Tomorrow is my orthopedics posting and i Dont about anything about this please help me so that i will have all the knowlege about orthopedics history taking and focus more on examination part in easy language and provide all the necessary concepts reqiured for orthopedics history taking in easy langue and if possible provide me figure also
Reading File
Finding Sources
Finding Sources
Searching the Web
orthopedics history taking clinical examination guide medical students easy
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading Web Page
https://medicine.buffalo.edu/departments/ortho/education/med…
Loading Image
Searching the Web
orthopedic examination look feel move diagram GALS gait spine upper limb lower limb
Loading Image
Loading Image
I now have all the material needed. Let me write the complete, easy-language orthopedics guide.
🦴 Complete Orthopedics Posting Guide
History Taking + Clinical Examination (Easy Language)
Sources: Miller's Review of Orthopaedics 9th Ed, Campbell's Operative Orthopaedics 15th Ed, Slideshare Ortho History Guide
🔑 Golden Rule of Ortho Posting
Every orthopaedic diagnosis is made by 3 things:
- History - what the patient tells you
- Examination - what you find with your hands and eyes
- Investigations - X-ray, MRI, blood tests
PART 1: HISTORY TAKING
Think of ortho history in 7 steps - use the mnemonic "PC-PADS-F"
1. Personal Details (Always Ask First!)
| Detail | Why It Matters |
|---|---|
| Name, age, sex | Age tells you what diseases are common |
| Occupation | Manual labour = repetitive injuries, office job = back/neck issues |
| Dominant hand | Important for upper limb injuries |
| Address | TB is common in overcrowded areas |
🔥 Age is a SUPERPOWER in Ortho - Memorize This!
| Age | Think of... |
|---|---|
| < 1 year | DDH (Developmental Dysplasia of Hip), Cerebral Palsy |
| 1-2 years | Rickets, Polio |
| 5-10 years | TB of hip, Perthes disease |
| < 15 years | Acute osteomyelitis, Juvenile Idiopathic Arthritis |
| 15-20 years | SCFE (Slipped Capital Femoral Epiphysis) |
| 10-20 years | Bone tumours (Osteosarcoma, Ewing's sarcoma) |
| 30-40 years | Rheumatoid Arthritis |
| > 40 years | Osteoarthritis, AVN (Avascular Necrosis), Degenerative disorders |
| Elderly women | Osteoporosis + fractures |
2. Chief Complaint (CC)
Ask: "What is your main problem?"
The 8 common ortho complaints are:
P - Pain
S - Swelling
D - Deformity
S - Stiffness
W - Weakness / Wasting
I - Instability ("my joint gives way")
N - Numbness / Tingling
L - Limp / Loss of function
Write them in order they appeared (e.g., "Pain in right knee for 3 months, followed by swelling for 1 month").
3. History of Presenting Illness (HPI) - The MOST IMPORTANT PART
For every complaint, ask these questions. Use "SOCRATES" for pain:
| Letter | Question | Example answer |
|---|---|---|
| S - Site | Where exactly is the pain? | "Right knee, inner side" |
| O - Onset | Sudden or gradual? | "Gradual, over months" |
| C - Character | What type of pain? | Dull ache / sharp / burning / throbbing |
| R - Radiation | Does it go anywhere? | "Goes down to the calf" |
| A - Associated | Anything else with it? | Fever, swelling, stiffness |
| T - Timing | Constant or comes and goes? | "Worse in morning, better after walking" |
| E - Exacerbating/Relieving | What makes it better/worse? | "Worse on stairs, better with rest" |
| S - Severity | Out of 10? | "7/10 at rest" |
🎯 Special Pain Analysis for Ortho (VERY IMPORTANT)
Morning stiffness > 1 hour = Inflammatory arthritis (Rheumatoid)
Pain worse after rest, better on movement = Inflammatory
Pain worse after activity, better on rest = Mechanical (Osteoarthritis)
Night pain / pain waking from sleep = Malignancy, infection, or inflammatory
Constant pain + fever + weight loss = Think Tumour or Infection (TB, Osteomyelitis)
🎯 For Swelling - Ask:
- Sudden onset after trauma? = Haemarthrosis (blood in joint) = ligament tear, fracture
- Gradual swelling? = Synovitis, OA effusion
- Painful or painless? Painless rapidly growing swelling = tumour until proven otherwise
🎯 For Deformity - Ask:
- Was it there since birth? = Congenital
- Developed after injury? = Fracture/dislocation
- Gradual progressive deformity? = Arthritis, rickets
🎯 For Stiffness - Ask:
- Which joint? Morning or evening?
