Eras protocols for major abdominal surgeries, and role of opioid vs non opioid analgesics
Reading File
Finding Sources
Finding Sources
Searching PubMed
"enhanced recovery after surgery" AND "abdominal surgery" AND analgesia
Finding Sources
Reading File
Reading File
Reading File
Searching PubMed
"ERAS" AND "opioid-free" AND "colorectal surgery"
Reading File
Reading File
Finding Sources
Searching PubMed
ERAS protocol AND "multimodal analgesia" AND "postoperative pain"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching the Web
ERAS Society guidelines 2024 colorectal surgery major abdominal opioid-sparing analgesia recommendations
I now have thorough material from multiple authoritative sources. Let me compose the comprehensive answer.
ERAS Protocols for Major Abdominal Surgery & the Role of Opioid vs. Non-Opioid Analgesics
1. What is ERAS and Why Does it Work?
Enhanced Recovery After Surgery (ERAS) is an evidence-based, multimodal, multidisciplinary perioperative care program designed to attenuate the surgical stress response, reduce catabolism, and accelerate return to normal function. It was pioneered by Henrik Kehlet in the 1990s, initially in colorectal surgery, and has since been extended to hepatobiliary, upper GI, gynecologic, urologic, bariatric, thoracic, and cardiac surgery.
The core physiological rationale is modulating the surgical stress response:
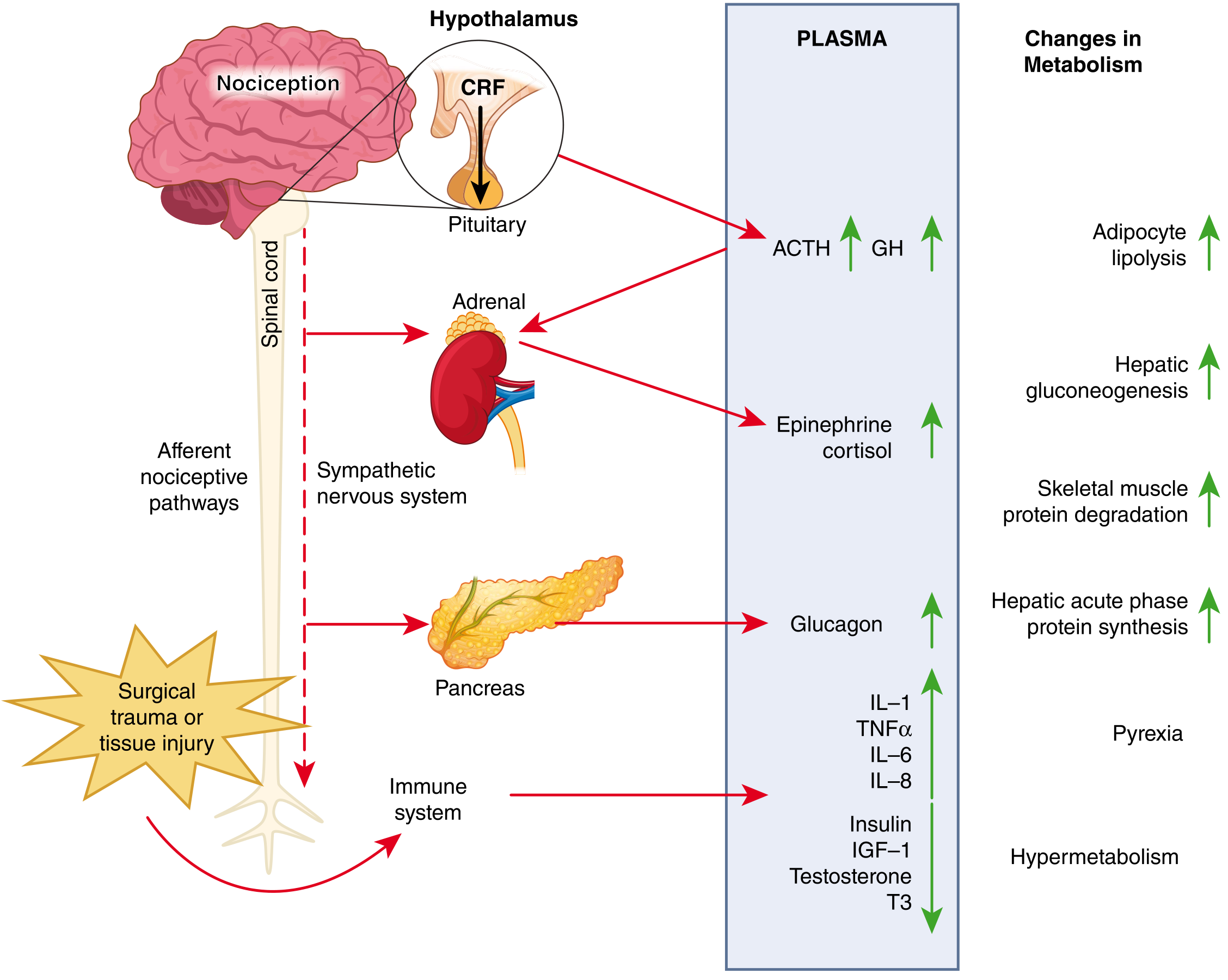
Figure: Surgical trauma activates afferent nociceptive pathways triggering the hypothalamus-pituitary-adrenal axis and sympathetic nervous system, releasing catecholamines, cortisol, and glucagon, while the immune system releases IL-1, TNF-alpha, IL-6, and IL-8 - collectively producing insulin resistance, catabolism, pyrexia, and hypermetabolism. ERAS targets each of these pathways. (Sabiston Textbook of Surgery, Fig 22.4)
ERAS works because it is a bundle - no single element is magic; it is the combined effect of multiple simultaneous interventions that produces benefit. Key outcomes include:
- Up to 50% reduction in complication rates in colorectal surgery (Varadhan meta-analysis)
- Reduced length of stay, readmissions, and mortality
- Cost savings of $1,000-$8,700 per patient depending on surgery type
- 42% improved 5-year survival in high-compliance ERAS colorectal patients
2. The Three Phases of ERAS: Key Elements
A. Preoperative Phase
| Element | Rationale |
|---|---|
| Patient education/prehabilitation | Reduces anxiety, sets expectations, improves compliance |
| Carbohydrate loading (clear carb drink up to 2h preop) | Raises insulin sensitivity by 50%, reduces postop insulin resistance |
| Fasting modification - solids allowed until 6h, clear fluids until 2h | Replaces outdated NPO-from-midnight rules |
| Nutritional optimization - correct malnutrition preop | Reduces wound healing complications |
| Smoking/alcohol cessation | Reduces pulmonary and wound complications |
| Avoidance of routine mechanical bowel preparation | MBP is not evidence-based; causes hypovolemia, electrolyte disturbance |
| Antibiotic prophylaxis within 60 min of incision | Reduces SSI |
