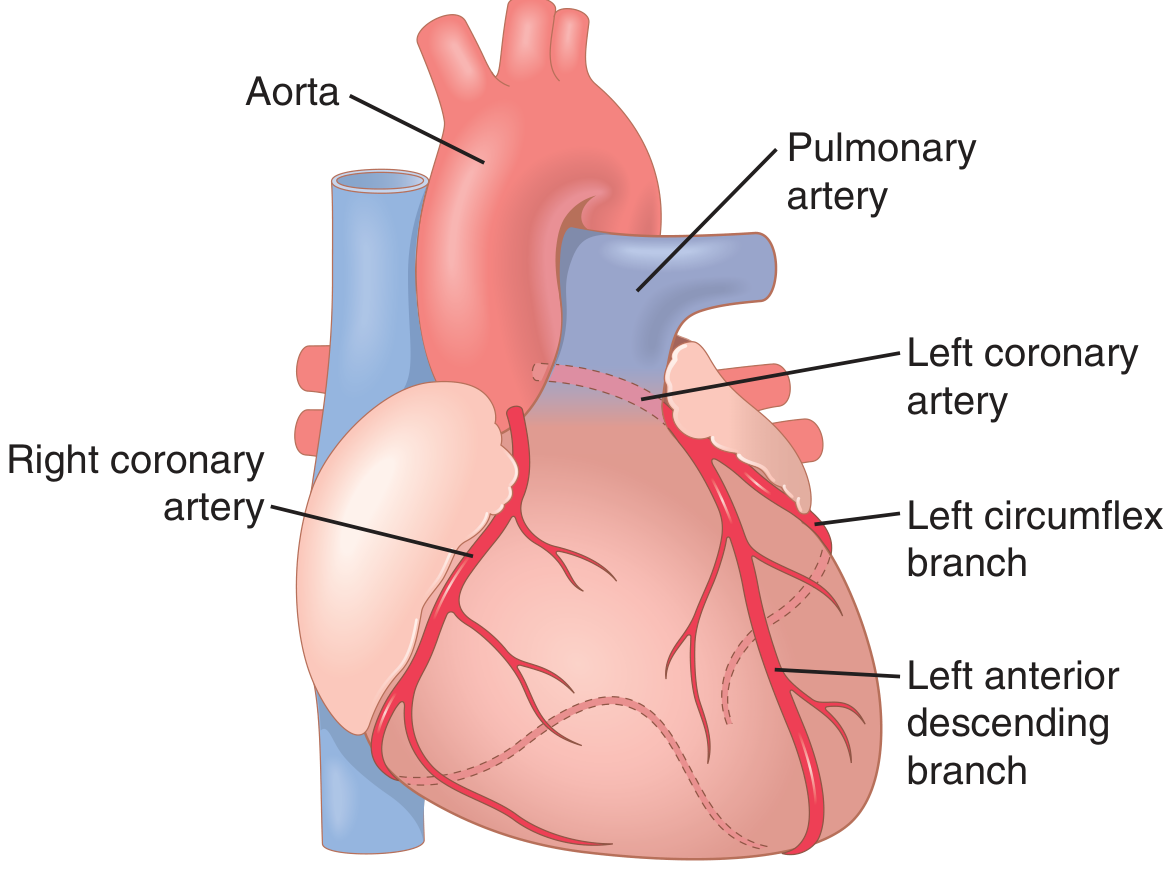
The coronary arteries arise from the aortic root, just above the aortic valve, and divide into two main trunks:
Left Coronary Artery (LCA)
Divides into two major branches:
- Left Anterior Descending (LAD) — supplies the anterior wall of the left ventricle and interventricular septum
- Left Circumflex (LCx) — supplies the lateral and posterior walls of the left ventricle
Right Coronary Artery (RCA)
- Supplies the right ventricle and, in most people, the posterior left ventricle
- In 80–90% of people (right-dominant), the RCA gives off the posterior descending artery (PDA)
"The left coronary artery supplies mainly the anterior and left lateral portions of the left ventricle, whereas the right coronary artery supplies most of the right ventricle, as well as the posterior part of the left ventricle in 80% to 90% of people." — Guyton and Hall Textbook of Medical Physiology
Layers of Supply
- Epicardial arteries — run on the outer surface of the heart
- Intramuscular arteries — penetrate deep into the myocardium
- Subendocardial plexus — supplies the innermost layer (most vulnerable to ischemia)
🔄 Venous Drainage
| Vessel | Drains From | Empties Into |
|---|---|---|
| Coronary sinus | ~75% of LV venous blood | Right atrium |
| Anterior cardiac veins | Right ventricle | Right atrium directly |
| Thebesian veins | Minute drainage | All cardiac chambers |
⏱️ Phasic Flow: Systole vs. Diastole
This is the most unique feature of coronary circulation:
- During systole: The contracting left ventricular muscle compresses the intramuscular coronary vessels → blood flow through the left coronary artery drops sharply (near zero in subendocardial vessels)
- During diastole: Muscle relaxes → vessels decompress → ~80% of left coronary flow occurs in diastole
- The right coronary artery is less affected because right ventricular contraction force is much less
"Coronary blood flow to the LV occurs almost entirely during diastole because extravascular compressive forces are exerted on the subendocardial intramural vessels during contraction." — Barash's Clinical Anesthesia, 9e
Clinical implication: Tachycardia (fast heart rate) shortens diastole → reduces coronary filling time → worsens myocardial ischemia.
