Shoulder joint anatomy
Reading File
Finding Sources
Searching Images
shoulder joint anatomy glenohumeral
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive textbook content and excellent diagrams. Here is the complete shoulder joint anatomy review:
Shoulder Joint Anatomy
The shoulder (glenohumeral) joint is the most mobile joint in the human body and simultaneously the most susceptible to dislocation. Approximately 45% of all joint dislocations involve the shoulder. Its wide range of motion comes at the cost of inherent bony instability, compensated by the rotator cuff, labrum, and capsulolimgentous structures.
1. Bony Anatomy
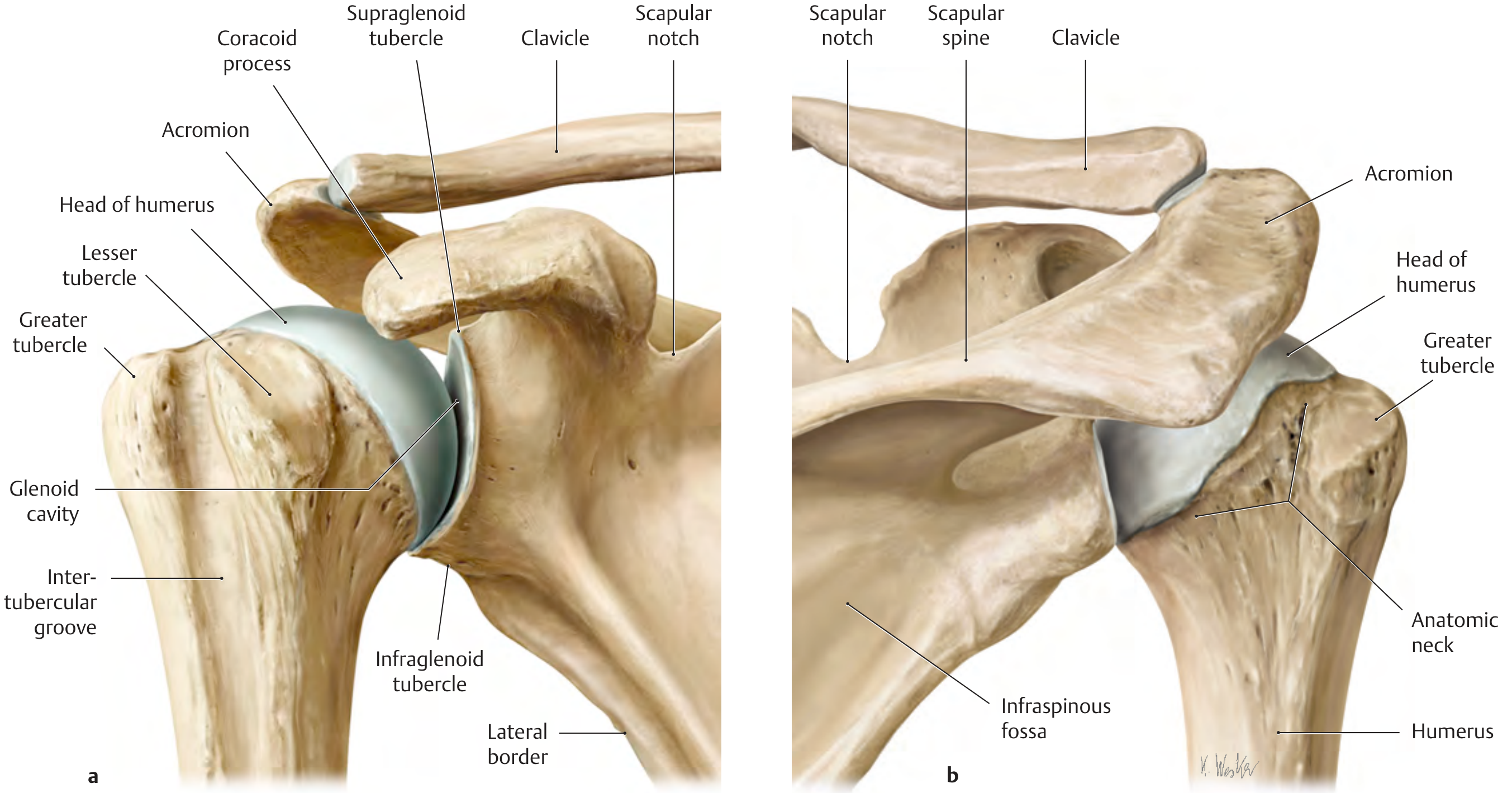
The glenohumeral joint is a spheroidal (ball-and-socket) joint formed by:
- Head of humerus — large, rounded, covered by hyaline cartilage
- Glenoid cavity of the scapula — shallow, pear-shaped fossa; its articular surface is 3–4× smaller than the humeral head
Key humeral landmarks:
| Structure | Significance |
|---|---|
| Greater tubercle | Attachment of supraspinatus, infraspinatus, teres minor |
| Lesser tubercle | Attachment of subscapularis |
| Intertubercular (bicipital) groove | Houses long head of biceps tendon |
| Anatomic neck | Attachment of joint capsule |
| Surgical neck | Common fracture site; at risk for axillary nerve injury |
2. Glenoid Labrum
The glenoid labrum is a fibrocartilaginous rim (~5 mm wide at its base) that deepens the shallow glenoid cavity. It:
- Increases contact area between articulating surfaces
- Serves as the attachment for the glenohumeral ligaments and long head of biceps
- Is torn in the Bankart lesion (anteroinferior avulsion during anterior dislocation)
3. Joint Capsule & Ligaments
The capsule is loose and thin posteriorly; anteriorly it is reinforced by the glenohumeral ligaments.