| VTE prophylaxis before anesthesia induction | LMWH + TED stockings |
| Epidural/spinal anesthesia placement (for open major abdominal surgery) | Reduces cortisol/adrenaline release; provides superior analgesia pre-emptively |
| Corticosteroids (e.g., dexamethasone 8mg IV) | Reduces PONV and inflammatory response |
B. Intraoperative Phase
| Element | Rationale |
|---|---|
| Minimally invasive surgery (laparoscopic/robotic) when feasible | Lower inflammatory mediators, faster functional recovery, better pain control |
| Multimodal opioid-sparing anesthesia | Short-acting drugs (propofol, remifentanil), non-opioid adjuncts |
| TIVA (Total IV Anesthesia) with propofol | Reduces PONV vs. volatile agents; possible oncologic benefit |
| Goal-directed fluid therapy | Balanced crystalloid; avoid over-resuscitation causing gut edema and delayed return of bowel function; use hemodynamic monitoring (stroke volume variation, pulse contour) |
| Normovolemia/avoidance of salt and water excess | Excessive IV NaCl causes tissue edema, impairs anastomotic integrity |
| Active temperature maintenance | Normothermia; hypothermia impairs coagulation, increases SSI risk |
| Avoidance of routine drains and NG tubes | Drains and NG tubes delay mobility and oral intake |
| Anesthetic adjuncts: ketamine, lidocaine IV infusion, magnesium, dexmedetomidine, beta-blockers | Multimodal antinociception; reduce intraoperative opioid requirements |
| Depth of anesthesia monitoring (BIS) | Especially in elderly; prevents cognitive dysfunction and delirium |
C. Postoperative Phase
| Element | Rationale |
|---|---|
| Early oral feeding - solids as early as 4h post bowel surgery | Accelerates GI recovery; delay increases infection and prolongs recovery |
| Multimodal opioid-sparing analgesia | Central tenet (detailed below) |
| Early mobilization - within 30 min of PACU arrival | Out of bed within hours; 6h/day upright from POD1 |
| Avoid routine NG tubes | NG decompression only for refractory ileus |
| Remove urinary catheter within 24h | Reduces UTI, enables mobilization |
| PONV prophylaxis - multimodal (ondansetron + dexamethasone ± droperidol) | PONV delays discharge and oral intake |
| Gum chewing (3-4×/day, sugar-free, ≥10 min) | Cochrane review: earlier return of bowel sounds, flatus, and bowel movements |
| Preset discharge criteria | Tolerating solid food ×3 meals, passed flatus/stool, oral analgesia adequate, low VAS pain score |
| Follow-up at 30 days | Audit for complications; essential for ERAS quality improvement |
| Alvimopan (peripherally acting µ-opioid antagonist) | For open colonic resection; counteracts opioid-induced ileus without reversing analgesia |
3. Opioid vs. Non-Opioid Analgesia in ERAS - The Central Debate
"A central tenet of ERAS is multimodal opioid-sparing postoperative analgesia. Historically, opioids were the cornerstone of pain management in the postoperative period; however, there are growing concerns related to the risk of patients developing dependence on opioids during the postoperative period and ultimately becoming chronic users."