📊 Normal Coronary Blood Flow
| Parameter | Value |
|---|---|
| Resting flow | ~70 mL/min per 100 g heart |
| Total resting flow | ~225 mL/min |
| % of cardiac output | 4–5% |
| Oxygen extraction at rest | ~70% of delivered O₂ |
| Increase during maximal exercise | 3–4× |
Since the heart already extracts ~70% of oxygen at rest, it cannot increase oxygen extraction much more when demand rises. Therefore, increased O₂ demand must be met almost entirely by increasing blood flow.
🧬 Regulation of Coronary Blood Flow
1. Local Metabolic Regulation (Most Important)
When cardiac workload increases → O₂ consumption rises → local hypoxia → release of vasodilator substances → coronary arterioles dilate → flow increases.
Key vasodilators released:
| Substance | Source |
|---|---|
| Adenosine | Most potent — from ATP breakdown in hypoxic myocytes |
| Nitric oxide (NO) | Endothelium |
| CO₂ / H⁺ | Metabolic byproducts |
| K⁺ | From active muscle cells |
| Prostaglandins | Vascular wall |
"Blood flow through the coronary system is regulated mostly by local arteriolar vasodilation in response to the metabolic needs of cardiac muscle. Whenever the vigor of cardiac contraction is increased, the rate of coronary blood flow also increases." — Guyton and Hall Textbook of Medical Physiology
2. Autoregulation
Coronary flow remains relatively constant between aortic pressures of ~70–150 mmHg, protecting the heart from pressure fluctuations.
3. Nervous Control
| Stimulus | Direct Effect | Net Effect |
|---|---|---|
| Sympathetic (norepinephrine) | α-receptors → vasoconstriction (epicardial); β-receptors → vasodilation (intramuscular) | Metabolic override → net vasodilation (↑ heart work) |
| Parasympathetic (acetylcholine) | Direct vasodilation | Net vasoconstriction (↓ heart work) |
Metabolic factors always override direct nervous effects within seconds.
4. Reactive Hyperemia
During systolic compression, an oxygen debt accumulates. When compression ends (diastole), there is a burst of reactive hyperemia to repay that debt.
⚡ Cardiac Metabolism
- At rest: ~70% of energy from fatty acid oxidation
- Under ischemia/hypoxia: switches to anaerobic glycolysis → produces lactic acid → causes anginal pain
🩺 Clinical Relevance
| Condition | Mechanism |
|---|---|
| Angina pectoris | Demand exceeds supply; subendocardium most vulnerable |
| Coronary artery disease | Atherosclerotic plaques narrow arteries |
| Vasospastic angina (Prinzmetal) | Excess α-adrenergic coronary constriction |
| Tachycardia worsening ischemia | Shortens diastolic filling time |
| Subendocardial infarction | Innermost layer most susceptible (compressed longest) |
Sources: Guyton and Hall Textbook of Medical Physiology; Costanzo Physiology 7th Ed.; Barash's Clinical Anesthesia 9th Ed.; Katzung's Basic and Clinical Pharmacology 16th Ed.; Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.