What are the causes of acute kidney injury and outline of management of it
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute kidney injury"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full answer.
Acute Kidney Injury (AKI): Causes and Management
Definition
AKI is defined as an abrupt decline in glomerular filtration rate (GFR) sufficient to decrease elimination of nitrogenous waste products and uremic toxins. The KDIGO criteria define AKI as any of:
- Rise in serum creatinine ≥0.3 mg/dL within 48 hours
- Rise in serum creatinine ≥1.5x baseline within 7 days
- Urine output <0.5 mL/kg/hr for ≥6 hours
Categories of AKI
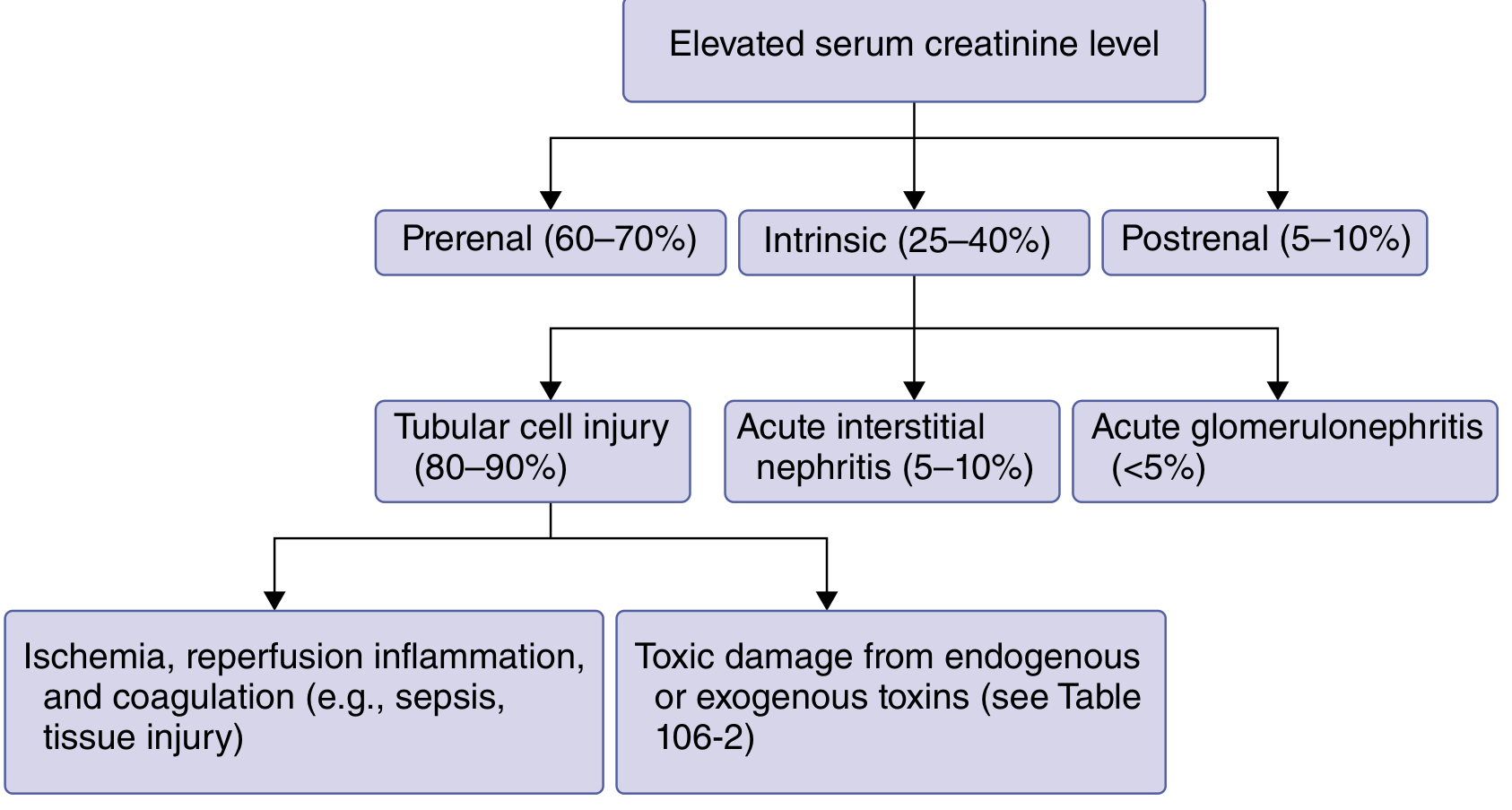
AKI is traditionally classified into Prerenal, Intrinsic (Renal), and Postrenal categories.
1. Prerenal AKI (60-70% of community-acquired cases)
Caused by reduced kidney perfusion with preserved tubular function. The kidney responds by maximally reabsorbing sodium and water.