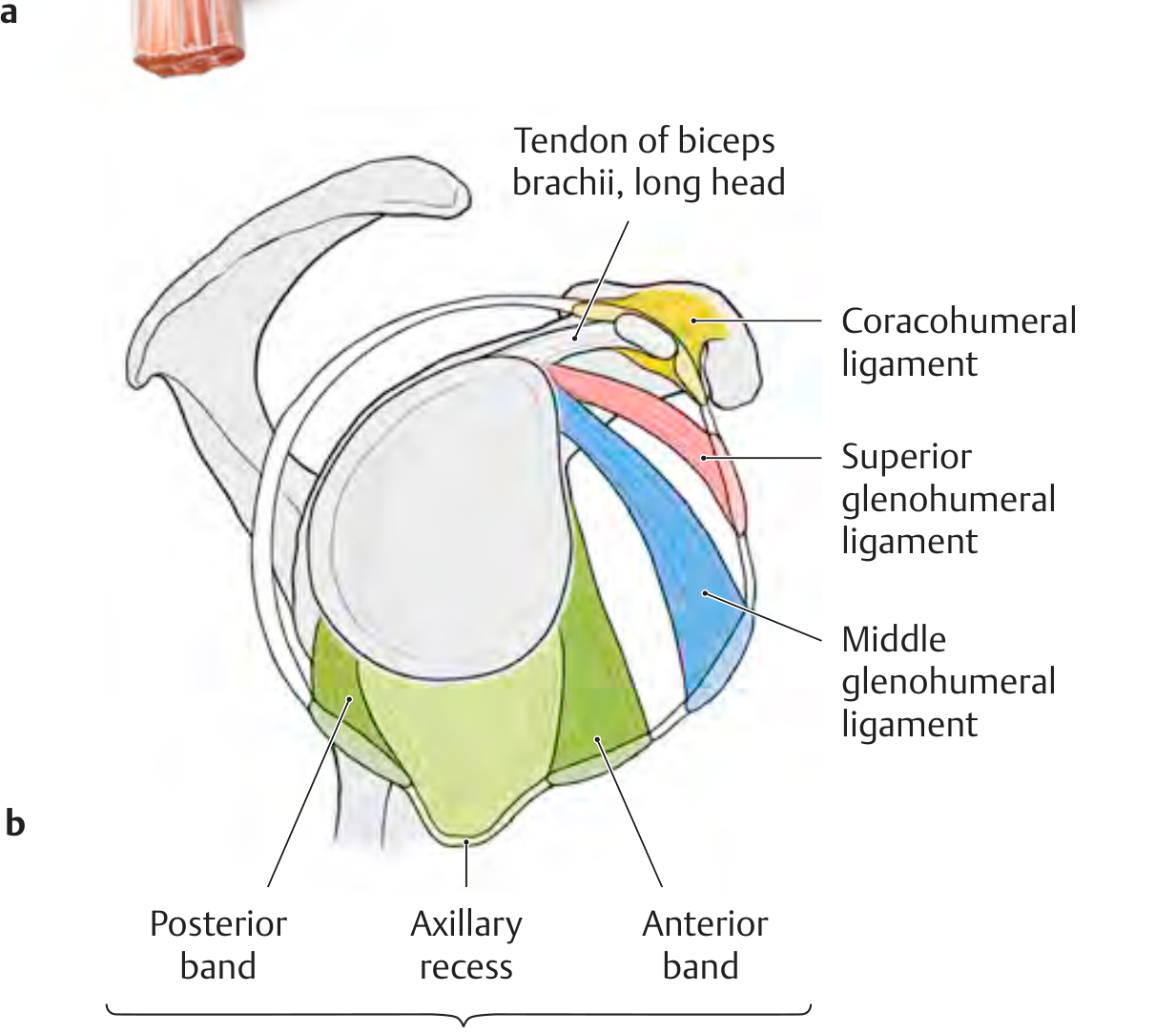
Glenohumeral Ligaments (anterior capsule reinforcements)
| Ligament | Origin | Insertion | Function |
|---|---|---|---|
| Superior GHL (SGHL) | Upper margin of glenoid | Intertubercular groove / lesser tubercle | Forms the rotator interval with the coracohumeral ligament; stabilizes the long head of biceps |
| Middle GHL (MGHL) | Upper margin of glenoid | Anatomic neck of humerus | Crosses almost at a right angle to the subscapularis tendon |