- Are there any clicking sounds?
🎯 For Instability - Ask:
- Does the joint "give way"? When? On which movement?
- E.g., knee giving way going down stairs = ACL tear
4. Past Medical History (PMH)
Ask about:
- Previous fractures or surgeries (especially ortho-related)
- TB (very relevant in India - can affect spine, hip, knee)
- Diabetes - poor wound healing, neuropathy, foot ulcers
- Hypertension, heart disease - affects anaesthesia risk
- Steroid use - causes AVN (avascular necrosis) of femoral head
- Cancer history - metastasis to bone causes pathological fractures
- Any previous joint problems
5. Drug History
Ask about:
- Steroids (long-term use causes osteoporosis + AVN)
- Methotrexate, immunosuppressants (for RA)
- NSAIDs - are they taking them already?
- Anticoagulants (warfarin, aspirin) - affects surgery
- Antibiotics - suggests ongoing infection
6. Family History
- RA, Ankylosing spondylitis - run in families
- Sickle cell disease - causes AVN and bone crises
- Gout - can be familial
- Achondroplasia, dwarfism - genetic
7. Social History
- Smoking - impairs bone healing, increases fracture risk
- Alcohol - AVN of femoral head, neuropathy, falls
- Occupation - heavy labour, computer work, sports
- Activities of daily living - can the patient manage at home? Can they climb stairs?
- Walking aids - do they use a stick, crutches, wheelchair?
- Support at home - who helps them?
PART 2: CLINICAL EXAMINATION
The Ortho Examination Framework: "LOOK - FEEL - MOVE"
Plus two extra steps: Neurovascular exam + Special tests
LOOK (Inspection)
