Give me an info graphic on Clostridium difficile for MD Microbiology exam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Generating Image
Here's your C. diff infographic, sourced directly from Medical Microbiology 9e and Henry's Clinical Diagnosis and Management by Laboratory Methods. Here's a quick key-point summary for your exam:
High-Yield C. difficile Summary
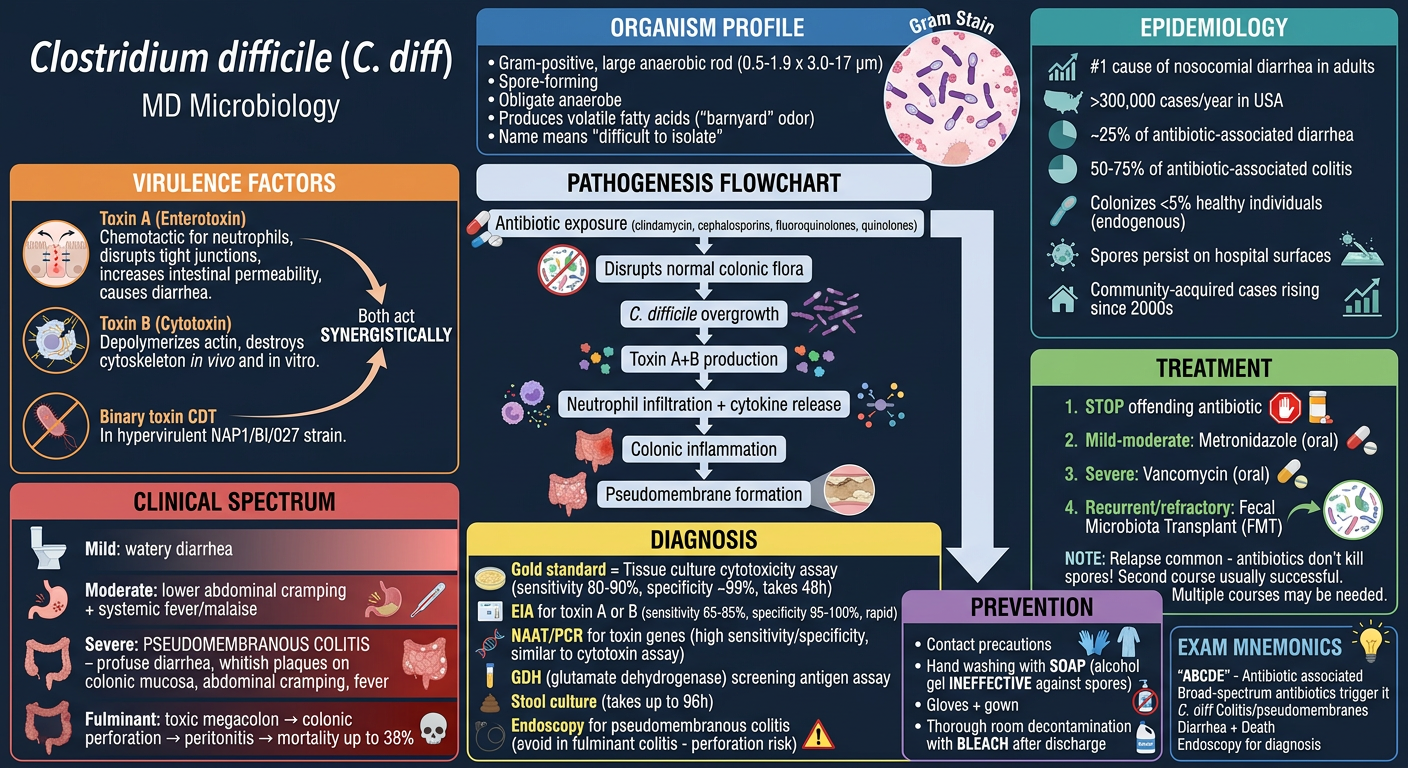
Organism: Large Gram-positive anaerobic rod, obligate spore-former, name = "difficile" (difficult to isolate due to extreme O2 sensitivity), produces volatile fatty acids ("barnyard" smell in culture).
Two Key Toxins (work synergistically):
- Toxin A (Enterotoxin) - attracts neutrophils, disrupts tight junctions, increases intestinal permeability → diarrhea
- Toxin B (Cytotoxin) - depolymerizes actin, destroys cytoskeleton in vivo and in vitro
Triggering Antibiotics (high-yield): Clindamycin, Cephalosporins, Fluoroquinolones/Quinolones (any broad-spectrum can do it)
Clinical Spectrum:
- Mild: self-limited watery diarrhea
- Severe: Pseudomembranous colitis - whitish plaques on colonic mucosa, profuse diarrhea, fever, cramping
- Fulminant: toxic megacolon → perforation → mortality up to 38%
Diagnosis:
| Test | Sensitivity | Specificity | Time |
|---|---|---|---|
| Tissue culture cytotoxin assay (gold std) | 80-90% | ~99% | 48h |
| EIA (toxin A/B) | 65-85% | 95-100% | Rapid |
| NAAT/PCR | High (similar to gold std) | High | Rapid |
| GDH antigen screen | Screening only | - | Rapid |
Treatment (in order):
- Stop the offending antibiotic
- Mild-moderate: Metronidazole (oral)
- Severe: Vancomycin (oral)
- Recurrent/refractory: Fecal Microbiota Transplant (FMT)
- Relapse is common - spores are NOT killed by antibiotics!
Prevention: Soap and water handwashing (alcohol-based hand rub is INEFFECTIVE against spores), bleach for surface decontamination, contact precautions.
