pericoronitis
Reading File
Finding Sources
Searching PubMed
pericoronitis
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Excellent - I now have comprehensive content from four textbooks plus the diagram image. I have enough to write a detailed, well-structured answer.
Pericoronitis
Pericoronitis is inflammation of the operculum - the gingival tissue (gum flap) overlying the occlusal surface of an erupting or partially erupted tooth. It is the most common dental emergency in young adults.
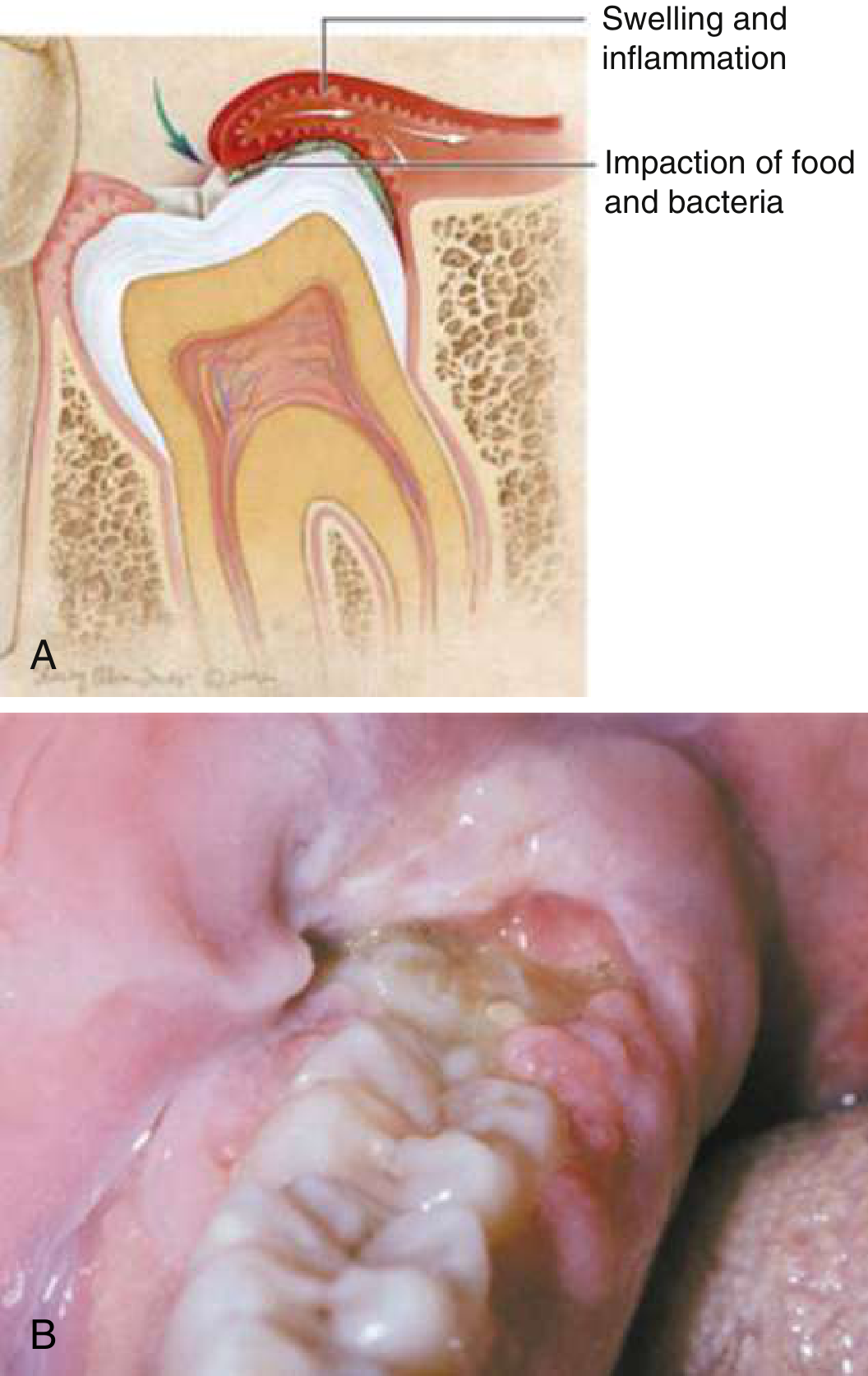
Anatomy and Pathophysiology
As a tooth erupts, a flap of gum tissue (the operculum) partially covers the crown. Debris and bacteria accumulate in the space beneath this flap, triggering an inflammatory response. The condition is worsened by trauma from biting (mastication against the opposing arch). The most commonly implicated tooth is the mandibular third molar (wisdom tooth), with symptoms typically arising in the 2nd or 3rd decade of life. Any partially erupted or impacted/malerupted tooth can be affected. The microbes predominantly responsible are gram-negative anaerobes (including Fusobacterium and spirochetes). - Rosen's Emergency Medicine, p. 860; Scott-Brown's Otorhinolaryngology, p. 702
Clinical Features
| Feature | Detail |
|---|---|
| Pain | Moderate to severe; aggravated by jaw movement and mastication |
| Swelling | Inflamed operculum, localized facial swelling |
| Trismus | Due to irritation of masseter and pterygoid muscles |
| Halitosis | Foul breath from trapped debris |
| Referred pain | Commonly to the ipsilateral ear |
| Lymphadenopathy | Regional nodes enlarged |
| Pus | Expressible from beneath the tissue flap on probing |
Examination with a tongue blade or finger elicits tenderness over the operculum and may produce drainage. - Roberts & Hedges' Clinical Procedures in Emergency Medicine, p. 2064
Complications and Spread
The proximity of the third molar to the masticator space (masseteric, pterygomandibular, superficial and deep temporal spaces) means infection can spread:
- Trismus - infection spreading to the pterygomandibular or submasseteric space
- Parapharyngeal space infection - if further spread occurs, this can be life-threatening (airway compromise)
- Ludwig's angina is the extreme end of this spectrum
Any signs of trismus, regional lymphadenopathy, or spreading infection are red flags for systemic spread. - Tintinalli's Emergency Medicine, p. 1622
Investigations
No laboratory or radiographic testing is routinely indicated for uncomplicated pericoronitis. Consider panoramic radiograph to assess tooth impaction and planned extraction. - Rosen's Emergency Medicine
Management
Mild to Moderate (localized, no systemic signs)