FEEL (Palpation)
MOVE (ROM - Range of Motion)
NEURO (Neurological exam)
VASCULAR (Circulation)
SPECIAL TESTS (for each joint)
Always start from the general - then go local!
GENERAL EXAMINATION (Before touching the joint)
As the patient walks in, observe:
- Build and nutrition
- Pallor, cyanosis, jaundice
- Any obvious deformity
- Attitude of the limb (how they're holding it)
- Gait - watch how they walk!
🚶 GAIT ANALYSIS (Very Important - Examiners Love This!)
The normal gait cycle has two phases:
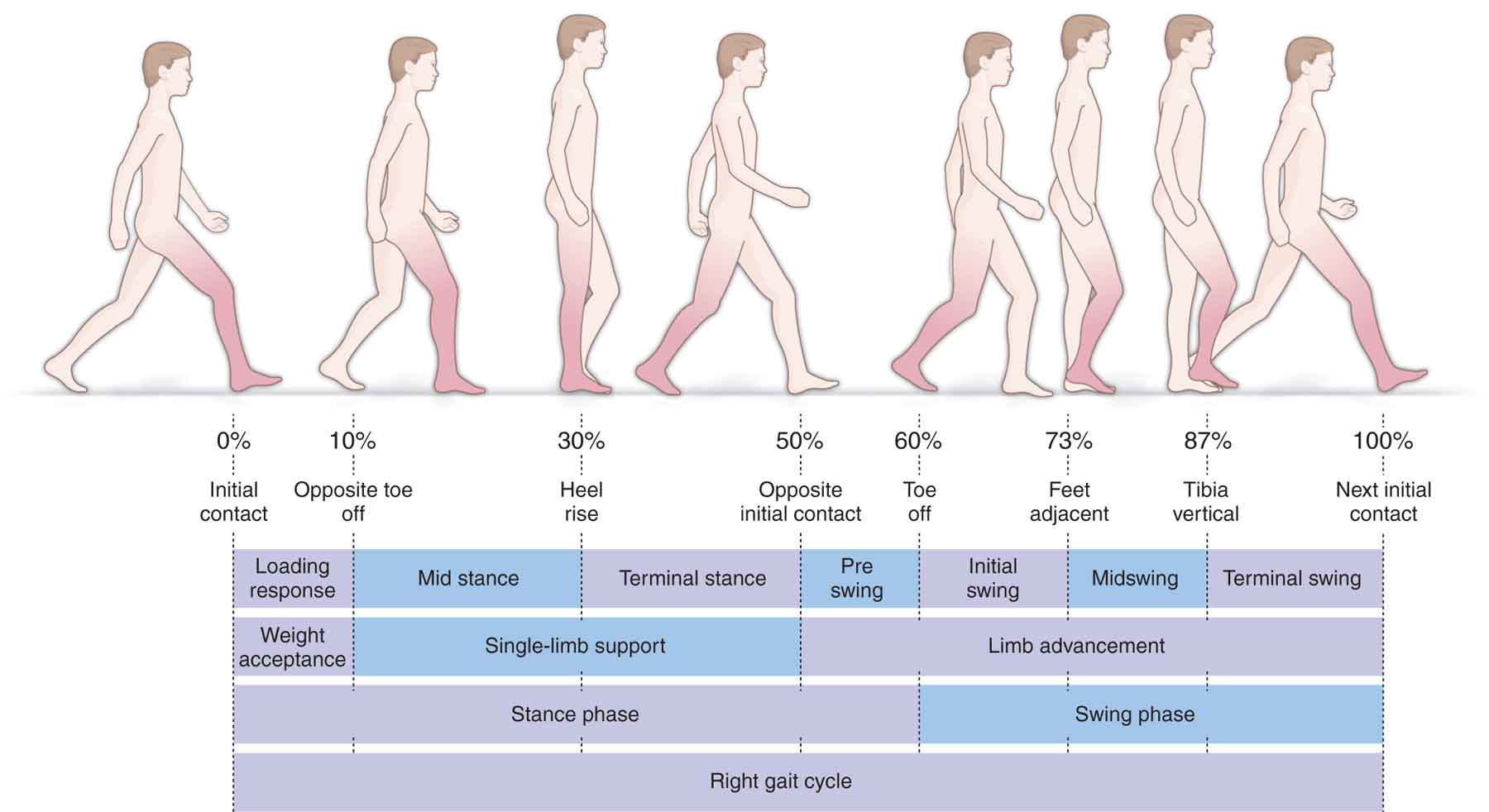
| Phase | What happens |
|---|---|
| Stance phase (60%) | Foot is on the ground |
| Swing phase (40%) | Foot is in the air |
Common Abnormal Gaits in Ortho:
| Gait Name | How It Looks | Cause |
|---|---|---|
| Trendelenburg gait (Waddling gait) | Patient leans to affected side when walking | Weak hip abductors (CDH, coxa vara, polio of glutei) |
| Antalgic gait | Short stance phase on painful side (limps quickly off painful leg) | Any painful condition of hip/knee/foot |
| Scissors gait | Legs cross while walking, narrow base | Cerebral palsy (spastic diplegia) |
| Steppage gait | High-stepping, foot drop | Common peroneal nerve palsy, L4-L5 disc |
| Spastic gait | Stiff-legged, circumduction of leg | UMN lesion (stroke, cord injury) |
| Short limb gait | Dipping/bobbing | True or apparent leg length discrepancy |
| Swaying gait | Trunk sway, wide base | Cerebellar lesion |
Tip: Trendelenburg test = Ask patient to stand on one leg. If the opposite hip drops = positive = weak abductors on the standing side.
