Here is the complete, exam-ready answer for all your MUHS 2nd MBBS Pathology topics:
2nd MBBS Pathology - MUHS Exam Complete Notes
Based on Robbins & Kumar Basic Pathology + Robbins & Cotran Pathologic Basis of Disease
SAQ SECTION
SAQ 1 - Factors Affecting Wound Healing (Enumerate) + Complications
Factors Affecting Wound Healing
LOCAL FACTORS
- Infection - most common cause of delayed healing; bacteria produce enzymes that damage tissue and prevent collagen deposition
- Blood supply - ischemia (peripheral vascular disease, diabetes) impairs healing
- Foreign body - sutures, glass, bone fragments incite chronic inflammation
- Mechanical factors - excessive movement, pressure, tension
- Wound size and depth - larger wounds require more granulation tissue
- Radiation - damages microvasculature and reduces fibroblast proliferation
- Denervation - reduced trophic support impairs healing (e.g., neuropathic ulcers)
SYSTEMIC FACTORS
- Diabetes mellitus - impaired leukocyte function, microangiopathy, neuropathy
- Malnutrition - protein deficiency, Vitamin C deficiency (collagen synthesis requires hydroxylation by Vit C), Zinc deficiency (cofactor for metalloenzymes)
- Corticosteroids / immunosuppressants - inhibit TGF-β, reduce collagen synthesis
- Anemia - reduced oxygen delivery
- Jaundice / uremia - toxic to fibroblasts
- Hematological disorders - thrombocytopenia (impairs initial hemostasis)
- Age - decreased fibroblast activity in elderly
- Obesity - poor blood supply to fat, increased tension
Mnemonic: MIND IT
Malnutrition, Infection, Neuropathy/Necrosis, Drugs (steroids), Ischemia, Temperature (cold), Tension
Complications of Wound Healing
| Complication | Description |
|---|
| Deficient scar | Dehiscence - wound breaks apart (poor collagen); Ulceration - chronic wound |
| Excessive scarring | Hypertrophic scar (stays within wound margins); Keloid (grows beyond margins - more common in dark-skinned individuals; contains thick type I collagen bundles) |
| Contracture | Excessive contraction → deformity (esp. palm, sole, anterior neck, burns) |
| Suture marks | Foreign body reaction |
| Pigment changes | Hyper/hypopigmentation |
| Incisional hernia | Weakened scar in abdominal wall |
| Wound infection | Commonest complication |
| Proud flesh | Excessive granulation tissue above skin level |
SAQ 2 - Chemotaxis and Phagocytosis
Chemotaxis
Definition: Directed movement of leukocytes towards the site of injury along a chemical concentration gradient.
Chemotactic agents (chemoattractants):
- Exogenous: Bacterial products (especially N-formylmethionyl peptides - fMLP)
- Endogenous:
- Complement fragment C5a (most potent)
- Leukotriene B4 (LTB4)
- Chemokines (e.g., IL-8/CXCL8)
- Products of the fibrinolytic cascade
Mechanism:
- Chemoattractant binds G-protein coupled receptor on leukocyte surface
- Activates phospholipase C → IP3 + DAG
- IP3 → Ca²⁺ release → cytoskeleton rearrangement
- Formation of pseudopods at leading edge (actin polymerization)
- Cell moves towards higher concentration of attractant
Chemoattractant gradient
Low ←------------------------→ High (site of injury)
Leukocyte moves →→→
Phagocytosis
Definition: Engulfment of particles (microbes, dead cells, debris) by leukocytes.
Steps:
Step 1 - Recognition and Attachment:
- Enhanced by opsonins: IgG (Fc portion binds FcγRIII receptor) and C3b (binds CR1 receptor)
- Pattern recognition receptors (e.g., mannose receptor, TLRs) also bind directly
Step 2 - Engulfment:
- Pseudopods extend around particle
- Phagosome forms (cytoplasmic vacuole)
- Lysosome fuses with phagosome → phagolysosome
Step 3 - Killing and Degradation (Intracellular killing):
(A) Oxygen-dependent (most important):
- Respiratory burst: NADPH oxidase converts O₂ to superoxide (O₂⁻)
- Superoxide → H₂O₂ → hypochlorous acid (HOCl) via myeloperoxidase (MPO)
- HOCl is most potent oxidant for bacterial killing
- iNOS → Nitric oxide (NO) → combined with O₂⁻ → peroxynitrite (also bactericidal)
(B) Oxygen-independent:
- Lysozyme (degrades cell walls)
- Lactoferrin (chelates iron - bacteriostatic)
- Defensins (antimicrobial peptides)
- Acid hydrolases
- Major basic protein (eosinophils - against helminths)
Diagram - Phagocytosis Steps:
Microbe
↓ [Opsonization by IgG + C3b]
Attachment to Fc/C3b receptors
↓
Pseudopod formation → Engulfment
↓
Phagosome
↓ [Lysosome fusion]
Phagolysosome
↓ [NADPH oxidase → O₂⁻ → H₂O₂ → HOCl via MPO]
Bacterial killing + Degradation
Clinical correlates:
- Chronic Granulomatous Disease (CGD): NADPH oxidase deficiency → recurrent catalase-positive bacterial infections
- Chediak-Higashi syndrome: Defective lysosome fusion → recurrent pyogenic infections
- Myeloperoxidase deficiency: Mild susceptibility to candidiasis
SAQ 3 - Lepromatous Leprosy: Gross and Microscopic Findings
Background
Lepromatous leprosy (LL) is the multibacillary pole of leprosy spectrum - occurs in patients with poor cell-mediated immunity (CMI) to M. leprae. Th2 response predominates; Th1 response absent → bacilli multiply unchecked.
Gross Findings
- Skin lesions: Multiple, small, poorly defined, symmetric, pale macules - blend into surrounding skin
- Infiltrations - diffuse infiltration of face → "Leonine facies" (lion-like appearance)
- Lepromas - poorly defined nodules on ears, nose, chin, elbows, knees, buttocks
- Madarosis - loss of outer third of eyebrows (pathognomonic), then eyelashes
- Saddle nose deformity - cartilage/bone resorption
- Gynecomastia - due to testicular involvement
- Nerve involvement: Bilateral, symmetric, stocking-glove pattern (peripheral neuropathy; misdiagnosed as diabetic neuropathy)
- "Varnished skin" / waxy, shiny appearance in diffuse type
- Lagophthalmos - inability to close eyes due to facial nerve damage
- Lucio phenomenon in diffuse leprosy (erythema necroticans)
Microscopic Findings (Histopathology)
KEY FEATURES:
- Virchow cells (Lepra cells): Large foamy macrophages stuffed with M. leprae bacilli (appear as "globi" - packets of bacilli). This is the hallmark.
- Grenz zone (Unna's zone): A clear zone of normal uninvolved dermis just beneath the epidermis (separates the dermis infiltrate from the epidermis)
- NO granulomas - no epithelioid cell granulomas (due to absent CMI)
- No giant cells
- Bacilli extremely numerous - AFB stain (Fite-Faraco) shows numerous organisms
- Lymphocytic infiltrate is scanty (vs tuberculoid where lymphocytes are abundant)
- Nerves are infiltrated and destroyed but slowly
- Atrophic epidermis
Easy diagram for exam:
Histopathology of Lepromatous Leprosy:
EPIDERMIS (thinned/atrophied)
══════════════════════════════
[GRENZ ZONE - clear zone]
══════════════════════════════
DERMIS:
[🫧 Virchow cells (foamy macrophages)]
[🫧 Virchow cells] [Lymphocytes - few]
[🫧 Virchow cells] [Globi on AFB stain]
[Nerve - infiltrated, intact long]
══════════════════════════════
Lepromin test: NEGATIVE in lepromatous leprosy
SAQ 4 - Primary Tuberculosis: Pathogenesis
Pathogenesis of Primary Tuberculosis
Primary TB occurs in a previously unexposed (unsensitized) host. Only ~5% develop significant disease; the rest heal.
