Please explain and help me remember national immunisation schedule. Also explain how it is formed, who forms it in which phase it is currently and all the recent updates in national immunisation schedule
India national immunization schedule 2024 2025 recent updates UIP vaccines
"national immunization schedule" India UIP vaccines
https://www.pib.gov.in/PressReleasePage.aspx?PRID=2241066
India UIP universal immunization programme NTAGI ITAG schedule formation phase 2025
PMID: 40252840
India HPV vaccine cervical cancer NIS 2026 rotavirus PCV IPV schedule update NTAGI recommendation
National Immunisation Schedule (NIS) - India (UIP) - Complete Guide
1. What Is the National Immunisation Schedule?
2. How It Is Formed - The Process
| Criteria | Meaning |
|---|---|
| Immunologically effective | Given at the right age when maternal antibody wanes; sufficient interval between doses |
| Epidemiologically sound | Targeting diseases with high burden, morbidity/mortality in the population |
| Operationally feasible | Minimise visits, simultaneous administration, cold chain viable, affordable |
| Socially acceptable | Account for local customs, seasonal factors, community practices |
The Body That Forms It - NTAGI
- Review disease burden data (morbidity, mortality, epidemiology)
- Assess vaccine safety and efficacy data
- Evaluate equity considerations (does it reach the most vulnerable?)
- Assess financial sustainability (Government of India + donor support)
- Review logistical implications (cold chain, storage, supply chain)
- Make a formal recommendation to MoHFW
- MoHFW approves and releases operational guidelines
3. Historical Evolution / Phases
| Year | Milestone |
|---|---|
| 1974 | WHO launches EPI (Expanded Programme on Immunisation) globally - 6 vaccines: BCG, DPT, OPV, Measles, TT |
| 1978 | India adopts EPI (without Measles initially) |
| 1983 | TT vaccine added for pregnant women |
| 1985 | EPI renamed Universal Immunisation Programme (UIP), launched November 19, 1985 (dedicated to Indira Gandhi) |
| 1989-90 | Phase-wise expansion to all districts complete |
| 1992 | UIP becomes part of Child Survival & Safe Motherhood Programme |
| 1997 | Integrated into Reproductive & Child Health (RCH) Programme |
| 2000-01 | NTAGI established; systematic process for new vaccine introduction begins |
| 2005 | UIP under National Rural Health Mission (NRHM) |
| 2010 | Pentavalent vaccine (DPT+HepB+Hib) pilot in Kerala and Tamil Nadu |
| 2014 | Mission Indradhanush launched to improve immunisation coverage |
| 2014-16 | IPV introduced; Rotavirus vaccine (RVV) introduced in select states |
| 2017 | PCV (Pneumococcal Conjugate Vaccine) introduced in select states |
| 2017 | MR (Measles-Rubella) vaccine replaces standalone Measles vaccine |
| 2019 | PCV, RVV, IPV scaled up nationally |
| 2021-22 | Td (Tetanus-Diphtheria) replaces TT vaccine |
| 2026 | HPV vaccine campaign + indigenously made Td vaccine launched |
4. Current NIS Schedule (2025-2026)
For Infants and Children
| Age | Vaccines |
|---|---|
| At Birth | BCG (0.1 mL, intradermal, left upper arm), OPV-0 (2 drops oral), Hepatitis B birth dose (0.5 mL, IM, anterolateral thigh) |
| 6 Weeks | OPV-1, Pentavalent-1 (DPT+HepB+Hib), fIPV-1 (fractional IPV, 0.1 mL intradermal), RVV-1 (Rotavirus), PCV-1 |
| 10 Weeks | OPV-2, Pentavalent-2, RVV-2 |
| 14 Weeks | OPV-3, Pentavalent-3, fIPV-2, RVV-3, PCV-2 |
| 9-12 Months | MR-1 (Measles-Rubella), JE-1* (Japanese Encephalitis), PCV Booster |
| 16-24 Months | MR-2, JE-2*, DPT Booster-1, OPV Booster |
| 5-6 Years | DPT Booster-2 |
| 10 Years | Td (Tetanus + adult Diphtheria) |
| 16 Years | Td |
For Pregnant Women
| Timing | Vaccine |
|---|---|
| Early pregnancy | Td-1 |
| 4 weeks after Td-1 | Td-2 |
| If vaccinated within last 3 years | Td-Booster only |
5. Key Vaccines - What They Protect Against
| Vaccine | Full Form | Diseases Prevented |
|---|---|---|