- Local irrigation - thorough debridement of food and debris from beneath the operculum
- Saline/chlorhexidine rinses - chlorhexidine 0.2% is the preferred topical agent; also saline rinses
- Analgesia - NSAIDs (ibuprofen 400-600 mg q6-8h) or acetaminophen (650 mg q6h); opioids for severe pain
- Antibiotics - only if pericoronitis is severe or systemic signs are present (see below); not needed for mild/localized cases
- Dental referral - within 24-48 hours for local treatment of the operculum or tooth extraction
Indications for Systemic Antibiotics
- Regional lymphadenopathy
- Trismus
- Signs of spreading infection
- Immunocompromised host
Antibiotic Regimens (Severe Pericoronitis)
| Antibiotic | Dose | Duration | Notes |
|---|---|---|---|
| Penicillin V | 500 mg PO tid-qid | 10 days | First-line |
| Amoxicillin/clavulanate | 500 mg/125 mg PO tid | 10 days | Alternative |
| Metronidazole | 500 mg PO bid | 10 days | Penicillin allergy; targets gram-negative anaerobes |
| Clindamycin | 300 mg PO qid | 10 days | Penicillin allergy |
Penicillin 500 mg q8h for 5-7 days is a common shorter course for pericoronitis specifically. Metronidazole is preferred in some guidelines given the predominance of gram-negative anaerobes. - Rosen's Emergency Medicine; Scott-Brown's Otorhinolaryngology, p. 702
Severe/Spreading Infection (trismus, systemic signs)
- IV antibiotics urgently
- ENT or oral surgery urgent consultation
- Drainage procedures are usually required, often necessitating extraction of the offending tooth
Disposition
- Localized pericoronitis: discharge with oral antibiotics (if indicated), mouth rinses, analgesia, and dental follow-up in 24-48 hours
- Patients should be referred to a dentist or oral surgeon for operculum treatment or tooth removal (especially if tooth is impacted/malerupted)
- Spreading infection with trismus or airway concern: hospital admission, IV antibiotics, urgent surgical consult
Differential Diagnosis (Odontogenic orofacial pain)
- Dental caries / pulpitis
- Periapical abscess
- Periodontal abscess
- Acute necrotizing gingivostomatitis (ANUG)
- Sialadenitis / parotitis
- Temporomandibular disorder
Sources: Rosen's Emergency Medicine, p. 860 | Tintinalli's Emergency Medicine, p. 1622 | Scott-Brown's Otorhinolaryngology, p. 702 | Roberts & Hedges' Clinical Procedures in Emergency Medicine, p. 2064
Recent evidence note: A 2024 systematic review on metronidazole for oral anaerobic infections (PMID 39120079) supports its use as monotherapy for pericoronitis, consistent with guidelines recommending it as the agent of choice for penicillin-allergic patients given the gram-negative anaerobic predominance.
This is a shared conversation. Sign in to Orris to start your own chat.