Step 1 - Inhalation of bacilli:
- Mycobacterium tuberculosis droplet nuclei (<5 μm) inhaled → reach distal alveoli (lower lobe of upper lobe or upper lobe of lower lobe, close to pleura)
Step 2 - Initial infection (0-3 weeks):
- Alveolar macrophages phagocytose bacilli
- Bacilli resist killing by: inhibiting phagosome-lysosome fusion (by preventing acidification), scavenging reactive oxygen species
- Bacilli multiply within macrophages → some escape and are taken up by dendritic cells → transported to hilar lymph nodes
- At this stage: NO CMI, No hypersensitivity → bacilli spread freely
Step 3 - Development of Cell-Mediated Immunity (3-8 weeks):
- Dendritic cells present mycobacterial antigens to CD4+ T cells in lymph nodes
- T cells differentiate into Th1 cells
- Th1 cells produce IFN-γ → activates macrophages
- Activated macrophages produce:
- Reactive oxygen/nitrogen species → kill bacilli
- TNF → recruits more monocytes
- Chemokines → granuloma formation
- Tuberculin test becomes positive at this stage (3-8 weeks)
Step 4 - Granuloma Formation:
- Activated macrophages → "epithelioid histiocytes" → aggregate around bacilli
- Some fuse → Langhans giant cells (nuclei arranged in horseshoe/peripheral pattern)
- Surrounded by lymphocytes
- Central caseous necrosis due to delayed-type hypersensitivity (Type IV)
Step 5 - Outcome (Ghon Complex formation):
- Ghon focus: 1-1.5 cm gray-white area of consolidation in parenchyma (caseous center)
- Bacilli travel via lymphatics → hilar/paratracheal lymph nodes (also caseate)
- Ghon Complex = Ghon focus + involved lymph nodes + connecting lymphangitis
- In ~95% → fibrosis + calcification → Ranke complex (radiologically visible)
- Hematogenous dissemination may occur (controlled by CMI in most)
PATHOGENESIS DIAGRAM:
Inhaled bacilli
↓
Alveolar macrophages (phagocytose but cannot kill initially)
↓ [3-8 weeks]
CD4+ T cells → Th1 response → IFN-γ
↓
Macrophage activation + Granuloma formation
↓
GHON FOCUS (lung parenchyma) + Lymph node caseation
↓
GHON COMPLEX = Ghon focus + lymphadenitis + lymphangitis
↓
95%: Fibrosis → Calcification (Ranke complex)
5%: Progressive primary TB (immunocompromised)
SAQ 5 - Inflammation: Chemical Mediators
Classification of Chemical Mediators
Chemical mediators can be:
- Cell-derived (preformed in granules OR newly synthesized)
- Plasma-derived (circulate as precursors, activated at injury site)
CELL-DERIVED MEDIATORS
1. Vasoactive Amines
Histamine:
- Source: Mast cells (main), basophils, platelets
- Triggers: C3a, C5a, physical injury, neuropeptides, cytokines
- Actions: Vasodilation, increased vascular permeability (most important early mediator)
- Receptors: H1, H2
Serotonin (5-HT):
- Source: Platelets (after activation)
- Actions: Vasoconstriction, increased permeability
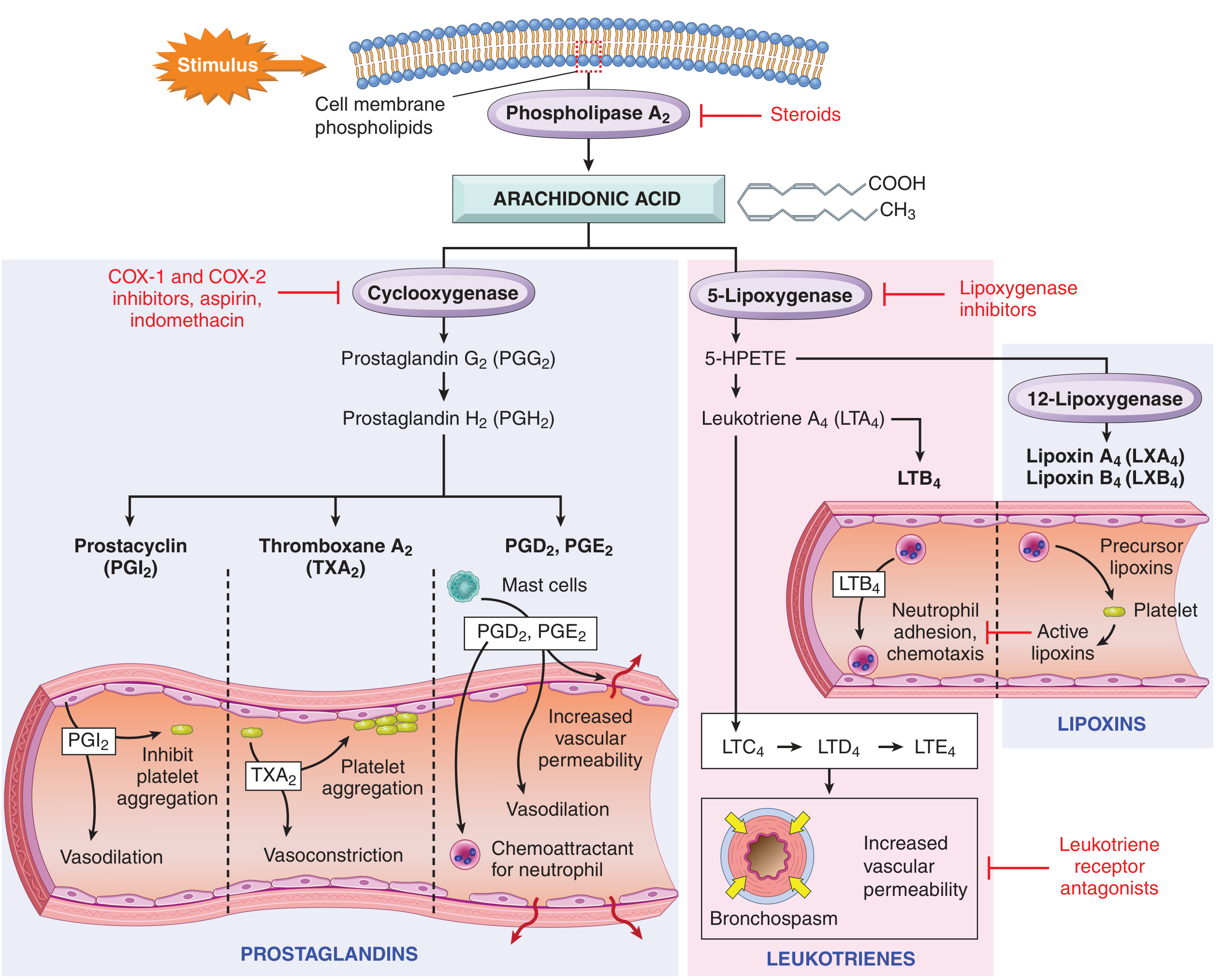
2. Arachidonic Acid Metabolites (Eicosanoids)
Generated from cell membrane phospholipids (phospholipase A2 cleaves arachidonic acid):
Prostaglandins (via COX pathway):
- PGE2, PGI2 (prostacyclin): Vasodilation, pain, fever
- TXA2: Vasoconstriction, platelet aggregation
Leukotrienes (via 5-Lipoxygenase pathway):
- LTB4: Chemotaxis, neutrophil adhesion (potent)
- LTC4, LTD4, LTE4 (cysteinyl leukotrienes): Increased vascular permeability, bronchoconstriction (important in asthma)
Arachidonic acid metabolism - Robbins & Kumar Basic Pathology
3. Platelet Activating Factor (PAF)
- Source: Mast cells, basophils, platelets, macrophages, endothelium
- Actions: Platelet aggregation, bronchoconstriction, increased vascular permeability (10,000x more potent than histamine)
4. Cytokines
TNF and IL-1:
- Source: Activated macrophages, dendritic cells
- Actions:
- Endothelial activation → upregulate adhesion molecules (E/P selectins, ICAM-1, VCAM-1)
- Fever (via PGE2 in hypothalamus)
- Cachexia, SIRS (septic shock)
- Chemokine production
- IL-1 activates Th17 cells
IL-6: Acute phase protein synthesis by liver (CRP, fibrinogen, serum amyloid A)
Chemokines (IL-8/CXCL8):
- Chemotaxis of neutrophils (most potent)
- Activates leukocyte integrins