| BCG | Bacillus Calmette-Guérin | Severe childhood tuberculosis (miliary TB, TB meningitis) |
| OPV | Oral Polio Vaccine | Poliomyelitis |
| Hep B | Hepatitis B | Hepatitis B, liver cirrhosis, hepatocellular carcinoma |
| Pentavalent | DPT + HepB + Hib | Diphtheria, Pertussis, Tetanus, Hepatitis B, H. influenzae type b |
| fIPV | Fractional Inactivated Polio Vaccine | Polio (induces mucosal immunity, used with OPV) |
| RVV | Rotavirus Vaccine | Rotavirus diarrhoea (major cause of infant death) |
| PCV | Pneumococcal Conjugate Vaccine | Pneumococcal pneumonia, meningitis, sepsis |
| MR | Measles-Rubella | Measles + Rubella (congenital rubella syndrome) |
| JE | Japanese Encephalitis | Japanese encephalitis (fatal viral encephalitis) |
| DPT Booster | Diphtheria-Pertussis-Tetanus | Boosting primary series immunity |
| Td | Tetanus + adult Diphtheria | Tetanus, diphtheria (in older children + pregnant women) |
6. Recent Updates (2024-2026) - Most Important
a) Nationwide HPV Vaccination Campaign (February 28, 2026)
- Launched by Prime Minister Modi from Ajmer, Rajasthan
- Target: 14-year-old girls (adolescent girls, single dose)
- Scale: ~1.15 crore (11.5 million) girls across India
- Free of cost at government health facilities
- India accounts for ~25% of global cervical cancer deaths (~80,000 per year)
- This is India's first large-scale HPV immunisation drive under UIP
b) Indigenous Td Vaccine Launch (February 21, 2026)
- Manufactured at Central Research Institute (CRI), Kasauli
- Replaces the older TT (Tetanus Toxoid) vaccine in the schedule
- ~55 lakh doses to be supplied to UIP by April 2026
- Marks India's self-reliance (Atmanirbhar Bharat) in vaccine production
c) Coverage Milestone
- Full immunisation coverage rose from 62% in 2015 to 98.4% as of January 2026
- Zero-dose children declined from 0.11% (2023) to 0.06% (2024) of total population
d) Mission Indradhanush
- Ongoing campaign to reach left-out and drop-out children and pregnant women
- Has completed multiple rounds (Intensified Mission Indradhanush 2.0, 3.0, 4.0)
e) PCV Nationwide Scale-Up
- PCV (Pneumococcal Conjugate Vaccine) scaled up pan-India - protects against the leading cause of bacterial pneumonia deaths in children
7. UIP vs IAP Schedule - Key Difference
| Feature | UIP (Government/NIS) | IAP Schedule |
|---|---|---|
| Cost | Free | Paid (private) |
| Vaccines | 12 core antigens | More vaccines (typhoid conjugate, Hep A, Varicella, MMR, influenza, etc.) |
| Recommended by | MoHFW/NTAGI | Indian Academy of Pediatrics |
| Setting | Government health centres | Private hospitals/clinics |
8. Memory Tricks - Mnemonic for NIS
| Letter | Vaccine | Age |
|---|---|---|
| Born | BCG, OPV-0, HepB | Birth |
| On | OPV-1, Penta-1, fIPV-1, RVV-1, PCV-1 | 6 Weeks |
| Planet | OPV-2, Penta-2, RVV-2 | 10 Weeks |
| Reach | OPV-3, Penta-3, fIPV-2, RVV-3, PCV-2 | 14 Weeks |
| For | MR-1, JE-1, PCV-Booster | 9-12 Months |
| Perfection | MR-2, JE-2, DPT-B1, OPV-B | 16-24 Months |
| Make | DPT Booster-2 | 5-6 Years |
| Jolly | Td | 10 Years |
| Durable | Td | 16 Years |
| Pregnant | Td-1, Td-2 or Td-Booster | Pregnancy |
9. Quick Recall Table
BIRTH → BCG + OPV0 + HepB
6 wk → OPV1 + Penta1 + fIPV1 + RVV1 + PCV1
10 wk → OPV2 + Penta2 + RVV2
14 wk → OPV3 + Penta3 + fIPV2 + RVV3 + PCV2
9-12m → MR1 + JE1 + PCV-B
16-24m → MR2 + JE2 + DPT-B1 + OPV-B
5-6 yr → DPT-B2
10 yr → Td
16 yr → Td
Preg → Td1 + Td2 (or Booster)
- Park's Textbook of Preventive and Social Medicine (23rd Ed.), Section: National Immunisation Schedule, NIS Table 43
- PIB India Press Release (March 2026) - UIP milestones and 2026 launches
- Jacob John T & Kompithra RZ (2025). "India's universal immunization program: A review of successes, challenges, and future directions." Indian Journal of Medical Microbiology [PMID: 40252840]
- ITSU cMYP 2018-22 (NTAGI structure and new vaccine introduction process)
we are currently in which mission Indradhanush phase?