| Inferior GHL (IGHL) | Inferior margin of glenoid | Middle of anatomic neck / surgical neck | Most important stabilizer against anteroinferior instability; has anterior band, posterior band, and axillary recess — forms a "hammock" during abduction |
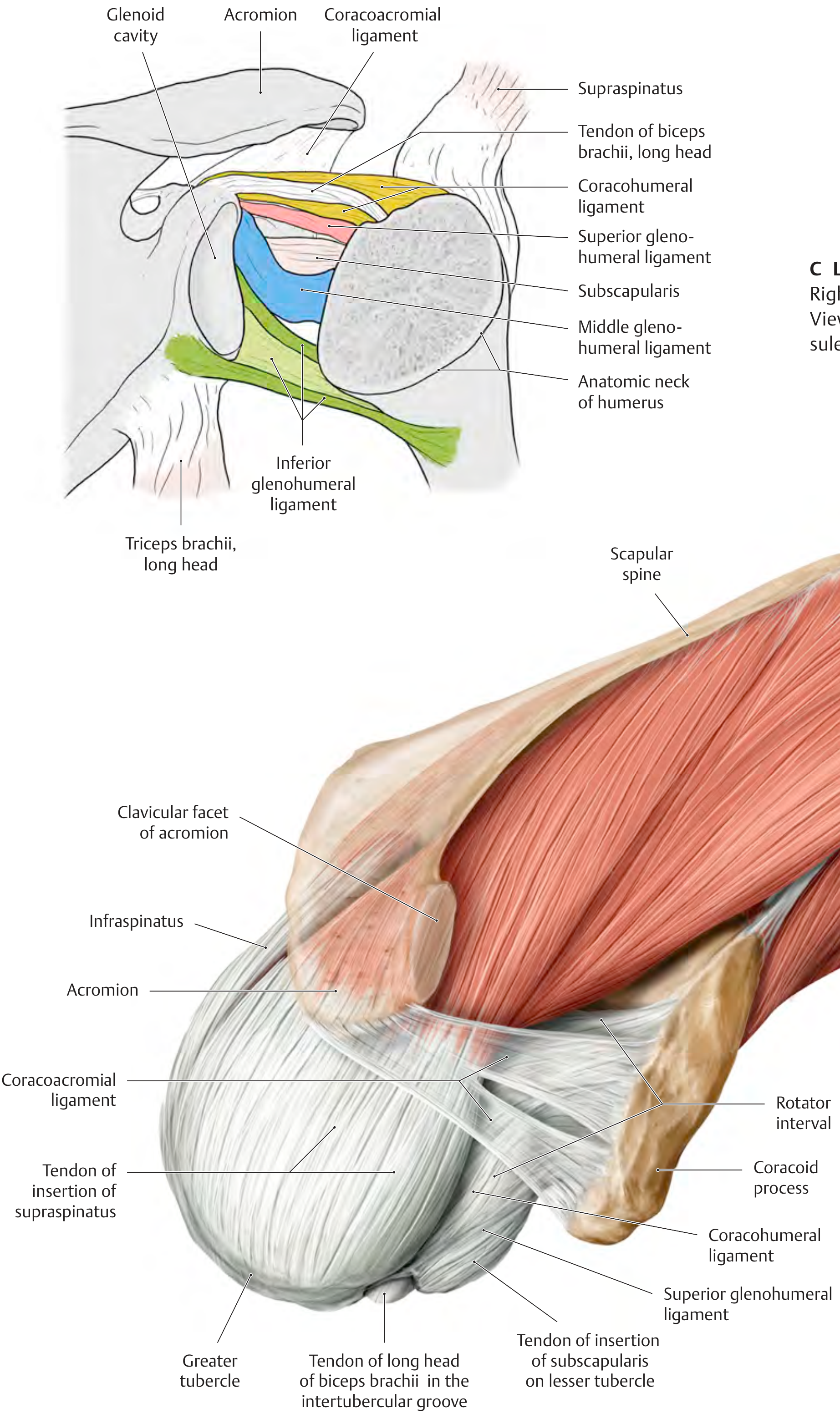
Coracohumeral Ligament (CHL)
Arises from the base of the coracoid process and passes as two bands to the greater and lesser tubercles. It stabilizes the long head of the biceps tendon and forms the roof of the rotator interval.