5. Reactive Oxygen and Nitrogen Species
- ROS (O₂⁻, H₂O₂, OH•): Microbial killing, endothelial damage
- Nitric Oxide (NO): Vasodilation (via cGMP in smooth muscle), microbicidal
6. Lysosomal Enzymes
- Source: Neutrophils and macrophages
- Neutral proteases (elastase, collagenase), acid hydrolases
- Actions: Tissue destruction, complement and kinin activation
PLASMA-DERIVED MEDIATORS
1. Complement System
- C3a and C5a (anaphylatoxins): Mast cell degranulation → histamine release → increased permeability
- C5a: Most potent chemotactic factor for neutrophils; also activates leukocytes
- C3b: Opsonization
- C5b-9 (MAC): Lysis of microorganisms
2. Kinin System
- Bradykinin: Vasodilation, increased vascular permeability, pain (most important pain mediator in inflammation), bronchospasm
- Generated from kininogen by kallikrein
- Activated by Hageman factor (Factor XII)
3. Coagulation/Fibrinolytic System
- Thrombin: Platelet activation, fibrin deposition
- Fibrin degradation products: Increased vascular permeability, chemotaxis
Summary Table
| Mediator | Source | Key Actions |
|---|
| Histamine | Mast cells | Vasodilation, ↑ permeability |
| PGE2/PGI2 | All cells | Vasodilation, pain, fever |
| TXA2 | Platelets | Vasoconstriction, platelet aggregation |
| LTB4 | Leukocytes | Chemotaxis |
| LTC4,D4,E4 | Mast cells | ↑ permeability, bronchoconstriction |
| IL-1, TNF | Macrophages | Fever, leukocyte adhesion, SIRS |
| IL-8 (CXCL8) | Macrophages, endothelium | Neutrophil chemotaxis |
| C5a | Complement | Chemotaxis, ↑ permeability |
| C3b | Complement | Opsonization |
| Bradykinin | Plasma | Pain, vasodilation, ↑ permeability |
| NO | Endothelium/macrophages | Vasodilation, microbicidal |
SAQ 6 - Ridley and Jopling Classification of Leprosy
Spectrum of Leprosy (5-group classification based on CMI vs bacterial load)
The Ridley-Jopling classification divides leprosy into a spectrum based on the patient's cell-mediated immunity (CMI) to M. leprae:
┌──────────────────────────────────────────────────────────┐
│ ← STRONG CMI ────────────────────── WEAK/NO CMI → │
│ │
│ TT BT BB BL LL │
│ │
│ Tuberculoid ←── Borderline ──→ Lepromatous │
│ │
│ [Paucibacillary] [Multibacillary] │
└──────────────────────────────────────────────────────────┘
| Feature | TT (Tuberculoid) | BT | BB (Borderline) | BL | LL (Lepromatous) |
|---|
| Lesions | 1-3, well-defined | Few, asymmetric | Several, irregular | Many, less defined | Numerous, small, symmetric |
| Edges | Sharp, raised | Raised | Punched-out inner edge | Sloping | Ill-defined |
| Sensation | Absent (anesthetic) | Reduced | Variable | Slightly reduced | Minimal loss |
| Hair loss | Present | Present | Variable | Present | Present |
| Nerve thickening | One nerve | One or more | Variable | Multiple | Bilateral symmetric (stocking-glove) |
| Bacillary load (BI) | 0 | 1+ | 2-3+ | 4-5+ | 6+ |
| Lepromin test | Strongly + | + | ± | - | Strongly - |
| CMI | Strong | Good | Unstable | Reduced | Absent |
| Histology | Epithelioid granulomas, no bacilli, nerve destruction, Grenz zone absent | Similar to TT | Mix of types | Macrophages beginning to foam | Virchow (foamy) macrophages, Grenz zone, NO granulomas |
| Stability | Stable | Unstable - may upgrade or downgrade | Very unstable | Unstable | Relatively stable |
WHO Classification (practical):
- Paucibacillary (PB): TT, BT, some BB → ≤5 skin lesions
- Multibacillary (MB): BB, BL, LL → >5 skin lesions
Mnemonic for spectrum: TT-BT-BB-BL-LL = "To Be Borderline Becomes Lepromatous"
SAQ 7 - Acute Inflammation: Definition, Vascular Events, Cellular Events, Types
Definition
Acute inflammation is the immediate and early response of the body to injury/infection, characterized by:
- Exudation of plasma proteins
- Emigration of leukocytes (predominantly neutrophils)
- Mediated by chemical mediators
- Short duration (hours to days)
Cardinal Signs (Celsus + Virchow):
- Rubor (redness) - vasodilation
- Calor (heat) - increased blood flow
- Tumor (swelling) - edema from exudation
- Dolor (pain) - bradykinin, PGE2, neuropeptides