Sources: Medical Microbiology 9e, p. 350; Henry's Clinical Diagnosis & Management by Laboratory Methods
Microbiology diagnosis
Asking for Preferences
Reading File
Reading File
Reading File
Generating Image
Here's your focused C. diff diagnosis infographic. Key exam points to memorize:
C. difficile Diagnosis - High-Yield Summary
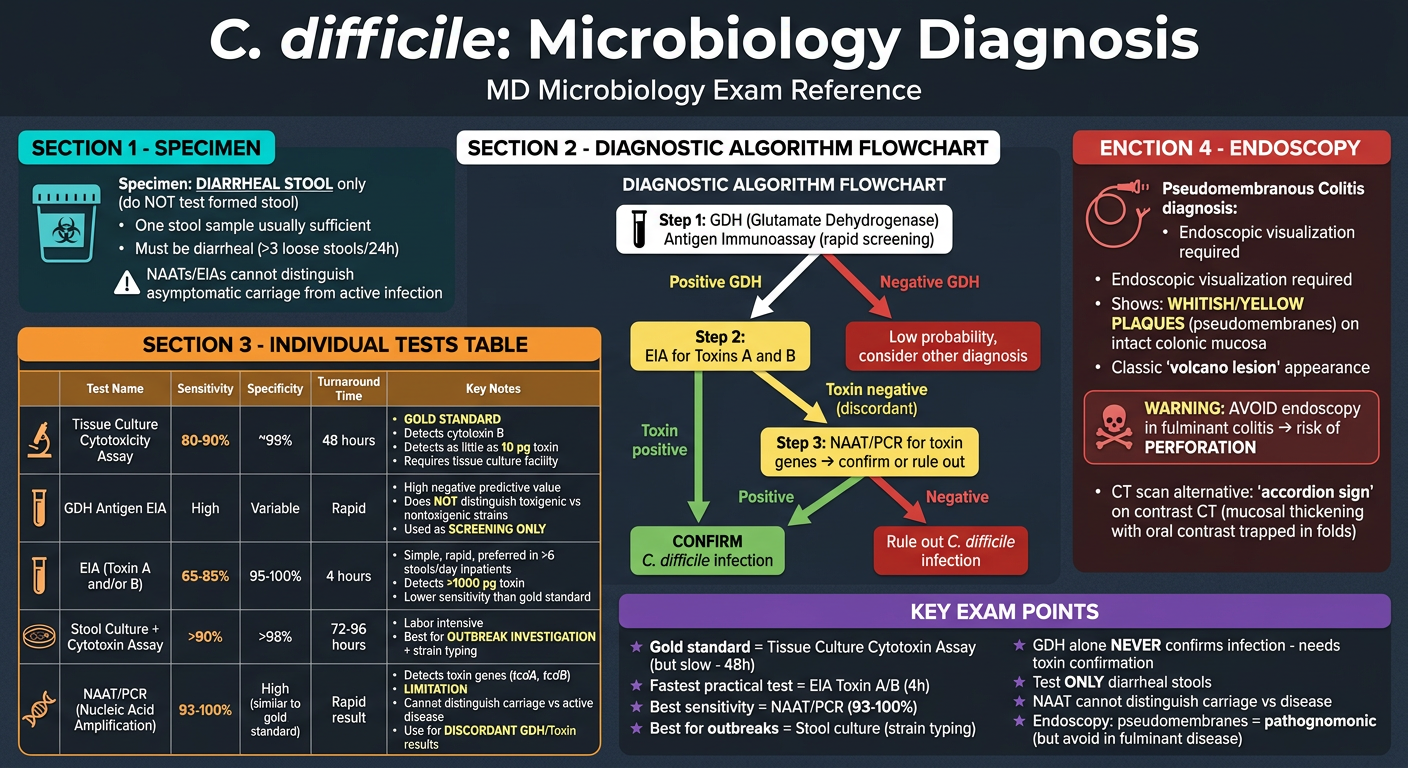
Specimen Rule: Only test diarrheal stool - never formed stool.
Diagnostic Tests at a Glance
| Test | Sensitivity | Specificity | Time | Role |
|---|---|---|---|---|
| Tissue culture cytotoxin assay | 80-90% | ~99% | 48h | Gold standard |
| EIA (Toxin A/B) | 65-85% | 95-100% | 4h | Rapid, practical |
| NAAT/PCR (toxin genes) | 93-100% | High | Rapid | Confirmatory |
| GDH antigen EIA | High NPV | - | Rapid | Screening only |
| Stool culture | >90% | >98% | 72-96h | Outbreak investigation |
Recommended Algorithm (3-step)
- Screen with GDH antigen EIA
- If positive GDH → confirm with Toxin A/B EIA
- If discordant → resolve with NAAT/PCR
Critical Limitations to Know
- NAAT/PCR - cannot distinguish asymptomatic carriage vs active disease
- GDH - cannot distinguish toxigenic vs non-toxigenic strains (always needs toxin confirmation)
- EIA - detects >1,000 pg of toxin; less sensitive than cytotoxin assay (detects as little as 10 pg)
Endoscopy
- Required for diagnosing pseudomembranous colitis directly
- Appearance: whitish/yellow plaques (pseudomembranes) on intact colonic mucosa
- AVOID in fulminant colitis - risk of perforation
- CT alternative: "accordion sign"
Sources: Henry's Clinical Diagnosis & Management by Laboratory Methods (Table 23.5); Medical Microbiology 9e
In same way explain Clostridium botulinum
Finding Sources
Reading File
Reading File
Reading File
Reading File
Generating Image
Generating Image
This is a shared conversation. Sign in to Orris to start your own chat.