Coracoacromial Ligament
Spans the coracoid process to the acromion, forming the coracoacromial arch — a secondary restraint preventing superior humeral head escape.
4. Rotator Cuff
The rotator cuff is the primary stabilizer of the glenohumeral joint, compressing the humeral head into the glenoid. It is formed by four muscles (mnemonic: SITS):
| Muscle | Origin | Insertion | Action |
|---|---|---|---|
| Supraspinatus | Supraspinous fossa | Superior facet of greater tubercle | Initiates abduction (0–15°); compresses head superiorly |
| Infraspinatus | Infraspinous fossa | Middle facet of greater tubercle | External rotation; posterior stabilization |
| Teres minor | Lateral border of scapula | Inferior facet of greater tubercle | External rotation; inferior stabilization |
| Subscapularis | Subscapular fossa | Lesser tubercle | Internal rotation; anterior stabilization |
The supraspinatus tendon functions as a gliding tendon over the fulcrum of the humeral head; the critical zone (~1–2 cm proximal to its insertion) is relatively avascular, predisposing it to degenerative tears.
5. Subacromial Space & Bursae
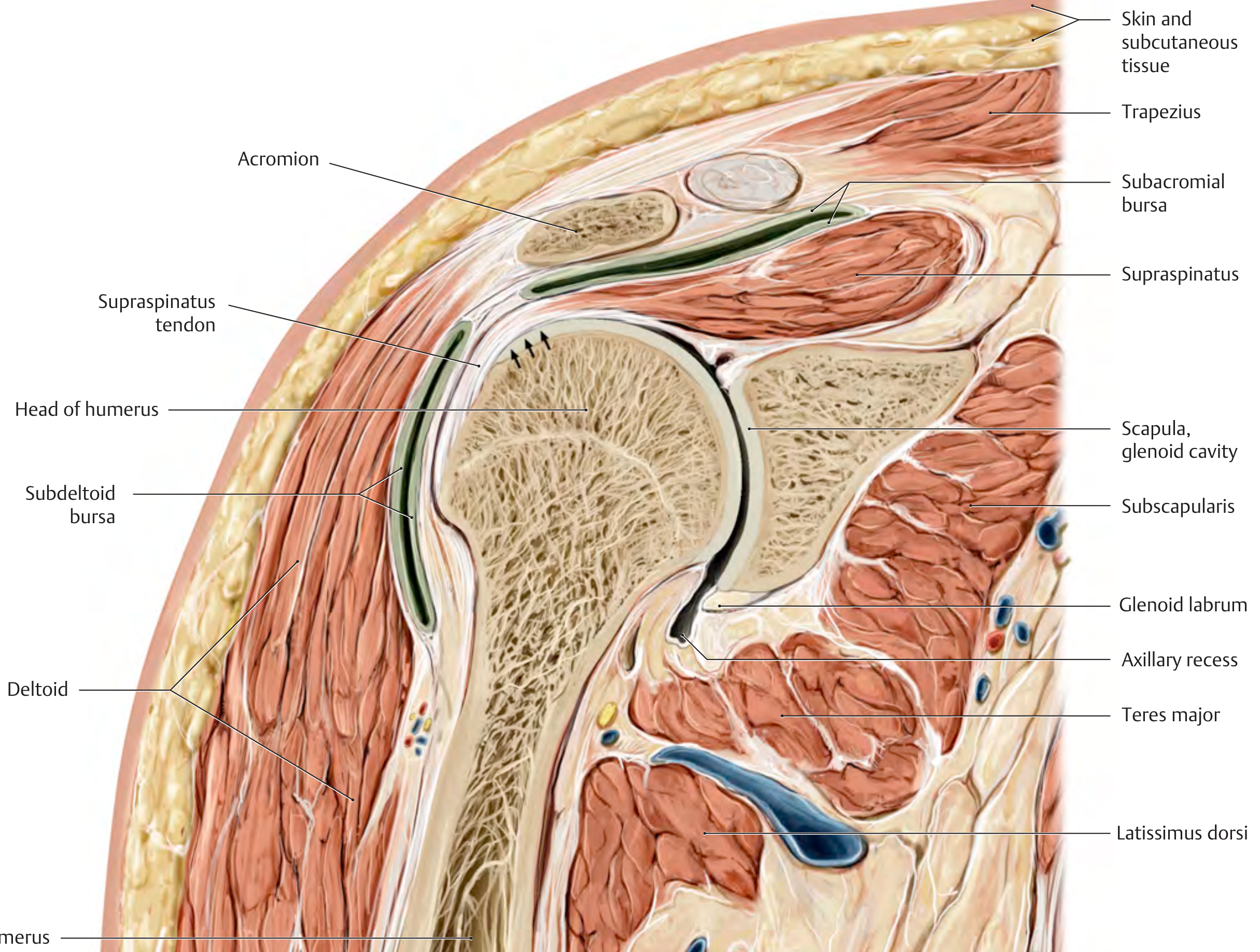
Between the rotator cuff (supraspinatus) and the coracoacromial arch lie two clinically important bursae:
- Subacromial bursa — lies between the supraspinatus tendon and the acromion
- Subdeltoid bursa — communicates consistently with the subacromial bursa
Together they allow frictionless gliding of the rotator cuff beneath the coracoacromial arch during abduction and elevation. A thickened, calcified, or degenerate supraspinatus tendon causes impingement syndrome — pain occurring in the arc between 60° and 120° of abduction.
6. Rotator Interval
The rotator interval is the triangular gap between the anterior border of the supraspinatus and the superior border of the subscapularis tendon. It contains:
- Long head of biceps tendon
- Superior glenohumeral ligament
- Coracohumeral ligament
- Joint capsule
The biceps pulley (biceps sling) — composed of the CHL, SGHL, and transverse humeral ligament — secures the biceps tendon within the bicipital groove.
7. Long Head of Biceps Tendon
- Originates from the supraglenoid tubercle and superior labrum (the bicipital anchor)
- Passes intra-articularly through the rotator interval
- Exits the joint through the intertubercular groove beneath the transverse humeral ligament
