Suicidal and homicidal cutthroat injury difference
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative forensic medicine textbooks and clinical images. Here is a detailed, well-organized answer.
Suicidal vs. Homicidal Cutthroat Injury: Differences
Cutthroat injuries are incised wounds of the neck. Distinguishing their manner of death is one of the most important problems in forensic pathology.
Suicidal Cut-Throat
Image: Suicidal cut-throat with multiple incisions and hesitation marks

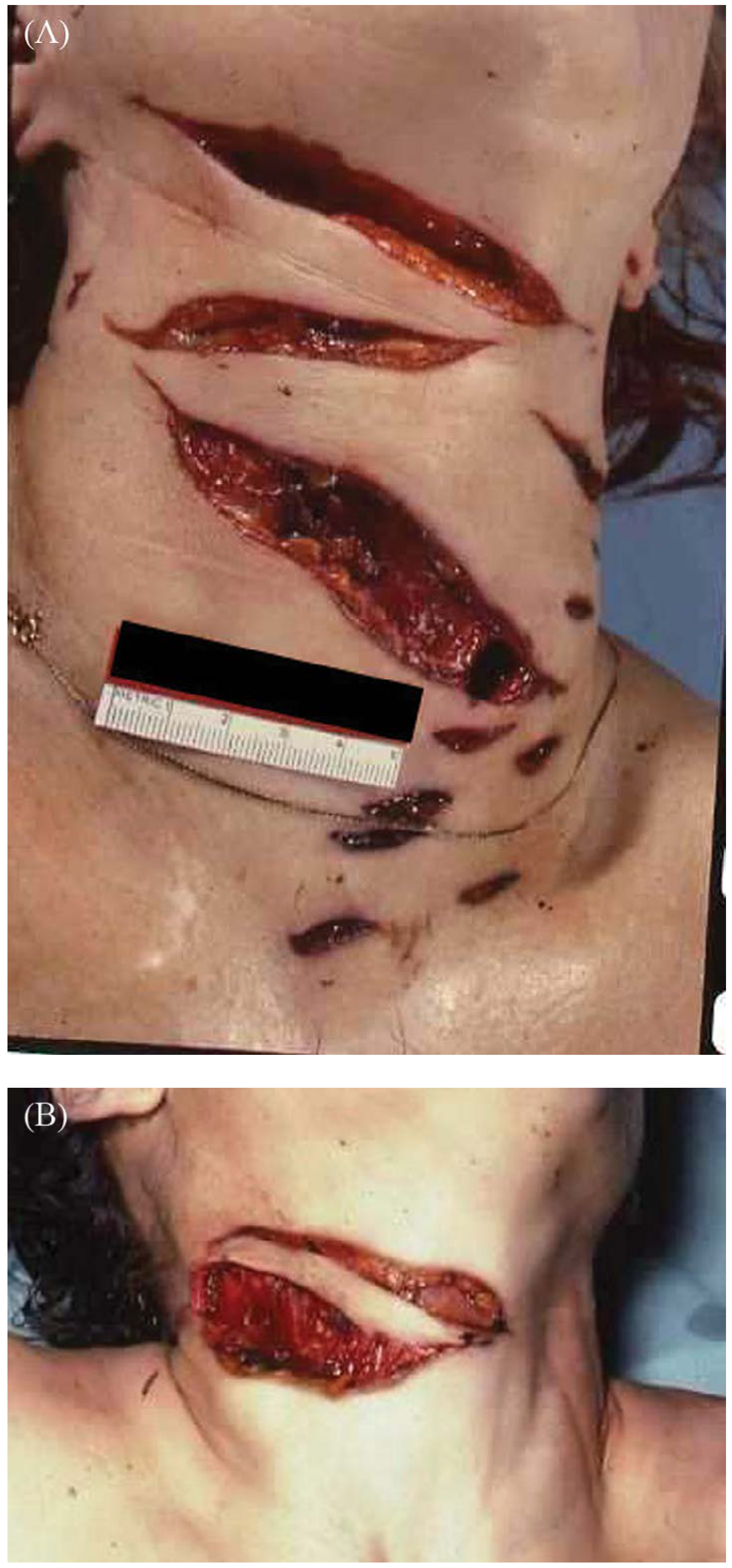
Homicidal Cut-Throat (inflicted from front)
Image: Homicidal incised wounds of the neck - short, slashing, deep wounds
Comprehensive Comparison Table
| Feature | Suicidal | Homicidal |
|---|---|---|
| Site / Situation | Left side of neck in right-handed person; passes across front of throat; rarely both sides | Usually on both sides of neck |
| Level | High - above thyroid cartilage | Low - on or below thyroid cartilage |
| Direction | Above downwards; left to right (right-handed). Sometimes horizontal | Transverse or from below upwards. If attacked from behind, may resemble suicidal wound |
| Number | Multiple (can be 20-30); superficial, parallel, merging with main wound; rarely single | Multiple but cross each other at a deep level; not repeated in depths of main wound |
| Edges | Usually ragged due to overlapping of multiple superficial incisions | Sharp and clean-cut; beveling may be present |
| Hesitation cuts | Present (in ~1/3 of cases) - superficial preliminary cuts above, below, or overlying the main wound | Absent (occasionally present if victim struggled or assailant hesitated) |
| Tailing | Present - wound tapers off on the right side in right-handed persons | Absent - boldly cut at commencement |
| Depth / Severity | Gradual deepening and shallowing; usually less severe overall; one wound may be very deep | More severe; all tissues including vertebrae may be cut; deep from the start |
| Vascular injury | Carotid artery usually escapes - head thrown back draws carotid beneath sternomastoid | Jugular veins and carotid artery likely to be cut |
| Defense wounds | Absent; unintentional cuts may appear on fingers if an open razor was used | Present - protective (defense) cuts on grasping surfaces of hands, wrinkled skin of palms, or back of forearms |
| Associated injuries | Often present: incised wounds on wrists, groins, thighs, ankles; healed scars from prior attempts | No wounds on wrists; but often severe injuries on head and neck |
| Weapon | Usually present; may be firmly grasped due to cadaveric spasm | Usually absent - removed by the murderer; cadaveric spasm not reported |
| Clothes | Not cut or damaged; victim may have opened collar to expose neck | May be cut corresponding to wounds on the body; disarrangement, torn buttons |