Mission Indradhanush current phase 2025 2026 India immunization
Intensified Mission Indradhanush IMI 5.0 phase 2025 2026 launch
https://www.jaagrukbharat.com/mission-indradhanush-strengthe…
Mission Indradhanush - All Phases at a Glance
Current Phase: IMI 5.0 (Most Recent)
- Measles-Rubella (MR) vaccination catch-up
- Targeting children up to 5 years
- Introduction of the U-WIN smart card for digital vaccine tracking
Complete Phase Timeline
| Phase | Year | Key Features |
|---|---|---|
| Mission Indradhanush 1.0 | Dec 2014 | Launched Dec 25, 2014; targeted 201 high-priority districts; 7 vaccines |
| MI 2.0 | 2015-16 | Expanded to 352 districts; 4 rounds |
| MI 3.0 | 2016-17 | Urban focus; added vaccines (Hep B, Hib) |
| MI 4.0 | 2017 | Included rotavirus-endemic districts |
| Intensified MI (IMI) 1.0 | Oct 2017 | ~2.53 crore children vaccinated; 121 districts including conflict zones; OPV replaced by IPV |
| IMI 2.0 | 2019-20 | Larger scope; included pregnant women specifically |
| IMI 3.0 | Feb-Apr 2022 | Post-COVID catch-up; 416 districts; included MR; launched U-WIN digitisation |
| IMI 4.0 | Feb-Apr 2023 | 416 districts; 33 states/UTs; focused on left-out zero-dose children |
| IMI 5.0 | Aug-Oct 2023 | MR catch-up drive; 3 sub-phases; U-WIN smart card rollout; 765 districts total cumulatively |
Key Points to Remember
- Total phases so far: 12 rounds (as of 2023, per PIB 2026)
- Current/latest named phase: IMI 5.0 (2023)
- Post-IMI 5.0 (2024-26): Routine UIP + HPV campaign (Feb 2026) + indigenous Td vaccine, but no new "IMI 6.0" has been officially announced as of May 2026
- The programme continues in routine immunisation mode with Mission Indradhanush rounds conducted periodically between the numbered phases
Quick Memory Trick
- MI 1-4 = 2014-2017 (Regular phases, district expansion)
- IMI 1-5 = 2017-2023 (Intensified, post-COVID catch-up, digital tracking)
- IMI 3.0 onward = U-WIN (digital vaccination records)
What is U-WIN and how does it work in vaccine tracking?
U-WIN platform India immunization tracking system how it works features 2024 2025
U-WIN - India's Universal Immunisation Digital Platform
What Is U-WIN?