- Three attachment types are described based on the depth of the sublabral sulcus (Types I–III)
8. Movements & Biomechanics
As a spheroidal joint, the glenohumeral joint has 3 degrees of freedom and 6 main movement directions:
| Axis | Movements |
|---|---|
| Horizontal axis | Flexion / Extension |
| Sagittal axis | Abduction / Adduction |
| Longitudinal (shaft) axis | Internal / External rotation |
Humeroscapular Rhythm (2:1 ratio)
During full abduction, the arm and scapula move in a 2:1 ratio:
- 60° occurs at the glenohumeral joint
- 30° occurs via scapulothoracic rotation
Beyond 80–90° of abduction, automatic external rotation keeps the greater tubercle from impinging on the coracoacromial arch. Internal rotation while abducting limits range to ~60°.
9. Neurovascular Supply
| Structure | Detail |
|---|---|
| Axillary nerve (C5, C6) | Exits through the quadrangular space; supplies deltoid and teres minor; at risk in surgical neck fractures and anterior dislocations |
| Musculocutaneous nerve | Supplies coracobrachialis, biceps, brachialis |
| Suprascapular nerve | Supraspinatus and infraspinatus |
| Anterior circumflex humeral artery | Small; supplies the humeral head (avascular necrosis risk in neck fractures) |
| Posterior circumflex humeral artery | Larger; accompanies axillary nerve through quadrangular space |
10. Clinical Correlates
| Condition | Anatomy Involved |
|---|---|
| Anterior dislocation (most common, ~95%) | Humeral head dislocates anteroinferiorly; Bankart lesion (labrum), Hill-Sachs lesion (posterosuperior humeral head), axillary nerve/artery injury |
| Rotator cuff tear | Supraspinatus most commonly (critical zone); infraspinatus next; subscapularis (anterior instability) |
| Supraspinatus impingement | Pain arc 60–120° abduction; subacromial bursa inflammation |
| SLAP tear | Superior labral tear from anterior to posterior; bicipital anchor disrupted |
| Frozen shoulder (adhesive capsulitis) | Contracture of the joint capsule and rotator interval |
| Bankart lesion | Anteroinferior labral avulsion ± bony fragment; treated arthroscopically with anchor sutures |
Sources: THIEME Atlas of Anatomy — General Anatomy and Musculoskeletal System; Imaging Anatomy Text and Atlas Vol. 3 — Bones, Joints, Vessels and Nerves; Gray's Anatomy for Students
This is a shared conversation. Sign in to Orris to start your own chat.