- Functio laesa (loss of function) - added by Virchow
Vascular Events in Acute Inflammation
1. Transient vasoconstriction (seconds, reflex, neurogenic - insignificant)
2. Vasodilation:
- Arterioles dilate first, then capillaries
- Mediated by: histamine, NO, PGE2
- Results in: redness (rubor) and heat (calor)
3. Increased vascular permeability (most important vascular event):
| Mechanism | Mechanism | Example |
|---|
| Endothelial contraction | Histamine, LTC4, bradykinin widen interendothelial gaps (15-30 min) | Immediate transient response |
| Endothelial retraction | Cytokines (IL-1, TNF) reorganize cytoskeleton (4-6 hrs, prolonged) | Delayed prolonged response |
| Direct endothelial injury | Burns, severe injury → cell death | Immediate sustained response |
| Leukocyte-mediated injury | Activated neutrophils/macrophages release enzymes → endothelial damage | Late response |
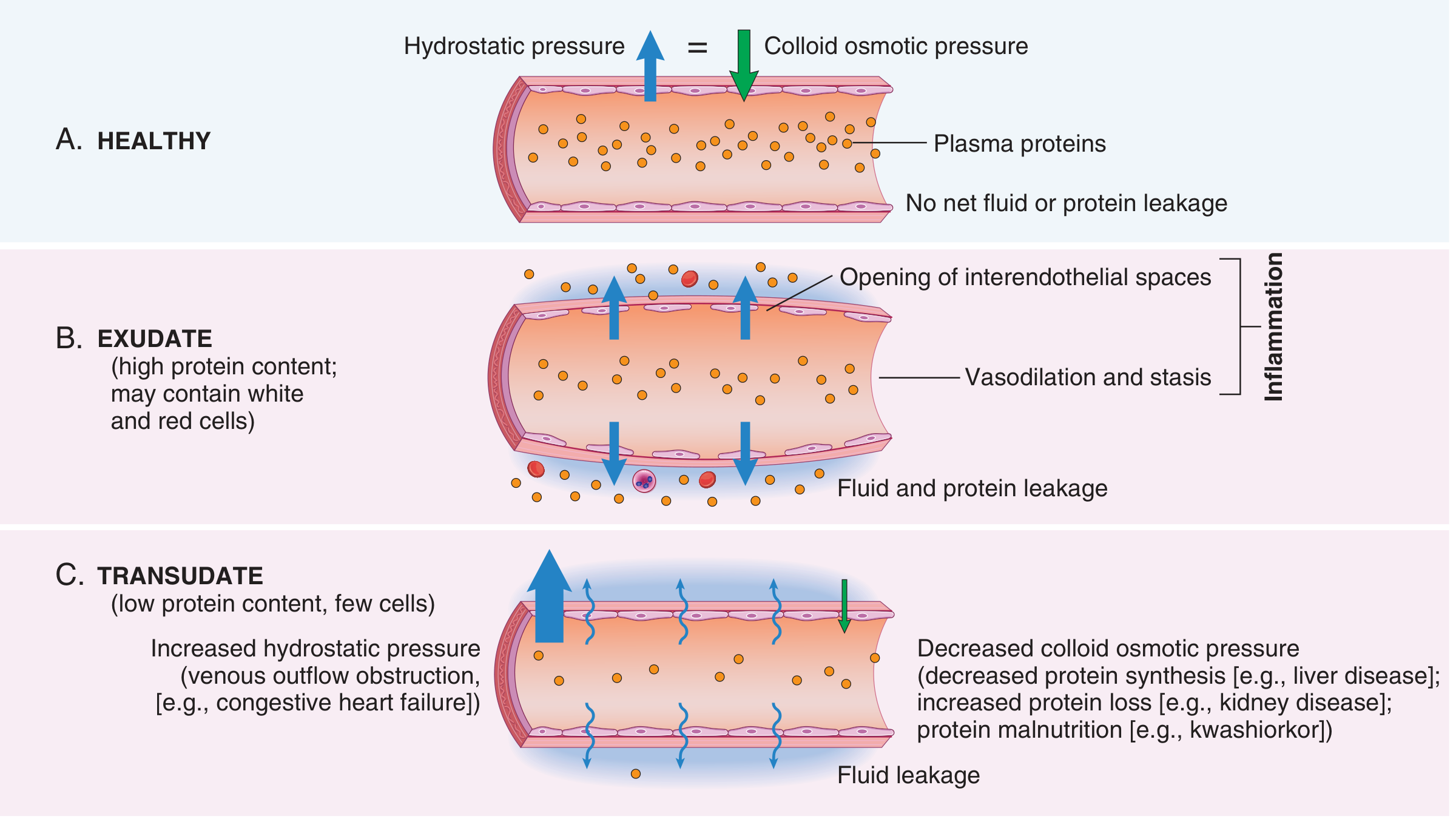
| Increased transcytosis | VEGF-mediated | Tumors, healing |
Result: Protein-rich exudate → edema (tumor) → hemoconcentration → stasis
4. Stasis:
- Slowing of blood flow → rouleaux formation → increased viscosity
- Sets stage for leukocyte margination
Exudate formation in inflammation - Robbins & Kumar Basic Pathology
Cellular Events (Leukocyte Emigration)
Sequence: Margination → Rolling → Adhesion → Transmigration → Chemotaxis → Phagocytosis
1. Margination:
- Stasis → RBCs concentrate centrally → leukocytes pushed to vessel wall
- Leukocytes move to endothelium
2. Rolling:
- Loose adhesion: Selectins
- P-selectin (on endothelium, from Weibel-Palade bodies) + E-selectin (induced by IL-1, TNF)
- Bind sialyl-Lewis X on leukocytes
- Leukocytes roll along endothelium
3. Firm Adhesion:
- Integrins on leukocytes (LFA-1/Mac-1 = CD11a/CD18) bind ICAM-1 on endothelium
- VCAM-1 binds VLA-4 integrin on leukocytes
- Integrins activated by chemokines
4. Transmigration (Diapedesis):
- Leukocytes squeeze through interendothelial junctions (mainly postcapillary venules)
- Mediated by PECAM-1 (CD31) - platelet endothelial cell adhesion molecule
- Secrete collagenase to cross basement membrane
5. Chemotaxis:
- Directed migration toward C5a, LTB4, IL-8, bacterial fMLP
6. Phagocytosis (see SAQ 2)
CELLULAR EVENTS DIAGRAM:
VESSEL LUMEN:
[RBC][RBC][WBC rolling]→→→→→→→[WBC adhering]
ENDOTHELIUM
↑ E/P selectin ↑ ICAM-1
[WBC squeezing through] ← PECAM-1 on junctions
↓ TRANSMIGRATION
INTERSTITIUM: WBC migrating toward C5a/IL-8/LTB4
↓ CHEMOTAXIS
SITE OF INJURY → PHAGOCYTOSIS
Sequence of leukocytes:
- 0-24 hours: Neutrophils predominate (first responders)
- 24-48 hours: Monocytes/Macrophages replace neutrophils (longer lived)
- Exception: Viral infections and Rickettsial - lymphocytes first
Morphologic Types of Acute Inflammation
- Serous inflammation: Watery exudate, low protein (e.g., skin blisters, pleural effusion in early infection)
- Fibrinous inflammation: Large permeability increase → fibrinogen → fibrin deposition (e.g., fibrinous pericarditis - "bread and butter" pattern; fibrinous pleuritis)
- Suppurative (Purulent) inflammation: Pus (neutrophils + liquefactive necrosis + dead tissue). Examples: Abscess (localized), cellulitis (diffuse), empyema (in cavities)
- Ulcerative inflammation: Necrosis at surface → mucosal ulcers (peptic ulcer, aphthous ulcer)
- Pseudomembranous inflammation: Necrotic membrane on mucosal surfaces (e.g., diphtheria, C. diff colitis)
- Hemorrhagic inflammation: Blood vessel destruction + RBC extravasation (e.g., anthrax, plague)
Outcomes of Acute Inflammation
- Resolution - complete restoration (pneumonia resolution)
- Healing by scarring/fibrosis - if tissue damage extensive
- Abscess formation - walled-off pus collection
- Progression to chronic inflammation - persistent stimulus
SAQ 8 - Granulation Tissue (Gross, Microscopy) + Delayed Wound Healing
Granulation Tissue
Definition: Specialized tissue formed in healing wounds - consists of new blood vessels (angiogenesis) + proliferating fibroblasts in a loose extracellular matrix.
Name derivation: Pinkish-red granular appearance on surface of healing wounds.