Causes:
True volume depletion:
- Hemorrhage
- Vomiting, diarrhea
- Burns
- Inadequate oral intake
- Excessive diuresis
Effective volume depletion (reduced cardiac output/effective arterial volume):
- Heart failure
- Cirrhosis (portal hypertension, hypoalbuminemia)
- Nephrotic syndrome
- Sepsis (distributive shock)
Medications that reduce glomerular perfusion:
- NSAIDs - block afferent arteriolar vasodilation (prostaglandin-mediated)
- ACE inhibitors / ARBs - block efferent arteriolar vasoconstriction (angiotensin II-mediated)
- Calcineurin inhibitors (cyclosporine, tacrolimus)
- Radiocontrast agents
Key diagnostic clue: BUN:Creatinine ratio >20:1, FENa <1%, high urine osmolality (>500 mOsm/kg), low urine sodium (<20 mmol/L).
2. Intrinsic (Renal) AKI (25-40%)
Involves direct damage to kidney parenchyma. Subdivided by anatomic compartment:
A. Tubular Injury / Acute Tubular Necrosis (ATN) - 80-90% of intrinsic AKI
Ischemic/Hemodynamic (most common):
- Prolonged prerenal states progressing to tubular damage
- Sepsis - the single most common cause of ATN in ICU patients
- Post-cardiac surgery, aortic clamping, cardiopulmonary bypass
- Major hemorrhage or trauma
Nephrotoxic:
| Category | Agents |
|---|---|
| Antimicrobials | Aminoglycosides, amphotericin B, vancomycin, acyclovir, tenofovir, foscarnet |
| NSAIDs | Ibuprofen, naproxen, COX-2 inhibitors |
| Contrast agents | Radiocontrast dye (especially with pre-existing CKD, diabetes, volume depletion) |
| Chemotherapy | Cisplatin, methotrexate |
| Immunosuppressants | Cyclosporine, tacrolimus |
| Endogenous toxins | Myoglobin (rhabdomyolysis), hemoglobin (intravascular hemolysis) |
| Others | Cocaine, ethylene glycol, toluene, uric acid crystals (tumor lysis syndrome) |
Rhabdomyolysis causes:
- Muscle trauma, crush injuries, burns, electric shock
- Excessive exercise, seizures, heat exhaustion
- Pressure necrosis from prolonged immobility/coma
- Drugs: statins (especially with fibrates or cyclosporine), alcohol, cocaine, amphetamines
- Electrolyte disorders: hypophosphatemia, hypokalemia
- Infections, inflammatory myopathies
B. Acute Interstitial Nephritis (AIN) - 5-10% of intrinsic AKI
- Drug-induced (most common): beta-lactam antibiotics, NSAIDs, proton pump inhibitors, sulfonamides, rifampicin
- Infectious: Leptospirosis, hantavirus, EBV, CMV, pyelonephritis
- Autoimmune: Sjogren's syndrome, SLE, sarcoidosis
- Classic triad: fever, rash, eosinophilia (present in <30% of cases)
C. Acute Glomerulonephritis (<5% of intrinsic AKI)
- Rapidly progressive glomerulonephritis (RPGN)
- Systemic lupus nephritis
- Granulomatosis with polyangiitis (Wegener's) / polyarteritis nodosa
- Goodpasture syndrome (anti-GBM disease)
- IgA nephropathy
- Henoch-Schonlein purpura
- Post-infectious glomerulonephritis
D. Vascular Causes
Small vessel / microvascular:
- Thrombotic microangiopathy (TTP, HUS, HELLP syndrome)
- Malignant hypertension
- Scleroderma renal crisis
- DIC
- Eclampsia
Large vessel:
- Renal artery occlusion (thromboembolism in atrial fibrillation, aortic dissection)
- Renal vein thrombosis (nephrotic syndrome, hypercoagulable states)
- Cholesterol embolism after vascular procedures
3. Postrenal AKI (5-10%)
Caused by urinary tract obstruction at any level. GFR is initially preserved due to afferent arteriolar dilation, but prolonged obstruction causes vasoconstriction and permanent damage.
Causes by site:
Urethra/bladder outlet:
- Benign prostatic hyperplasia (most common in older men)
- Urethral stricture
- Functional (neurogenic bladder)
- Prostate/cervical/bladder cancer
Ureters (must be bilateral or obstruct a solitary kidney):
- Ureteric stones
- Retroperitoneal fibrosis
- Pelvic malignancy (colorectal, cervical, ovarian)
- Blood clots
FENa is ≥1% and BUN:Cr ratio is >20.
Management of AKI
Management follows a systematic approach based on the underlying category.
1. General Principles (All AKI)
- Optimization of hemodynamics: Volume resuscitation to correct intravascular depletion; target mean arterial pressure >65 mmHg. Use balanced crystalloids (Hartmann's/lactated Ringer's) rather than normal saline where possible. Avoid aggressive resuscitation in patients with heart failure or cirrhosis.
- Remove nephrotoxins: Discontinue NSAIDs, ACE inhibitors/ARBs, aminoglycosides, radiocontrast, calcineurin inhibitors where feasible.
- Nutrition: Provide 20-30 kcal/kg/day; use enteral route if oral intake is impossible. Avoid excessive protein restriction.
- Drug dose adjustment: Reduce doses and frequency of renally-cleared drugs; serum creatinine may underestimate GFR loss in AKI.
- Monitor input/output strictly, insert urinary catheter to measure urine output accurately.