LOOK (Inspection) - 3 Things to Inspect
A) Skin
| Look for | Meaning |
|---|---|
| Redness | Inflammation, infection |
| Bluish discolouration | Bruising / recent trauma |
| Pallor | Ischaemia |
| Blackening | Gangrene / necrosis |
| Scars | Previous surgery |
| Sinuses / discharging wounds | TB, chronic osteomyelitis |
| Skin creases | Loss of creases = swelling; asymmetric creases = DDH |
| Loss of hair | Peripheral vascular disease |
B) Shape of Limb / Swelling
- Localised swelling = specific structure (bursa, cyst, tumour)
- Diffuse swelling = joint effusion, gross injury
- Wasting/atrophy of muscles = disuse or nerve damage
C) Deformity
Types of deformity - you MUST know these!
| Term | Meaning | Example |
|---|---|---|
| Valgus | Distal part points AWAY from midline | Knock-knee (genu valgum) |
| Varus | Distal part points TOWARD midline | Bow-legs (genu varum) |
| Flexion deformity | Joint stuck in flexion, can't straighten | Fixed flexion deformity of knee in OA |
| Hyperextension | Joint bends backward more than normal | Genu recurvatum |
| Rotational deformity | Limb twisted | Fracture malunion |
| Shortening | Limb appears shorter | Fracture, DDH |
| Kyphosis | Forward bending of spine | TB spine, old age |
| Scoliosis | Lateral curvature of spine | Idiopathic, polio |
| Lordosis | Excessive inward curve | Lumbar region, bilateral hip flexion |
FEEL (Palpation) - Systematic
Start with: Temperature
- Use the back of your hand
- Compare both sides
- Warm = inflammation/infection
- Cold = ischaemia
Then Palpate:
1. Tenderness
- Point tenderness = fracture (press with one finger - if exact spot hurts = likely fracture)
- Diffuse tenderness = joint inflammation
2. Swelling - 3 Types
| Type | How to check | What it means |
|---|---|---|
| Bony hard | Like pressing bone | Callus, exostosis, tumour |
| Firm/rubbery | Feels like pressing a rubber ball | Fibrous tissue, ganglion |
| Soft/fluctuant | Fluid inside - press one side, other side rises | Effusion, abscess, cyst |
| Crepitus | Grinding felt on movement | OA (bone on bone) |
Special effusion tests for knee:
- Patellar tap test - fluid > 15-20 ml (press on patella - it bounces back)
- Bulge sign / Stroke test - small effusions < 15 ml (wipe fluid from medial side, tap lateral side - see medial bulge)
3. Muscle bulk and tone
- Compare both sides
- Wasting suggests disuse atrophy or nerve palsy
MOVE (Range of Motion)
Two types of movement:
| Type | What it is | Why we check both |
|---|---|---|
| Active ROM | Patient moves the joint themselves | Tests muscle strength + pain |
| Passive ROM | YOU move the joint for the patient | Tests the joint itself |
If active < passive = muscle/tendon problem
If both are equally reduced = joint problem (arthritis, stiffness)
Normal ROM Values (Know These!)
| Joint | Movement | Normal Range |
|---|---|---|
| Shoulder | Flexion | 0-180° |
| Abduction | 0-180° | |
| ER/IR | 90°/90° | |
| Elbow | Flexion | 0-145° |
| Supination/Pronation | 90°/90° | |
| Wrist | Flexion | 80° |
| Extension | 70° | |
| Hip | Flexion | 0-120° |
| Abduction | 45° | |
| IR/ER | 45°/45° | |
| Knee | Flexion | 0-135° |
| Extension | 0° (some have 10° hyperextension) | |
| Ankle | Dorsiflexion | 20° |
| Plantarflexion | 50° |
Describe Movements as:
- Full and painless (normal)
- Limited but painless (stiffness without inflammation)
- Full but painful (mild inflammation)
- Limited AND painful (arthritis, infection, serious pathology)
NEUROVASCULAR EXAMINATION (Always Do This After Move)
This is critically important in trauma cases!
Vascular Check:
- Peripheral pulses (radial, ulnar, popliteal, dorsalis pedis, posterior tibial)
- Capillary refill time - press nail for 2 seconds, should pink up < 2 seconds
- Skin temperature and colour
- Compartment syndrome warning: 5 Ps = Pain out of proportion, Pallor, Pulselessness, Paraesthesia, Paralysis
Neurological Check:
- Motor - test key muscle groups (MRC grading 0-5)
- Sensory - test dermatomes with light touch/pin prick
- Reflexes - DTRs (knee jerk = L3/4, ankle jerk = S1, biceps = C5/6, triceps = C7)
MRC Muscle Power Grading:
| Grade | Meaning |
|---|---|
| 0 | No movement |
| 1 | Flicker of movement |
| 2 | Movement with gravity eliminated |
| 3 | Movement against gravity |
| 4 | Movement against some resistance |
| 5 | Normal power |
MEASUREMENTS - LEG LENGTH DISCREPANCY
Very important in ortho - examiners always ask!