Gross Appearance:
- Pink/red, granular, moist surface
- Bleeds easily on touch (rich vascularity)
- Soft, boggy texture
- Appears by day 3-5 after injury
- Gradually replaced by scar tissue
Microscopic Appearance:
HISTOPATHOLOGY OF GRANULATION TISSUE:
┌─────────────────────────────────────┐
│ Proliferating fibroblasts │
│ (spindle-shaped, pale cytoplasm) │
│ │
│ New capillaries (thin-walled, │
│ open lumens) - angiogenesis │
│ │
│ Loose ECM (type III collagen, │
│ fibronectin, hyaluronan) │
│ │
│ Inflammatory cells │
│ (macrophages, lymphocytes, │
│ occasional neutrophils) │
│ │
│ Myofibroblasts (α-SMA positive) │
│ → wound contraction │
└─────────────────────────────────────┘
Key histological features:
- Numerous thin-walled capillaries with open lumens (perpendicular to surface)
- Plump proliferating fibroblasts (activated by TGF-β, PDGF, FGF)
- Loose ECM (edematous stroma)
- Macrophages (secrete growth factors: VEGF, TGF-β)
- NO epithelium initially
Growth factors driving granulation tissue:
- VEGF → angiogenesis
- TGF-β → fibroblast activation, collagen synthesis
- PDGF, FGF → fibroblast and smooth muscle proliferation
- EGF → epithelial regeneration
Causes of Delayed Wound Healing (Enumerate)
Local causes:
- Infection (most common)
- Poor blood supply / ischemia
- Foreign body
- Necrotic tissue / eschar
- Excessive movement / mechanical disruption
- Radiation damage
- Denervation
Systemic causes:
- Diabetes mellitus
- Malnutrition (protein, Vit C, Zinc deficiency)
- Corticosteroids / immunosuppressive drugs
- Anemia / hypoxia
- Uremia, jaundice
- Advanced age
- Obesity
- Malignancy
- Hematological disorders (thrombocytopenia)
SAQ 9 - Wound Healing by Primary Intention + Secondary Intention
Healing by Primary Intention (First Intention)
Definition: Healing of clean, sutured wounds with minimal tissue loss and no infection. Edges are apposed.
Example: Clean surgical incision closed with sutures.
Steps:
| Time | Events |
|---|
| Immediately | Narrow incision; fibrin clot fills gap; clot dehydrates → scab |
| 24-48 hours | Neutrophils at margins; epithelial cells migrate from both edges along deep margin → reseal epidermis |
| Day 3 | Macrophages replace neutrophils; granulation tissue begins to invade; collagen fibers start forming |
| Day 5 | Neo-vascularization maximal; granulation tissue fills incision space; collagen bridging |
| Week 2 | Continued collagen accumulation; vessels regress; leukocytes disappear |
| Month 1 onwards | Scar: collagen type I replaces type III; remodeling (MMP activity); strength increases |
| Final | Fine white scar (minimal fibrosis); tensile strength reaches ~80% of normal at 3 months |
WOUND HEALING BY 1° INTENTION:
Day 0: |SKIN|____|SKIN| ← wound gap, fibrin clot
Day 1-2: |----→→→→←----| ← epithelial migration
Day 3-5: | Granulation | ← granulation tissue fills
tissue + vessels
Week 2: | Collagen | ← remodeling begins
Month 1+: | SCAR | ← fine scar
Healing by Secondary Intention (Second Intention)
Definition: Healing of large tissue defects, contaminated wounds, or wounds with ragged edges - where edges cannot be approximated.
Example: Large ulcers, burns, infected wounds, tooth extraction socket.
Differences from primary intention:
| Feature | Primary (1°) | Secondary (2°) |
|---|
| Tissue defect | Minimal | Large |
| Inflammation | Mild | Intense and prolonged |
| Granulation tissue | Little | Abundant |
| Wound contraction | Minimal | Marked (myofibroblasts) |
| Scar | Fine, minimal | Larger, more prominent |
| Time | Faster | Slower |
| Re-epithelialization | Easy | Slow (large surface) |
Steps in Secondary Intention:
- Large defect fills with fibrin clot initially
- Intense inflammatory reaction clears debris (macrophages dominant)
- Granulation tissue fills from base upward (extensive)
- Wound contraction - key feature - myofibroblasts (modified fibroblasts with smooth muscle characteristics) pull wound edges together (up to 5-10% of original area)
- Re-epithelialization from wound edges (slow)
- Progressive scar formation and remodeling
SAQ 10 - Primary Tuberculosis: Common Sites, Primary Complex, Evolution of Tubercle
Common Sites of Primary TB
- Lungs - most common (95%); lower part of upper lobe or upper part of lower lobe, close to pleura
- Tonsils
- Cervical lymph nodes (via tonsils)
- Small intestine (ileocecal region) - via ingestion of contaminated milk (Bovine TB - M. bovis)
- Skin (inoculation TB - rare)
Primary Complex (Ghon Complex) - Components
THREE components:
- Ghon focus (Primary focus / Ghon lesion): 1-1.5 cm area of consolidation with central caseous necrosis in lung parenchyma
- Lymphangitis: Inflammation along lymphatics draining the Ghon focus
- Lymphadenitis: Caseous enlargement of hilar/paratracheal lymph nodes
GHON COMPLEX DIAGRAM:
┌─────────────────────────────┐
│ LUNG │
│ │
│ Ghon focus │
│ [caseous 1-1.5cm] ←←←←← │
│ | │
│ | lymphangitis │
│ ↓ │
│ [Hilar lymph node] │
│ (caseous necrosis) │
└─────────────────────────────┘
Ghon Complex = Ghon focus + lymphangitis + enlarged lymph node
Evolution/Fate of Tubercle (Schematic)
INHALED BACILLI
↓
INITIAL ALVEOLAR LESION (non-specific pneumonia)
↓ [3 weeks - CMI develops]
TUBERCLE FORMATION
- Epithelioid macrophages aggregate
- Langhans giant cells form (nuclei peripherally/horseshoe arranged)
- Lymphocytic cuff surrounds
- Central CASEOUS NECROSIS
↓
GHON FOCUS (mature tubercle)
↓
┌─────────────────────────────────────────────────────┐
│ FATE (95% healthy individuals) │
│ │
│ Fibrosis → Calcification → RANKE COMPLEX │
│ (detectable on X-ray as calcified nodule + node) │
└─────────────────────────────────────────────────────┘
OR (5% / immunocompromised)
┌─────────────────────────────────────────────────────┐
│ PROGRESSIVE PRIMARY TB │
│ Liquefaction of caseous material │
│ Cavity formation │
│ Spread: Bronchogenic/Lymphatic/Hematogenous │
└─────────────────────────────────────────────────────┘
Microscopic stages of tubercle evolution:
- Stage 1: Neutrophilic exudate (0-1 week)
- Stage 2: Epithelioid cell accumulation (2-3 weeks)
- Stage 3: Langhans giant cells + lymphocyte cuff (3-4 weeks)
- Stage 4: Central caseous necrosis (4+ weeks)
- Stage 5: Fibrosis + calcification (healing)
SAQ 11 - Ghon's Complex: Gross, Microscopic Features, Fate
Gross Features of Ghon Complex
Ghon Focus:
- 1-1.5 cm diameter, gray-white area of consolidation
- Close to pleura (subpleural)
- Center shows caseous necrosis - cheese-like, yellowish-white, solid material
- Hard chalky consistency on calcification
- Lower part of upper lobe or upper part of lower lobe
Lymph Nodes:
- Hilar lymph nodes enlarged (often larger than the primary focus)
- Caseous necrosis within nodes
- On healing: fibrosis + calcification (may be visible on X-ray)
Ranke Complex (healed Ghon complex):
- Calcified Ghon focus + calcified lymph nodes → visible on chest X-ray
Microscopic Features