- Sabiston Textbook of Surgery, p. 379
Why Minimize Opioids?
- Postoperative ileus (POI): Opioids bind peripheral µ-receptors in the gut wall, inhibiting GI motility. This is the dominant mechanism of POI after abdominal surgery, directly extending hospital stay.
- Opioid dependence and the opioid crisis: 50% of patients report not filling their opioid prescriptions post-surgery, yet inappropriate prescribing by surgeons has contributed heavily to North America's opioid epidemic.
- Dose-dependent side effects: PONV, sedation, urinary retention, respiratory depression, sleep disturbance - all of which conflict with ERAS goals of early mobilization and oral intake.
Multimodal Analgesic Strategy
Multimodal analgesia combines two or more drugs acting at different points on the pain pathway, achieving synergistic or additive effects that reduce the required dose of each agent and minimize side effects.
Non-Opioid Analgesics in ERAS
1. Acetaminophen (Paracetamol)
- Often underestimated; provides sustained and equivalent analgesia compared with other perioperative analgesics when given regularly
- Can be given orally, rectally, or IV
- Opioid-sparing effect is inconsistent across studies, but its high safety profile makes it a routine ERAS component
- Administered on a scheduled basis (not PRN) - critical distinction
2. NSAIDs / COX-2 Inhibitors
- Provide anti-inflammatory, antipyretic, and analgesic effects
- Nonselective (ibuprofen, naproxen, diclofenac, ketorolac) inhibit COX-1 and COX-2
- Selective (celecoxib) inhibit mainly COX-2 with fewer GI and platelet effects
- Meta-analyses: IV diclofenac and ketorolac give good postoperative pain relief
- Important caveat: observational studies raised concern about anastomotic leakage with COX-2 inhibitors; one meta-analysis found no significant risk with ≤48h use, but risk may be elevated with >3 days of use or in emergency colorectal surgery
- Use with caution in: peptic ulcer disease, bleeding risk, CVD, renal/hepatic impairment
3. Thoracic Epidural Analgesia (TEA)
- Gold standard for open major abdominal surgery (colorectal, hepatic, esophageal, gastric)
- Placed at T7-T10; when covering T10 dermatome, it blunts adrenal catecholamine and cortisol release, directly reducing insulin resistance
- Provides excellent pain relief with minimal or no systemic opioids
- Supports return of bowel function by blocking sympathetic efferents to the gut
- Drawbacks: hypotension (may require vasopressors), failure rates up to 30%, contraindicated in coagulopathy
- For laparoscopic surgery, TEA benefit is less clear - abdominal wall blocks may be preferred
4. Transversus Abdominis Plane (TAP) Block
- Ultrasound-guided injection of local anesthetic (bupivacaine, ropivacaine) into the neurofascial plane between internal oblique and transversus abdominis
- Effective for somatic pain of abdominal wall incision
- TAP blocks performed before surgery appear to provide better analgesia than post-closure blocks
- Associated with decreased length of stay vs. systemic opioids in laparoscopic colorectal surgery
- Liposomal bupivacaine (extended-release) formulations show promising results
5. IV Lidocaine Infusion
- Systemic IV lidocaine (1-1.5 mg/kg/h) has anti-inflammatory and analgesic properties
- Reduces postoperative pain scores, opioid consumption, and time to first bowel movement
- Considered an alternative when neuraxial/regional techniques are not feasible
6. Ketamine (Sub-anesthetic doses)
- N-methyl-D-aspartate (NMDA) receptor antagonist
- Prevents central sensitization ("windup")
- Used intraoperatively (0.1-0.5 mg/kg bolus) or as low-dose infusion (0.1-0.2 mg/kg/h)
- Recent systematic review (PMID 41814842, 2026) confirms perioperative ketamine/esketamine supports ERAS goals
- Particularly useful in opioid-tolerant patients
7. Dexamethasone
- Dual role: PONV prophylaxis + analgesic (reduces peripheral inflammation)
- Single dose 8mg IV preoperatively is standard ERAS practice
8. Magnesium
- NMDA antagonist; reduces opioid consumption perioperatively