- Nationally launched: October 2024 by the Prime Minister
- Built on the eVIN + CoWIN framework - i.e., the same technological architecture that powered India's COVID-19 vaccination drive
- Available in 12 Indian languages including English
- As of 2024: became the largest digital immunisation repository in the world
The Digital Health Trilogy Behind It
| Platform | Full Name | Purpose |
|---|---|---|
| eVIN | Electronic Vaccine Intelligence Network | Tracks vaccine stock levels and cold chain temperatures in real time at all storage points |
| CoWIN | COVID Vaccine Intelligence Network | COVID-19 vaccination registration, appointments, certificates |
| U-WIN | Universal Immunisation WIN | Real-time tracking of every routine immunisation dose - birth to 19 years |
How U-WIN Works - Step by Step
For Beneficiaries (Parents/Guardians)
- Register on the U-WIN app or portal using a mobile number
- One mobile number can register up to 10 people covering:
- Pregnant women
- Infants (0-1 year)
- Children (1-7 years)
- Adolescents (7-19 years)
- Each beneficiary gets a unique health identifier - linked to their ABHA (Ayushman Bharat Health Account) or Child ABHA
- Receive appointment reminders via SMS for upcoming due vaccines
- After vaccination, a digital vaccination certificate is generated (like CoWIN certificate)
- Access vaccination history anytime from the app
For Healthcare Workers (ANMs, Vaccinators)
- Log in to U-WIN on their device (phone/tablet)
- System auto-generates the list of beneficiaries due for vaccination on that session day
- Worker marks each dose administered - child's record updated in real time
- Helps with community mobilisation (knowing who to chase up)
- Flags children who are overdue or have missed doses ("drop-outs")
- Works even in remote areas like Andaman & Nicobar islands
For Programme Supervisors / Government
- Real-time national dashboard showing coverage district by district
- Identifies zero-dose children (never vaccinated) and partial immunisation cases
- Tracks session performance - did the session happen? How many doses were given?
- Integrates with eVIN so vaccine availability at the facility is matched against demand
- Generates automatic reports for HMIS (Health Management Information System)
Key Features Summary
| Feature | Detail |
|---|---|
| Registration | Mobile number-based, up to 10 family members |
| Identifiers | ABHA + Child ABHA linkage |
| Reminders | Automated SMS for upcoming vaccine due dates |
| Certificates | Digital vaccination certificate per dose/beneficiary |
| Languages | 12 Indian languages |
| Healthcare worker tools | Beneficiary due-list generation, session management |
| Backend | Tracks drop-outs, zero-dose children, coverage gaps |
| Supply chain link | Integrated with eVIN for cold chain + stock monitoring |
| Scale (2024) | 130+ million registrations (30M+ pregnant women, 100M+ children), 500+ million doses tracked digitally |
Why U-WIN Matters
