Infective endocarditis microbiology
Reading File
Finding Sources
Searching PubMed
"infective endocarditis" AND microbiology
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - I now have a comprehensive picture from multiple authoritative sources. Here is the full answer:
Infective Endocarditis - Microbiology
Overview of the Microbial Spectrum
IE results from microbial adherence to damaged valvular endothelium, where platelets and fibrin form a nidus to which organisms bind. Three species account for the majority of cases: S. aureus, viridans group streptococci, and enterococci. The likely causative organism varies by valve type, route of acquisition, and host risk factors.
From the ICE (International Collaboration on Endocarditis) Prospective Cohort Study (2,781 adults, 25 countries):
| Organism | % of IE Cases |
|---|---|
| Staphylococcus aureus | 31% |
| Viridans group streptococci | 17% |
| Enterococci | 11% |
| Coagulase-negative staphylococci | 11% |
| Streptococcus gallolyticus | 6% |
| Other streptococci (incl. nutritionally variant) | 6% |
| Culture-negative | 10% |
| HACEK | 2% |
| Non-HACEK gram-negative bacteria | 2% |
| Fungi/yeast | 2% |
| Polymicrobial | 1% |
- Fuster and Hurst's The Heart, 15th Ed., p. 1028
Classification by Valve Type and Clinical Setting
The endocarditis classification flowchart below summarizes organisms by context:
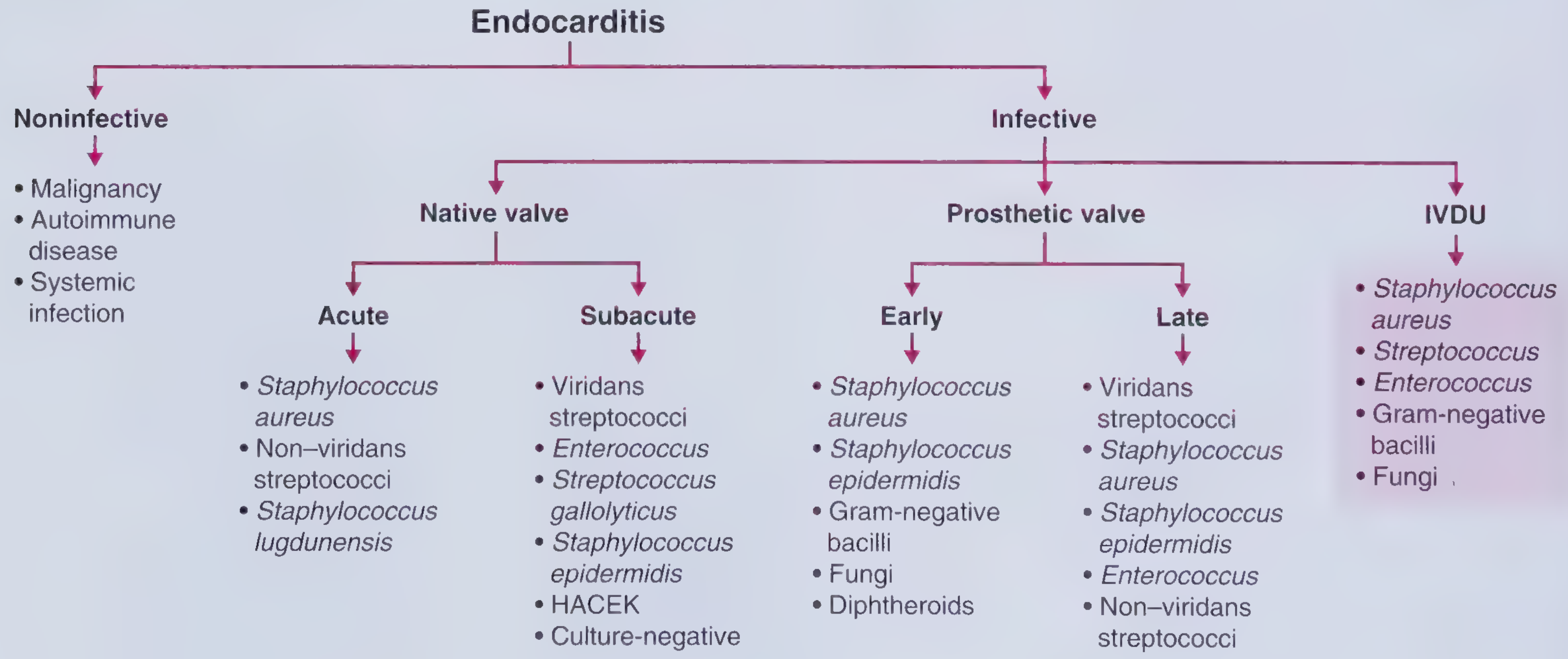
- Frameworks for Internal Medicine
1. Native Valve IE (NVIE)
Predominantly gram-positive cocci. S. aureus is now the most common single pathogen overall, with rising incidence driven by healthcare-associated bacteremia (IV catheters, hemodialysis, invasive procedures).