Two types:
1. True leg length (anatomical shortening)
- Measure from Anterior Superior Iliac Spine (ASIS) to medial malleolus
- Short = fracture, DDH, AVN, post-surgery
2. Apparent leg length (due to pelvic tilt or adduction deformity)
- Measure from umbilicus / xiphisternum to medial malleolus
- True length will be equal but apparent length differs
Rule: If apparent ≠ true = there is a pelvic/spinal tilt or a deformity at the hip
Causes of True Shortening:
| Type | Site | Cause |
|---|---|---|
| Bony | Above trochanter (Telescoping) | Fracture neck femur, CDH |
| Bony | Below trochanter | Femur/tibia shaft fractures |
| Apparent | Pelvic tilt | Hip adduction contracture |
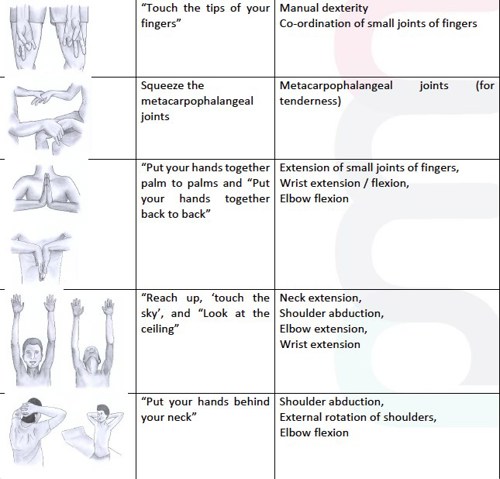
GALS SCREENING EXAMINATION (Quick 2-minute Ortho Screen)
The GALS exam is a rapid screening tool for any patient with joint complaints.
Ask 3 screening questions first:
- "Do you have any pain or stiffness in your muscles, joints, or back?"
- "Can you dress yourself without any difficulty?"
- "Can you walk up and down stairs without any difficulty?"
Then examine: Gait, Arms, Legs, Spine
SPECIAL TESTS BY REGION (Quick Reference)
🦴 SPINE
| Test | How | Positive Means |
|---|---|---|
| SLR (Straight Leg Raise) | Lift leg with knee straight, pain radiating below knee < 70° is positive | L4-S1 disc prolapse / nerve root compression |
| Femoral stretch test | Patient prone, flex knee - pain in front of thigh | L2-L4 nerve root compression |
| Schober's test | Mark 10 cm above and 5 cm below S2 dimples; normal = distance increases >5cm on flexion | Limited spinal flexion (Ankylosing Spondylitis) |
🦵 HIP
| Test | Positive Means |
|---|---|
| Trendelenburg test | Weak hip abductors |
| FABER / Patrick's test (Flexion-ABduction-External Rotation) | Hip or SI joint pathology |
| Thomas test (eliminate lumbar lordosis, extend hip) | Fixed flexion deformity of hip |
| Telescoping test | CDH (congenital dislocation of hip) |
🦵 KNEE
| Test | Positive Means |
|---|---|
| Anterior Drawer / Lachman test | ACL tear |
| Posterior Drawer test | PCL tear |
| McMurray's test (rotation + flex/extend) | Meniscus tear |
| Valgus stress test | MCL (medial collateral ligament) tear |
| Varus stress test | LCL (lateral collateral ligament) tear |
| Patellar apprehension test | Patellar subluxation/dislocation tendency |
💪 SHOULDER
| Test | Positive Means |
|---|---|
| Impingement sign (Neer) | Subacromial impingement |
| Hawkins test | Subacromial impingement |
| Jobe (empty can) test | Supraspinatus tear |
| Drop arm test | Rotator cuff tear |
| Apprehension test | Anterior shoulder instability |
| Speed's test | Biceps tendon / SLAP lesion |
🖐 HAND/WRIST
| Test | Positive Means |
|---|---|
| Tinel's sign (tap over carpal tunnel) | Carpal tunnel syndrome (CTS) |
| Phalen's test (wrist flexion 60 sec) | CTS |
| Finkelstein's test (thumb in fist, ulnar deviate) | De Quervain's tenosynovitis |
| Froment's sign | Ulnar nerve palsy |
| Allen's test | Radial or ulnar artery occlusion |