2. Prerenal-Specific
- Prompt IV fluid resuscitation (isotonic crystalloid)
- Treat underlying cause (heart failure, sepsis, cirrhosis)
- Discontinue precipitating medications (NSAIDs, ACE inhibitors, ARBs)
- Hepatorenal syndrome: terlipressin (or norepinephrine) + IV albumin + octreotide/midodrine
3. Intrinsic Renal-Specific
ATN (ischemic/septic): No proven pharmacologic treatments. Supportive care; no role for low-dose dopamine, atrial natriuretic peptide, or erythropoietin (all failed in trials).
Rhabdomyolysis:
- Aggressive IV fluids (up to 10 L/day initially)
- Alkaline diuresis (75 mmol/L NaHCO3 in 0.45% saline) - promotes myoglobin excretion and prevents cast formation
- Loop diuretics if fluid-replete but urine output inadequate (target 200-300 mL/hr)
- Monitor calcium and phosphate carefully
Tumor lysis syndrome: Aggressive IV fluids + allopurinol (or rasburicase for severe hyperuricemia)
Contrast nephropathy prevention: Volume expansion with IV isotonic saline before and after procedure; minimize contrast volume; avoid concurrent nephrotoxins.
Glomerulonephritis/vasculitis: Immunosuppressive therapy (high-dose glucocorticoids ± cyclophosphamide); anti-complement therapy for atypical HUS; plasma exchange for TTP and Goodpasture syndrome.
Allergic AIN: Discontinue offending drug; empiric prednisone (1 mg/kg/day tapered over 1 month) if AKI persists.
Scleroderma renal crisis: ACE inhibitors.
4. Postrenal-Specific
- Prompt relief of obstruction is the priority:
- Bladder outlet: Insert urethral (or suprapubic) catheter
- Ureteric obstruction: Percutaneous nephrostomy tube or ureteral stent
- Post-obstructive diuresis: Monitor and replace fluids and electrolytes carefully after relief
5. Management of Metabolic Complications
| Complication | Treatment |
|---|---|
| Hyperkalemia | Restrict dietary K+; stop K+-sparing diuretics/ACE-I/ARBs/NSAIDs; loop diuretics; sodium zirconium cyclosilicate (Lokelma) or patiromer; insulin + glucose; inhaled beta-agonist; calcium gluconate 1g IV (cardiac stabilization) |
| Metabolic acidosis | NaHCO3 if pH <7.2 or HCO3 <15 mmol/L; dialysis for refractory cases |
| Volume overload | Salt and water restriction; loop diuretics (furosemide 40-80mg IV); ultrafiltration |
| Hyperphosphatemia | Dietary phosphate restriction; oral phosphate binders (calcium acetate, sevelamer, aluminum hydroxide) with meals |
| Hypocalcemia | Calcium carbonate or calcium gluconate if symptomatic |
| Hyponatremia | Restrict free water intake; minimize hypotonic IV fluids |
| Hypermagnesemia | Stop Mg2+-containing antacids/laxatives |
6. Renal Replacement Therapy (RRT / Dialysis)
Absolute indications (AEIOU mnemonic):
- Acidosis - severe metabolic acidosis refractory to medical treatment
- Electrolyte disorders - hyperkalemia unresponsive to medical therapy
- Ingestion of dialyzable toxins (methanol, ethylene glycol, lithium)
- Overload of volume - pulmonary edema refractory to diuretics
- Uremic symptoms - encephalopathy, pericarditis, bleeding, nausea/vomiting
Modalities:
- Intermittent hemodialysis (IHD) - preferred when hemodynamically stable
- Continuous RRT (CRRT) - preferred in hemodynamically unstable ICU patients
- Peritoneal dialysis - an alternative in low-resource settings
Timing of RRT: Current evidence (AKIKI, IDEAL-ICU trials) suggests watchful waiting until a definitive indication develops is at least as good as early initiation; late or watchful-waiting strategy avoids unnecessary RRT in patients who recover spontaneously.
Diagnostic Clues Summary
| Parameter | Prerenal | Intrinsic (ATN) | Postrenal |
|---|---|---|---|
| FENa | <1% | ≥1% | ≥1% (variable early) |
| BUN:Cr ratio | >20:1 | <10-15:1 | >20 (early) |
| Urine osmolality | >500 mOsm/kg | ~300 mOsm/kg (isosthenuria) | Variable |
| Urine sodium | <20 mmol/L | >40 mmol/L | Variable |
| Urinary sediment | Bland | Muddy brown granular casts | May show RBCs |
| Response to fluids | Rapid reversal | Persists | Reversal after relief |
Sources:
- Comprehensive Clinical Nephrology, 7th Edition, Ch. 70 (Paine, Jefferson, Velez)
- Goldman-Cecil Medicine International Edition, Ch. 106 (Acute Kidney Injury)
- Harrison's Principles of Internal Medicine, 22nd Edition, Table 321-3
- Brenner and Rector's The Kidney, 2-Volume Set, Ch. 72 (Prevention and Management of AKI)
This is a shared conversation. Sign in to Orris to start your own chat.