Streptococci
- Viridans group streptococci (VGS) - normal oropharyngeal flora; classic cause of subacute community-acquired IE following dental procedures. Key species: S. sanguinis, S. mutans, S. mitior, S. gallolyticus
- S. gallolyticus (formerly S. bovis) - bacteremia with this organism should prompt colonoscopy, as GI malignancy, polyps, or inflammatory disease are associated in up to 60% of cases
- Nutritionally variant streptococci (Abiotrophia and Granulicatella spp.) - require specialized culture media; have diminished susceptibility to penicillins/cephalosporins and often need aminoglycoside combination therapy
- S. pneumoniae IE - rare but acute and fulminant; causes severe valve damage with high mortality
- Group B streptococci (S. agalactiae) - associated with obstetric complications, diabetes, liver disease, alcoholism, and injection drug use
Staphylococci
- S. aureus - the dominant pathogen in acute IE; possesses virulence factors (fibronectin-binding proteins, coagulase) allowing adherence to endothelium and evasion of host defenses; 80-90% of staphylococcal IE is due to S. aureus. Risk is elevated with hemodialysis, diabetes, HIV, and recent surgery
- Coagulase-negative staphylococci (CoNS) - mainly S. epidermidis; principally affect prosthetic/damaged valves and intracardiac devices rather than intact native endothelium
- S. lugdunensis - a CoNS that behaves like S. aureus clinically, with high rates of perivalvular extension and metastatic spread
Enterococci
- Cause ~5-10% of subacute bacterial endocarditis
- Normal GI/genitourinary flora; bacteremia follows GU or GI instrumentation
- E. faecalis is more common and virulent than E. faecium in native valve disease
- High-level antibiotic resistance is increasingly common in healthcare-associated strains
- Frequently associated with prosthetic materials and indwelling catheters
2. Prosthetic Valve IE (PVE)
| Timing | Organisms |
|---|---|
| Early PVE (<1 year, esp. <2 months post-op) | S. aureus, CoNS (S. epidermidis), gram-negative bacilli, Candida spp., diphtheroids |
| Late PVE (>1 year) | Same as NVIE - viridans streptococci, S. aureus, CoNS, Enterococcus, non-viridans streptococci |
- The Washington Manual of Medical Therapeutics; Bailey & Love's Surgery, 28th Ed., Table 59.3
3. IV Drug Use (IVDU)-Associated IE
- S. aureus is responsible for >50% of cases; causes predominantly right-sided (tricuspid valve) endocarditis
- Viridans streptococci, Enterococcus, gram-negative bacilli, fungi also occur
- Eikenella corrodens (a HACEK organism) - linked to needle/skin licking; infection is often a standalone surgical indication
- Pseudomonas aeruginosa - rare, more common in PWID
4. HACEK Organisms
HACEK = Haemophilus (aphrophilus, parainfluenzae, paraphrophilus), Aggregatibacter actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, Kingella kingae
- Fastidious, slow-growing gram-negative rods; normal oropharyngeal flora
- Account for ~2% overall IE; 5-10% of community-acquired cases
- May take 3-4 weeks on standard culture (accelerated to 5-7 days with BACTEC systems)
- Classically form large, friable vegetations prone to embolization
- Particularly affect immunocompromised patients, prosthetic valve recipients, and IVDU
5. Fungi
- Candida (52%) and Aspergillus (24%) are the dominant fungal pathogens
- Seen in immunocompromised hosts and patients with indwelling devices
- Bulky vegetations - prone to large vessel embolization and even valve obstruction
- Aspergillus is almost never culture-positive from blood; diagnosis relies on serology/PCR
- Treatment nearly always requires combined medical and surgical management including prosthetic valve removal; chronic suppressive antifungal therapy is needed
- Mortality is extremely high
6. Culture-Negative IE (~10% of cases)
Defined as IE with no microbiologic identification after ≥3 blood cultures incubated for ≥7 days. Key causes:
| Organism | Key Clue |
|---|---|
| Coxiella burnetii (Q fever) | Exposure to cattle, sheep, goats; zoonotic |
| Bartonella spp. | Homeless individuals, HIV infection, cat scratch exposure |
| Brucella spp. | Unpasteurized dairy, livestock handlers (4% of IE in Spain) |
| Legionella spp. | Environmental water sources |
| Tropheryma whipplei | Whipple's disease features |
| Cutibacterium (Propionibacterium) acnes | Prosthetic material; very slow growth (median 5.5 days) |
| Nutritionally variant streptococci | Require specialized culture media |
| Prior antibiotic therapy | Most common preventable cause |
Diagnosis uses serology (Coxiella, Bartonella, Brucella, Legionella) and PCR on blood or explanted valve tissue.
Key Clinical Associations Summary
| Context | Most Likely Organism(s) |
|---|---|
| Community-acquired, dental procedure | Viridans streptococci |
| Healthcare-associated, IV catheter | S. aureus, CoNS |
| Colonic malignancy/polyps | S. gallolyticus |
| IV drug use, tricuspid | S. aureus |
| Early prosthetic valve | S. epidermidis, S. aureus, gram-negatives, Candida |
| Zoonotic exposure (cattle/sheep) | Coxiella burnetii |
| Immunocompromised | Candida, Aspergillus |
| Homeless/HIV | Bartonella spp. |
| Oropharyngeal needle licking (IVDU) | Eikenella corrodens |
Recent evidence note: A 2025 meta-analysis of 133 studies (PMID 40015544) characterizes the current epidemiological profile of IE and may update some incidence figures, particularly the continued rise of S. aureus as the dominant pathogen in developed healthcare settings.
- Primary sources: Fuster and Hurst's The Heart 15th Ed.; Washington Manual of Medical Therapeutics; Bailey & Love's Surgery 28th Ed.; Frameworks for Internal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.