INVESTIGATIONS TO KNOW
| Investigation | Used For |
|---|---|
| X-ray | First line for all bone/joint problems (AP + Lateral views) |
| MRI | Soft tissues (ligaments, tendons, cartilage, disc prolapse, tumours) |
| CT scan | Complex fractures, bony anatomy detail |
| Bone scan (technetium) | Stress fractures, osteomyelitis, metastasis |
| Ultrasound | Soft tissue swellings, rotator cuff tendons |
| ESR, CRP | Infection, inflammation (RA, osteomyelitis, TB) |
| Serum uric acid | Gout |
| Rheumatoid Factor, Anti-CCP | Rheumatoid Arthritis |
| Mantoux, ADA | TB of bone/joint |
| Biopsy | Tumours (to confirm malignancy) |
🔴 RED FLAGS IN ORTHO - NEVER MISS THESE!
These suggest serious pathology (infection, cancer, neurology):
- Unremitting night pain (malignancy)
- Fever + bone/joint pain (osteomyelitis, septic arthritis)
- Constitutional symptoms (weight loss, night sweats, anorexia) with bone pain = tumour or TB
- Rapidly growing painless swelling = sarcoma until proven otherwise
- Cauda equina symptoms (saddle anaesthesia + bladder/bowel dysfunction) = SURGICAL EMERGENCY
- Bilateral neurological symptoms with spine pathology = cord compression
- Pulseless cold limb after trauma = vascular emergency
🩺 QUICK REVISION SUMMARY - ORTHO CLERKING FORMAT
When you approach a patient tomorrow, use this format:
1. Greet and introduce yourself
2. PC: "What brought you here today?" (pain, swelling, deformity, stiffness)
3. HPI: SOCRATES for pain + specific ortho questions
4. Age-related differential diagnosis in mind
5. PMH: TB, DM, steroids, cancer, previous fractures
6. Drug Hx: steroids, NSAIDs, anticoagulants
7. Family Hx: RA, gout, sickle cell
8. Social Hx: occupation, smoking, alcohol, mobility
9. EXAMINATION:
- General: build, pallor, gait (Trendelenburg? Antalgic?)
- Local LOOK: skin changes, deformity, swelling, wasting
- Local FEEL: temperature, tenderness (point vs diffuse), swelling type
- Local MOVE: Active then Passive ROM in degrees
- Measurements: leg length if lower limb
- Neurovascular: pulses, capillary refill, sensation, power, reflexes
- Special tests: relevant to the joint
10. Summarise findings and suggest investigations
🧠 MNEMONICS TO REMEMBER
| Mnemonic | Stands For |
|---|---|
| SOCRATES | Site, Onset, Character, Radiation, Associated symptoms, Timing, Exacerbating/relieving, Severity |
| LFM + NV + ST | Look, Feel, Move, Neuro, Vascular, Special Tests |
| 5 Ps of compartment syndrome | Pain, Pallor, Pulselessness, Paraesthesia, Paralysis |
| GALS | Gait, Arms, Legs, Spine (quick screening) |
| FABER | Flexion, ABduction, External Rotation (hip test) |
Good luck tomorrow! Focus on watching the patient walk in (gait), doing a proper LOOK-FEEL-MOVE, and never forgetting the neurovascular check after any trauma. Your examiner will be most impressed if you do these things systematically without being prompted.
- Miller's Review of Orthopaedics 9th Ed | Campbell's Operative Orthopaedics 15th Ed 2026
This is a shared conversation. Sign in to Orris to start your own chat.