- Before U-WIN: Vaccine records were on paper cards (the yellow immunisation card), easily lost, no national database, no way to track missed children at scale
- After U-WIN: Every dose is logged centrally, missed children are flagged automatically, and parents get reminders - closing the gap between scheduled and actual immunisation
Any new updates and details of cold chain?
India UIP cold chain system eVIN updates 2024 2025 vaccine storage infrastructure
https://www.pib.gov.in/PressReleasePage.aspx?PRID=2241066
Vaccine Cold Chain - Complete Guide
What Is the Cold Chain?
Right vaccine → Right quantity → Right place → Right time → Right condition (no temperature breaks) → Right cost
India's Cold Chain Infrastructure (2026 Update)
| Parameter | Figure |
|---|---|
| Total cold chain points | ~30,000 |
| Ice-Lined Refrigerators (ILRs) + Deep Freezers | 1.06 lakh (1,06,000+) |
| Walk-in Coolers (WIC) + Walk-in Freezers (WIF) | 432 |
| Immunisation sessions conducted annually | 1.3 crore (13 million) |
| Span | National vaccine depots → Primary Health Centres |
Cold Chain Equipment - Classified
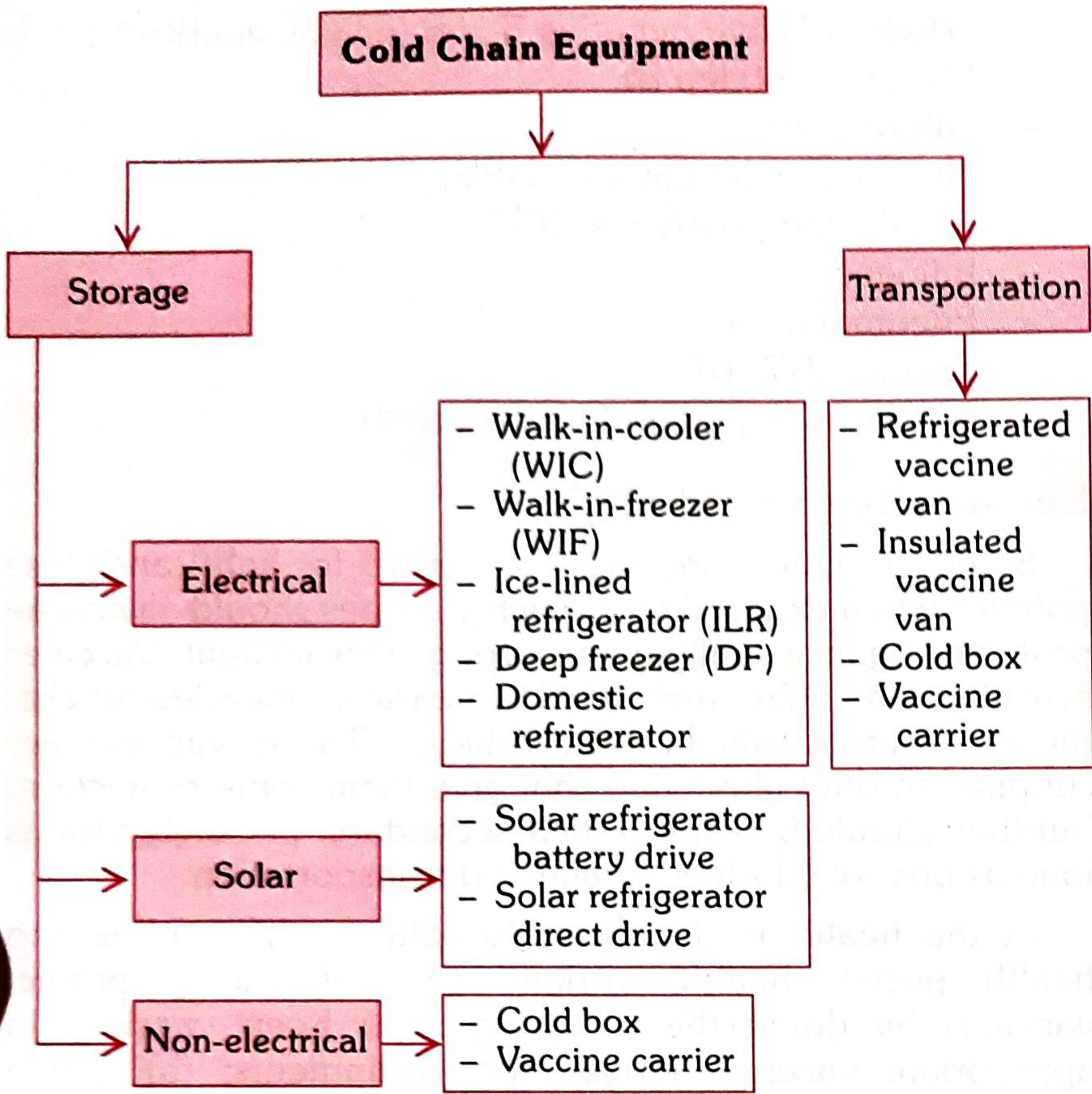
A. Storage Equipment
Electrical
| Equipment | Temp Range | Use / Level |
|---|---|---|
| Walk-in Freezer (WIF) | -15°C to -25°C | National/State/Regional stores; bulk OPV storage + ice pack preparation; has auto standby generator |
| Walk-in Cooler (WIC) | +2°C to +8°C | State/District; large quantity storage of all vaccines except OPV; sizes of 16.5, 32, 40 cubic meters |
| Ice-Lined Refrigerator (ILR) | +2°C to +8°C | District/PHC level; most important cold chain link; maintains temp even during 8-hour power cuts via ice bank lining |
| Deep Freezer (DF) | -15°C to -25°C | District/CHC level; OPV storage + freezing ice packs |
| Domestic Refrigerator | +2°C to +8°C | Sub-centre; limited use only |
Solar
| Equipment | How It Works |
|---|---|
| Solar Refrigerator (Battery Drive) | DC compressor charged by solar panels; two compartments: vaccine (+2 to +8°C) and freezer (up to -7°C) |
| Solar Refrigerator (Direct Drive) | Freezes a "phase change material" using solar energy; uses that ice bank to maintain cooling at night/cloudy days |
Non-electrical
- Cold boxes
- Vaccine carriers
B. Transportation Equipment
| Equipment | Use |
|---|---|
| Refrigerated Vaccine Van | Maintains temp during long-distance transport |
| Insulated Vaccine Van | Short-distance transport with ice packs |
| Cold Box | Carries 20-100 vials; maintains temp for 24+ hours with frozen ice packs; used for outreach/field sessions |
| Vaccine Carrier | Carries 16-20 vials; 4 frozen ice packs; for outreach sessions |
| Day Carrier | Carries 6-8 vials; 2 frozen ice packs; few hours use only for nearby sessions |
| Ice Packs | Filled with plain water (no salt); discarded if leaking |
Key rule: At sub-centre and village level, vaccines are NOT stored - they are supplied on the day of use only. Risk of cold chain failure is greatest at this level.