- Often given as IV infusion intraoperatively
9. Dexmedetomidine / Clonidine
- Alpha-2 agonists; reduce opioid requirements and sympathetic activation
- Dexmedetomidine useful for sedation without respiratory depression in PACU
10. Neuraxial (Intrathecal) Opioids
- Single-shot intrathecal morphine (0.1-0.3 mg) provides 12-24h of excellent visceral analgesia
- Lower doses than systemic opioids; avoids ileus better than IV opioids
- Respiratory depression risk - requires monitoring
- Used where epidural catheter is not practical
Role of Opioids in ERAS
Opioids are not eliminated from ERAS - they are rationalized:
- Short-acting intraoperative opioids (fentanyl, remifentanil, sufentanil) are still used for intraoperative nociception but at the lowest effective dose
- Patient-controlled analgesia (PCA) with IV morphine or hydromorphone serves as rescue for breakthrough pain
- Oral opioids (oxycodone, tramadol) are used as step-down after multimodal non-opioid therapy is maximized
- The goal is opioid sparing, not opioid elimination - most ERAS protocols prescribe opioids PRN as rescue only, not scheduled
4. Surgery-Specific ERAS Highlights
| Surgery | Key ERAS Analgesic Features |
|---|---|
| Colorectal | TEA preferred for open; TAP block for laparoscopic; alvimopan if opioids used intraoperatively |
| Liver resection | TEA avoided if coagulopathy (common); TAP + IV lidocaine + acetaminophen + NSAIDs preferred |
| Pancreatic | TEA strongly recommended for open Whipple; compliance >80% linked to reduced mortality |
| Esophageal | TEA + multimodal; early enteral feeding via jejunostomy |
| Gastric | Epidural or TAP; strict fluid restriction; early NGT removal |
| Bariatric | IV ketamine + TAP + acetaminophen; NSAIDs used cautiously; opioids minimized due to OSA risk |
5. ERAS Outcomes Evidence
- Colorectal surgery (Varadhan meta-analysis): Complication rates reduced by up to 50% with ERAS compliance
- Liver surgery RCT meta-analysis: Significantly reduced morbidity, faster functional recovery, shorter LOS
- Pancreatic surgery: >80% ERAS compliance associated with significantly reduced mortality and major complications
- Esophageal, gastric, bariatric surgery: Similar benefits confirmed
6. Recent Evidence Updates (PubMed, 2024-2026)
- Perioperative Ketamine/Esketamine for ERAS (PMID 41814842, J Invest Surg 2026): Systematic review confirms ketamine and esketamine support opioid-sparing goals within ERAS pathways
- Ketamine in Bariatric Surgery Multimodal Analgesia (PMID 41840313, Obes Surg 2026): Meta-analysis of RCTs confirms opioid-sparing benefits in bariatric ERAS
- The ERAS Society published updated colorectal surgery guidelines in 2024 (available open-access via erasociety.org)
- The 2026 ASA Practice Guideline on Perioperative Pain Management reinforces fascial plane blocks and regional techniques for abdominal surgery, showing moderate-quality evidence for reduced pain intensity and opioid consumption
Key Takeaway
ERAS is a bundle of care, not a single intervention. Its analgesic strategy rests on:
- Pre-emptive neuraxial blockade (TEA for open surgery) to blunt the neuroendocrine stress response
- Scheduled non-opioid baseline analgesia (acetaminophen + NSAID/COX-2 inhibitor)
- Targeted regional techniques (TAP block, wound infiltration, IV lidocaine)
- Opioid adjuncts (ketamine, magnesium, dexmedetomidine) to minimize dose
- Opioids only as rescue/PRN - not scheduled first-line
This multi-layered approach shortens ileus, enables earlier oral intake and mobilization, reduces side effects, and ultimately shortens hospital stay while improving safety.
Sources: Sabiston Textbook of Surgery (9780443124341), Miller's Anesthesia 10e (9780323935920), Sleisenger & Fordtran's GI and Liver Disease (9780323609623), Current Surgical Therapy 14e (9780323796835), Morgan & Mikhail's Clinical Anesthesiology 7e; PubMed PMIDs 41814842, 41840313; ERAS Society 2024 Colorectal Guidelines
This is a shared conversation. Sign in to Orris to start your own chat.