MICROSCOPY DIAGRAM - TUBERCULOUS GRANULOMA:
┌──────────────────────────────┐
│ CENTRAL CASEOUS NECROSIS │
│ (pink amorphous material, │
│ no nuclear debris, │
│ ghost cell outlines) │
│ │
│ ┌────────────────────┐ │
│ │ Epithelioid cells │ │
│ │ (activated macro- │ │
│ │ phages; oval │ │
│ │ nuclei, abundant │ │
│ │ pink cytoplasm) │ │
│ └────────────────────┘ │
│ │
│ LANGHANS GIANT CELLS │
│ (10-50 nuclei arranged │
│ at periphery in │
│ horseshoe/ring pattern) │
│ │
│ CD4+ Lymphocyte cuff │
│ (outermost layer) │
└──────────────────────────────┘
Key histological features:
- Central caseous necrosis (eosinophilic amorphous material with ghost cell outlines)
- Epithelioid macrophages (elongated, pale, abundant pink cytoplasm; called "epithelioid" due to resemblance to epithelium)
- Langhans giant cells (multinucleated, nuclei at periphery in horseshoe pattern - distinguishes from foreign body giant cells where nuclei scattered centrally)
- Peripheral lymphocytic infiltrate
- Fibrosis at periphery (older lesions)
- AFB stain (Ziehl-Neelsen) may show red acid-fast bacilli (often scanty in primary TB)
Fate of Ghon Complex
Ghon Complex
↓
┌─────────────────────────────────────────────────────────┐
│ 1. HEALING (95%) - Fibrosis → Calcification → Ranke │
│ complex; bacilli remain dormant (latent TB) │
│ │
│ 2. REACTIVATION (later) - dormant bacilli reactivate │
│ → Secondary TB (apical lung disease) │
│ │
│ 3. PROGRESSIVE PRIMARY TB (5%, immunocompromised): │
│ a. Lobar pneumonia (consolidation) │
│ b. Caseous pneumonia (very bad prognosis) │
│ c. MILIARY TB - hematogenous spread → millet seed │
│ granulomas in all organs (lungs, liver, spleen, │
│ brain, kidney) │
│ d. TB meningitis (spread to meninges) │
│ e. Pleuritis (Ghon focus ruptures into pleura) │
│ f. TB lymphadenitis (spread to regional nodes) │
└─────────────────────────────────────────────────────────┘
LAQ SECTION
LAQ 1 - Inflammation: Full Answer
Definition of Inflammation
Inflammation is the local vascular and cellular response of a living tissue to injury, infection, or immunological stimuli. It is a protective mechanism designed to:
- Eliminate the initial cause of injury (pathogens, dead cells)
- Remove necrotic tissue
- Initiate tissue repair
"Inflammation is fundamentally a protective response; without it, infections would go unchecked and wounds would never heal." - Robbins
Cardinal Signs (5)
- Rubor (redness) - vasodilation → increased blood
- Calor (heat) - vasodilation + increased metabolism
- Tumor (swelling) - increased vascular permeability → exudation
- Dolor (pain) - bradykinin, PGE2, substance P
- Functio laesa (loss of function) - Virchow's addition
Types
- Acute Inflammation - rapid onset, short duration (hours-days), neutrophils predominant
- Chronic Inflammation - slow onset, prolonged, lymphocytes/macrophages/plasma cells
Acute Inflammation - Vascular Events (Detailed)
1. Immediate Transient Vasoconstriction (seconds):
- Neurogenic reflex; insignificant
2. Active Hyperemia (vasodilation):
- Mediators: Histamine (from mast cells), NO, PGE2, bradykinin, substance P
- Arterioles dilate → increased blood flow → redness (rubor) + heat (calor)
3. Increased Vascular Permeability (key event):
The principal mechanism is endothelial cell contraction creating interendothelial gaps (widening of tight junctions):
| Type | Mechanism | Duration | Mediators |
|---|
| Immediate transient | Endothelial contraction (reversible, venules only) | 15-30 min | Histamine, C3a, C5a, bradykinin |
| Delayed prolonged | Endothelial retraction (cytoskeletal reorganization) | 4-6 hrs to days | TNF, IL-1 |
| Immediate sustained | Direct endothelial damage → cell death | Hours | Burns, toxins |
| Leukocyte-mediated | Neutrophil products damage endothelium | Late | ROS, proteases |
| Transcytosis | Increased vesicular transport (VEGF-mediated) | Variable | VEGF |
Results:
- Exudate (high protein fluid) → edema (tumor)
- Loss of plasma volume → hemoconcentration
- Increased blood viscosity → stasis
Exudate vs Transudate:
| Feature | Exudate | Transudate |
|---|
| Mechanism | Increased permeability | Osmotic/hydrostatic imbalance |
| Protein content | >3 g/dL | <3 g/dL |
| Specific gravity | >1.020 | <1.012 |
| Cells | Many leukocytes | Few cells |
| LDH | High | Low |
4. Stasis:
- Slowing of blood flow → rouleaux of RBCs → leukocytes pushed peripherally (margination)
- Visible as vascular congestion (dark congested vessels)
5. Lymphatic Changes:
- Lymph flow increases (drains excess fluid)
- Lymphangitis (red streaks), lymphadenitis (tender lymph nodes) may develop
Acute Inflammation - Cellular Events (Detailed)
The full sequence: MARC→P→PHAGO
Margination → Rolling → Adhesion → Crawling → Paracellular transmigration → Chemotaxis → Phagocytosis
1. Margination:
- Slowing of blood → axial flow disturbed → leukocytes pushed to periphery
- Leukocytes "pavment" the endothelium
2. Rolling:
- Molecules: Selectins
- P-selectin: On endothelium (from Weibel-Palade bodies within minutes of histamine/thrombin stimulation); also on platelets
- E-selectin (CD62E): On endothelium (induced in 1-2 hrs by IL-1, TNF)
- L-selectin (CD62L): On leukocytes
- Bind sialyl-Lewis X (sLeX) moieties on mucin-like glycoproteins
- Leukocytes tumble and roll slowly along vessel wall
3. Firm Adhesion/Arrest:
- Molecules: Integrins
- LFA-1 (CD11a/CD18, αLβ2) on leukocytes binds ICAM-1 on endothelium
- Mac-1 (CD11b/CD18, αMβ2) on monocytes/macrophages binds ICAM-1
- VLA-4 (α4β1) on monocytes binds VCAM-1 on endothelium
- Integrins are in low-affinity state normally; chemokines (IL-8) rapidly convert to high-affinity state via G-protein signaling → firm arrest
4. Transmigration (Diapedesis):
- Leukocyte squeezes through interendothelial junctions (paracellular route)
- Key molecule: PECAM-1 (CD31) - expressed on both leukocytes and endothelium
- Homotypic PECAM-1 interaction facilitates passage
- Leukocyte then secretes collagenases to cross the basement membrane
- Transcellular route (through endothelium) also possible
5. Chemotaxis:
- Directed migration up concentration gradient of chemoattractants
- Best chemoattractants: C5a, LTB4, IL-8, fMLP (bacterial N-formyl peptides)
- Mechanism: chemoattractant binds GPCR → phospholipase C → IP3 + DAG → Ca²⁺ release → actin polymerization at leading edge (pseudopod)
6. Phagocytosis (see SAQ 2 above)
7. Leukocyte Sequencing:
- Neutrophils predominate 0-24 hours (first responders: short-lived, 6-24h in tissue)
- Monocytes/Macrophages predominate 24-48 hours (long-lived, secrete growth factors)
- Exceptions: Viral infections → lymphocytes first; Eosinophilic → eosinophils; Pseudomonas → neutrophils persist
LAQ 2 - Healing of Simple Fracture of Bone + Complications
Healing of Simple Fracture of Bone
Bone has a unique ability to regenerate (not just repair), restoring original structure if healing proceeds normally.