Temperature Sensitivity of Vaccines
Freeze-sensitive vaccines (must NOT go below 0°C)
- Pentavalent (DPT+HepB+Hib)
- Hepatitis B
- IPV (fIPV)
- PCV
- Rotavirus
- HPV
- Td / TT / DT
- Influenza, Cholera
Heat-sensitive vaccines (Groups A-F, most to least sensitive)
| Group | Vaccines |
|---|---|
| A (most sensitive) | OPV |
| B | Influenza |
| C | IPV, JE (freeze-dried), MR (freeze-dried) |
| D | Cholera, Pentavalent, Hib (liquid), Rotavirus, Rubella |
| E | BCG, HPV, JE, Td/TT |
| F (least sensitive) | Hepatitis B, Hib (freeze-dried), Pneumococcal |
Light-sensitive vaccines
ILR - The Most Important Cold Chain Link
- Operates on vapour compression (like a regular fridge)
- Has an ice-lined inner wall that maintains vaccine temperature for up to 8 hours during power cuts
- Basket-type design - vaccines stored in baskets, NOT against the walls
- Temperature must be checked and recorded twice daily (morning + end of session)
Open Vial Policy (OVP) - 2015
- Cold chain has been maintained (vaccine stored at +2°C to +8°C throughout)
- VVM (Vaccine Vial Monitor) has not passed the discard point
- Vial expiry date has not passed
- Vaccine septum has not been submerged in water
- No visible contamination or floating particles
Vaccine Vial Monitor (VVM)
- The inner square is lighter than the outer circle = safe to use
- Inner square same colour or darker = discard, do not use
- Helps field workers make real-time discard decisions without a thermometer
eVIN - Digital Cold Chain Monitoring (Latest Update)
- IoT temperature sensors on every storage unit
- Real-time alerts if temperature goes out of range
- Tracks vaccine stock levels at each cold chain point
- Central dashboard for supply chain managers
- Proved critical during COVID-19 rollout
- Now being exported as a model to other countries (Lao PDR, Zambia)
Handling During Immunisation Session
- Check vials at start of session; discard if VVM has passed
- Keep freeze-sensitive vaccines (Pentavalent, IPV, PCV, Hep B) away from direct contact with frozen ice packs - place a layer of foam/card between them
- OPV can be placed directly against ice packs (freeze-stable)
- Reconstituted vaccines (BCG, MR): discard after 4 hours or at end of session, whichever is earlier
- Multi-dose opened vials with preservatives: OVP applies (up to 28 days) if conditions met
New Updates (2025-2026)
- eVIN expanded nationwide - all States/UTs now covered with real-time temperature + stock monitoring
- U-WIN integration with eVIN - demand-side and supply-side now digitally linked for the first time
- Model Immunisation Centres launched in UP, Bihar, Chandigarh, and Ladakh - upgraded cold chain + digital infrastructure as pilot hubs
- HPV vaccine cold chain set up pan-India for the February 2026 campaign (HPV is freeze-sensitive, Group E)
- A-VIN (Animal Vaccine Intelligence Network) - same eVIN framework now piloted in two states for animal vaccines, showing scalability of the model
- Park's Textbook of Preventive and Social Medicine - "The Cold Chain," Cold Chain Equipment, Temperature Requirements sections (pp. 122-126)
- PIB India - Celebrating the Power of Vaccines, 2026
- UNDP India - A Decade of Digital Health, 2025
How to remember freeze sensitive and light sensitive vaccines and how to arrange them in a standard refrigerator, there is a mnemonic, I guess.