| Blood stain pattern | If standing: stains on front of body and clothes running downward; splashes on feet; mirror may show blood splashes | If victim was asleep: blood runs down sides of neck and collects behind neck/shoulders; stains on both palms (victim tried to cover wound) |
| Scene | Quiet, secluded place - bedroom or locked bathroom; often in front of a mirror; suicidal note may be found | Considerable disturbance at scene - disarranged furniture, trampled vegetation, confused footprints |
| Other wounds on body | Suicidal cuts on wrists, thighs, ankles (tentative cuts) | Severe injuries usually on head and neck; no wrist wounds |
Key Distinguishing Points to Remember
1. Hesitation (Tentative) Cuts
The most diagnostically useful feature of suicide. These are multiple, superficial, parallel cuts at the beginning of the main wound or adjacent to it. They represent the person's initial hesitancy before committing to the deeper, fatal incision. They are present in roughly one-third of suicidal cases. They can occasionally appear in homicide if the victim was struggling.
2. Tailing
In suicides, the wound starts deep on the left (in right-handed persons) and trails off to a shallower "tail" on the right. In homicide, the wound is boldly incised - no tailing.
3. Direction and Level
- Suicidal: high, above thyroid cartilage, sloping downward from left to right
- Homicidal: low, at or below thyroid cartilage, may slope upward
4. Vascular Sparing in Suicide
When a person commits suicide, they typically hyperextend the neck (chin up, head back). This moves the carotid bundle beneath the sternomastoid and against the spine - so the carotid artery is often spared. Death in many suicidal cutthroats results from hemorrhage from smaller vessels, injury to the larynx/trachea, or air embolism rather than carotid transection.
5. Defense Wounds
Firmly indicate homicide. Cuts on the palmar aspect of fingers and hands are from the victim grabbing the blade in self-defense.
6. Handedness Rule
In a right-handed person:
- Suicidal: wound originates high on the left side
- Homicidal (from behind, by right-handed assailant): knife drawn from left to right; wound starts below the left ear (opposite side from assailant's dominant hand)
7. Weapon at Scene
Weapon present = suggests suicide (especially if found in the hand due to cadaveric spasm). Weapon absent = suggests homicide (perpetrator removed it).
Cause of Death in Cut-Throat Wounds
Regardless of manner, death may result from:
- Hemorrhage (most common)
- Air embolism
- Asphyxia (blood aspiration into trachea)
- Injury to cervical vertebrae/spinal cord
Sources: The Essentials of Forensic Medicine and Toxicology, 36th ed. (2026), Table 8.7 | Parikh's Textbook of Medical Jurisprudence, Table 20.4 | PC Dikshit Textbook of Forensic Medicine | DiMaio's Forensic Pathology, 3rd ed., pp. 202-206
This is a shared conversation. Sign in to Orris to start your own chat.