Stages (6 Stages)
Stage 1 - Hematoma Formation (Hours-Days):
- Fracture ruptures blood vessels in periosteum, Haversian canals, and surrounding soft tissue
- Blood fills fracture gap → fracture hematoma (organizing, provides scaffold)
- Inflammatory mediators released → local vasodilation, edema, pain
- Fibrin network forms temporary scaffold
- Critical point: Hematoma must NOT be evacuated - it is essential for healing
Stage 2 - Procallus (Soft Callus) Formation (Days 1-2 weeks):
- Periosteal cambium layer is the main source of new bone-forming cells
- Fibroblasts and chondroblasts invade hematoma → fibrocartilaginous soft callus
- New capillaries invade the area
- Soft callus converts hematoma → fibrocartilage tissue (rubbery, palpable)
- Osteoclasts appear and begin resorbing dead bone ends
Stage 3 - Hard Callus (Woven Bone Callus) (2-6 weeks):
- Osteoblasts differentiate (from cambium layer, endosteum, bone marrow stromal cells)
- Endochondral ossification converts cartilage → woven bone
- Intramembranous ossification from periosteum forms primary callus
- Hard, mineralized callus replaces soft callus
- X-ray visible as fuzzy mineralized area around fracture
- Callus is larger than original bone (fusiform)
Stage 4 - Consolidation (Months):
- Woven bone is gradually replaced by lamellar bone (stronger, organized)
- Remodeling by coordinated osteoclast/osteoblast activity
- Fracture line may still be visible on X-ray
Stage 5 - Remodeling (Months to Years):
- Final restoration of original cortical architecture
- Wolff's Law: Bone remodels in response to mechanical stress
- Medullary cavity re-established
- Callus gradually resorbed (Haversian systems restored)
- Final result: virtually indistinguishable from original bone (in children, even angulation can remodel)
FRACTURE HEALING STAGES DIAGRAM:
Day 0: |BONE|====|BONE| ← fracture + hematoma
Days 1-7: |BONE|xxxx|BONE| ← fibrocartilaginous soft callus
Weeks 2-6:|BONE|####|BONE| ← hard bony callus (woven bone)
(callus larger than bone)
Months: |BONE|=====|BONE| ← lamellar bone remodeling
Final: |BONE======|BONE| ← restored cortex + medullary canal
Cells involved:
- Periosteal cambium cells → osteoblasts (primary source)
- Endosteal cells → osteoblasts
- Bone marrow stromal cells → osteoprogenitor cells
- Osteoclasts → bone resorption/remodeling
- Chondroblasts → temporary cartilage in soft callus
Growth factors/mediators:
- BMP (Bone Morphogenetic Proteins) - most important for osteogenesis
- TGF-β, IGF, PDGF, FGF
- PTH - stimulates bone turnover
- Prostaglandins - early stimulation
Complications of Fracture Healing
Early Complications:
- Non-union - fracture fails to unite (interposed soft tissue, poor blood supply, infection, movement)
- Delayed union - union occurs but takes longer than expected
Late Complications:
| Complication | Description |
|---|
| Malunion | Bones unite in wrong position (angulation/rotation) → deformity |
| Non-union | Fibrous union or pseudoarthrosis (false joint forms) |
| Avascular necrosis | Head of femur (subcapital fracture), scaphoid, talus - vessels torn at fracture |
| Infection (osteomyelitis) | Open fractures, post-operative; Staph aureus most common |
| Myositis ossificans | Ectopic bone in muscle near fracture site (esp. elbow) |
| Compartment syndrome | Swelling → compression of compartment → muscle necrosis |
| Volkmann's ischemic contracture | Result of compartment syndrome (forearm) |
| Sudeck's atrophy | Reflex sympathetic dystrophy; patchy osteoporosis, pain |
| Joint stiffness | Prolonged immobilization → periarticular fibrosis |
| Post-traumatic arthritis | Intraarticular fracture → joint damage → osteoarthritis |
| Fat embolism | Marrow fat released → lungs, brain → respiratory failure, confusion |
| Growth disturbance | Epiphyseal injury in children → limb length discrepancy |
LAQ 3 - Regeneration and Repair + Factors Affecting Wound Healing + Healing of Fracture
Regeneration and Repair - Concepts
After any injury, the body must restore tissue integrity. Two processes occur:
Regeneration: Replacement of lost tissue with cells of the same type - complete restoration of structure and function. Possible only in labile and stable cells.
Repair (Fibrosis): Replacement of lost tissue with scar tissue (collagen) - incomplete structural restoration. Occurs in permanent cells or when ECM framework is destroyed.