freeze sensitive vaccines mnemonic "DRIPT" OR "RIPT" cold chain refrigerator arrangement India UIP
freeze sensitive vaccines mnemonic "HRIPT" OR "DPT HepB TT" remember light sensitive BCG measles rubella
Freeze-Sensitive & Light-Sensitive Vaccines - Mnemonics + ILR Arrangement
1. FREEZE-SENSITIVE Vaccines
Mnemonic: "Don't Let The Poor Infants Freeze"
| Letter | Vaccine |
|---|---|
| Don't | DPT (Diphtheria-Pertussis-Tetanus) |
| Let | Liquid Pentavalent (DPT+HepB+Hib) |
| The | TT / Td (Tetanus Toxoid / Tetanus-Diphtheria) |
| Poor | PCV (Pneumococcal Conjugate Vaccine) |
| Infants | IPV / fIPV (Inactivated Polio Vaccine) |
| Freeze | HepB (Hepatitis B) |
DPT · Rotavirus · IPV · Pentavalent · TT/Td · HepB + PCV + HPV
2. LIGHT-SENSITIVE Vaccines
Mnemonic: "BCG Measles Rub the Rubella MMR"
| Vaccine | Why |
|---|---|
| BCG | Highly light-sensitive |
| Measles | Heat AND light sensitive |
| MR (Measles-Rubella) | Heat AND light sensitive |
| MMR | Light sensitive |
| Rubella | Light sensitive |
3. ILR (Ice-Lined Refrigerator) - Standard Arrangement
Official WHO/GOI Rule:
┌─────────────────────────────────────────┐
│ FREEZER COMPARTMENT (top) │ ← ICE PACKS only
├─────────────────────────────────────────┤
│ TOP BASKET → FREEZE-SENSITIVE │ ← HepB, Penta, DPT,
│ │ TT/Td, IPV, PCV, HPV
├─────────────────────────────────────────┤
│ BOTTOM BASKET → HEAT-SENSITIVE │ ← OPV, BCG, MR,
│ (freeze-stable) │ Measles, Rotavirus, JE
└─────────────────────────────────────────┘
Why this seems backwards (but makes perfect sense):
- The coldest zone in a top-opening ILR is the bottom - closest to the ice-lined walls
- Freeze-sensitive vaccines placed at top = farther from the ice = protected from freezing
- Heat-sensitive freeze-stable vaccines placed at bottom = benefit from coldest zone = more protection from heat
- Diluents go next to their corresponding freeze-dried vaccines (or on the bottom shelf if space is short)
Memory trick:
"FREEZE-sensitive = goes on TOP (away from ice)" "HEAT-sensitive = goes to BOTTOM (nearest ice)"
4. Additional ILR Rules (Dos and Don'ts)
| ✅ DO | ❌ DON'T |
|---|---|
| Check temperature twice daily (morning + end of session) | Don't store food or drinking water |
| Leave space between vaccine boxes for air circulation | Don't open ILR frequently |
| Place thermometer in basket between vaccines | Don't keep expired vaccines or VVM-passed vials |
| Condition frozen ice packs before placing near vaccines | Don't put unconditioned ice packs directly against freeze-sensitive vaccines |
| Store diluents at +2°C to +8°C at least 24 hrs before use | Don't disturb thermostat setting |
| FIFO - early expiry on top, later expiry below | Don't place heavy weight on ILR lid |
5. Quick Recap Table
| Property | Vaccines | Basket Position |
|---|---|---|
| Freeze-sensitive | DPT, Penta, TT/Td, PCV, IPV/fIPV, HepB, HPV, Rotavirus | TOP |
| Heat + Light sensitive | BCG, Measles, MR, MMR, Rubella | BOTTOM (dark vials, protect from light) |
| Most heat-sensitive | OPV (Group A) | BOTTOM |
| Never stored at sub-centre | All vaccines | Supplied on day of use only |