Cell Types and Regenerative Capacity
| Cell Type | Division | Examples | Healing |
|---|
| Labile cells | Divide throughout life (cycling cells) | Epidermis, GI mucosa, hematopoietic cells, testicular germinal cells | Regenerate completely |
| Stable cells | Normally quiescent (G0); can re-enter cell cycle with stimulus | Hepatocytes, renal tubular cells, smooth muscle, fibroblasts, pancreatic exocrine cells | Regenerate if ECM scaffold intact |
| Permanent cells | Cannot divide (terminally differentiated) | Neurons, cardiac myocytes, skeletal muscle | Cannot regenerate; heal by scar |
Process of Repair (Sequence of Events)
After an injury that exceeds regenerative capacity, a sequence of events occurs:
1. Hemostasis (seconds-minutes):
- Platelet plug → fibrin clot (provisional matrix)
- Platelets release PDGF, TGF-β → stimulate repair
2. Inflammatory Phase (0-5 days):
- Neutrophils debride wound (0-48 hrs)
- Macrophages replace neutrophils (Day 2 onwards) - "command cells" of healing
- Macrophages secrete: VEGF, TGF-β, PDGF, TNF, IL-1
- Without macrophages, healing is severely impaired
3. Proliferative Phase (Days 3 - Week 3):
Three subprocesses run simultaneously:
- Angiogenesis: VEGF → endothelial sprouting → new capillaries
- Fibroplasia: TGF-β + PDGF → fibroblast migration and proliferation → collagen synthesis
- Type III collagen (reticulin) synthesized first → later replaced by Type I
- Collagen cross-linking requires Vitamin C (hydroxylation of proline/lysine)
- Re-epithelialization: EGF, TGF-α → basal keratinocytes migrate over wound bed
4. Remodeling Phase (Week 3 - Year 1):
- Matrix metalloproteinases (MMPs) remodel collagen
- Granulation tissue replaced by scar
- Type III collagen → Type I collagen (stronger)
- Scar matures: avascular, acellular, predominantly type I collagen
- Tensile strength:
- Week 1: 10% of normal
- Month 1: 40%
- Month 3: 70-80%
- Maximum: 80-85% (never 100%)
REPAIR PROCESS DIAGRAM:
Injury
↓ [Seconds]
Hemostasis (fibrin clot, platelet plug)
↓ [Hours]
Acute Inflammation (neutrophils debride)
↓ [Day 2]
Macrophage influx (secrete growth factors)
↓ [Day 3-5]
Granulation Tissue (VEGF→ angiogenesis + TGF-β→ fibroplasia)
↓ [Week 1-3]
Re-epithelialization (EGF, TGF-α → keratinocytes migrate)
↓ [Week 3 onwards]
Remodeling (Type III → Type I collagen; MMP activity)
↓ [Months]
MATURE SCAR (acellular, avascular, 80% tensile strength)
Factors Affecting Wound Healing (Complete Enumeration)
(See SAQ 1 for complete details)
Mnemonic: "DIVAS of wound healing"
Diabetes, Infection, Vitamin deficiency, Age/Anemia, Steroids + all other local/systemic factors listed in SAQ 1
Summary - Comparison of Types of Healing
| Feature | Primary Intention | Secondary Intention | Fracture |
|---|
| Tissue type | Skin | Skin/mucosa | Bone |
| Tissue defect | Minimal | Large | Variable |
| Granulation tissue | Little | Abundant | Fibrocartilage callus |
| Contraction | Minimal | Marked | Not applicable |
| Scar | Thin | Thick | Remodeled to normal |
| Regeneration | Partial | Partial | Complete |
| Mediators | TGF-β, PDGF, VEGF | TGF-β, PDGF, VEGF | BMP, TGF-β, PDGF, FGF |
Key Images for Reference
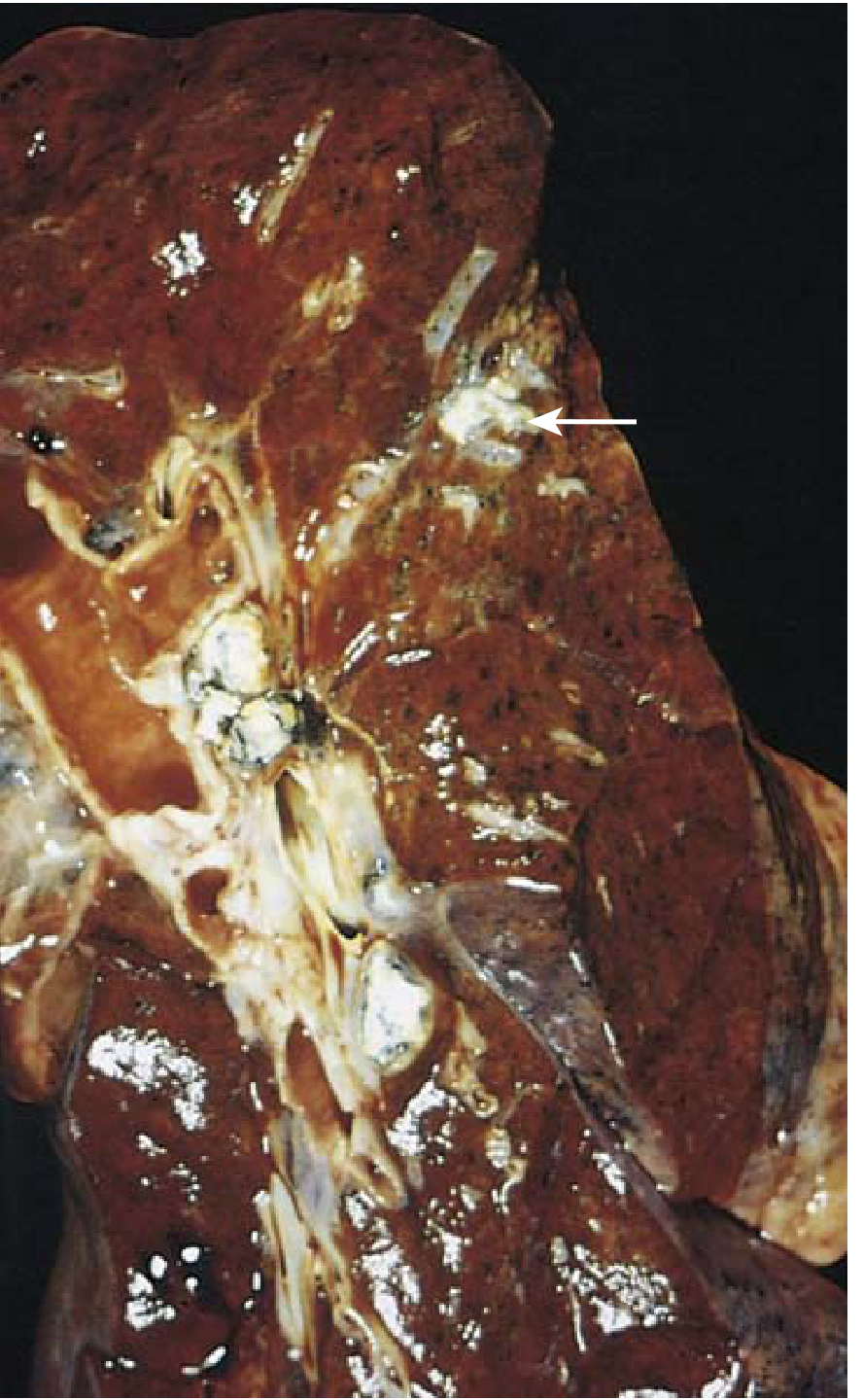
Ghon Complex (Gross):
Gross specimen - lung with Ghon focus (arrow = caseous white lesion in parenchyma with associated hilar node involvement) - Robbins & Kumar Basic Pathology
Exudate vs Transudate (Vascular changes):
Vascular changes in acute inflammation - formation of exudate - Robbins & Kumar Basic Pathology
Arachidonic Acid Pathway (Chemical Mediators):
Prostaglandins and Leukotrienes - the two major arms of arachidonic acid metabolism - Robbins & Kumar Basic Pathology
Quick Revision - High-Yield Points for MUHS Exam
Most tested facts:
- Vasodilation mediator: Histamine (main early), NO, PGE2
- Most important chemotaxis: C5a > LTB4 > IL-8 > fMLP
- Most important opsonin: IgG (Fc portion) + C3b
- Phagocyte killing: NADPH oxidase → O₂⁻ → H₂O₂ → HOCl (myeloperoxidase)
- CGD: NADPH oxidase deficiency; can't make respiratory burst
- First leukocyte at injury: Neutrophil (0-24 hrs)
- First collagen in healing: Type III (reticulin) → later Type I
- Tensile strength: 80-85% maximum (never 100%)
- Keloid vs Hypertrophic: Keloid extends beyond wound margins; more in dark skin
- Ghon complex: Ghon focus + lymphangitis + hilar lymphadenitis
- Ranke complex: Calcified Ghon complex (on X-ray)
- Virchow cell: Foamy macrophage in lepromatous leprosy (hallmark)
- Grenz zone: Normal dermis between epidermis and LL infiltrate
- Lepromin test: Positive in TT; Negative in LL
- Langhans giant cell: Nuclei at periphery (horseshoe) - TB; NOT Langerhans cell (skin DC)
- Best fracture healing: Periosteal cambium cells + BMP
- Soft callus type: Fibrocartilage
- Hard callus type: Woven bone (replaced by lamellar bone in remodeling)
Sources: Robbins & Kumar Basic Pathology (10th ed.), Robbins & Cotran Pathologic Basis of Disease (10th ed.), Andrews' Diseases of the Skin