What's antral mycosa in nose
Reading File
Finding Sources
Searching the Web
antral mucosa nose maxillary sinus anatomy
Finding Sources
Reading File
Here is a clear explanation of antral mucosa in the context of the nose:
Antral Mucosa
"Antral" refers to the antrum - specifically the maxillary antrum (also called the antrum of Highmore), which is the medical name for the maxillary sinus. The maxillary sinus is the largest of the four paired paranasal sinuses and sits within the cheekbones on either side of the nose.
Antral mucosa, therefore, is the mucous membrane lining the inside of the maxillary sinus.
Structure of Antral Mucosa
The antral mucosa is made up of:
- Ciliated pseudostratified columnar (respiratory) epithelium - the same type that lines the nasal cavity
- Goblet cells scattered among the epithelial cells, which produce mucus
- A thin lamina propria (connective tissue layer) beneath the epithelium
- Submucosal glands that contribute to mucus secretion
Compared to the nasal cavity mucosa, the antral mucosa is considerably thinner and less vascular.
Function
- The cilia beat in coordinated waves to transport mucus toward the maxillary ostium (the natural opening of the sinus), which drains into the middle meatus of the nasal cavity
- Mucus traps pathogens, dust, and debris
- The lining helps humidify and warm inhaled air passing through the sinuses
Clinical Relevance
- Sinusitis (rhinosinusitis): Inflammation of the antral mucosa is the hallmark of maxillary sinusitis. When the ostium becomes blocked, mucus builds up, bacteria grow, and the mucosa becomes swollen and inflamed
- Antral mucosa thickening: Seen on CT/X-ray as a sign of chronic maxillary sinusitis
- Mucosal stripping: In older surgical procedures (Caldwell-Luc surgery), the antral mucosa was sometimes stripped - this is now avoided because it can cause mucociliary dysfunction. Modern endoscopic sinus surgery (FESS) aims to preserve the mucosa
- TNM staging of maxillary sinus tumors: T1 is specifically defined as a tumor "limited to the antral mucosa with no erosion or destruction of bone" - so the term appears in cancer staging as well (Scott-Brown's Otorhinolaryngology)
In short: antral mucosa = the mucous lining inside your maxillary (cheekbone) sinus. It keeps the sinus clean via ciliary action, and when it becomes inflamed or diseased, it leads to sinusitis or, rarely, sinonasal tumors.
Lupus pernio
Reading File
Finding Sources
Finding Sources
Searching the Web
lupus pernio sarcoidosis clinical features diagnosis treatment
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information. Here is a thorough answer:
Lupus Pernio

Definition
Lupus pernio is a specific cutaneous manifestation of sarcoidosis - NOT lupus erythematosus and NOT a cold injury (pernio/chilblain). The name is a historical misnomer coined by Besnier in the 19th century, who incorrectly thought the lesions were related to lupus vulgaris (cutaneous TB) and cold injury. It is one of the most clinically significant forms of cutaneous sarcoidosis because of its strong association with systemic disease.
Epidemiology
- More common in women, typically in the 4th or 5th decade
- Higher prevalence in Black patients
- Occurs in approximately 25% of patients with sarcoidosis (cutaneous sarcoidosis overall); lupus pernio is a subset
Clinical Features
Skin lesions:
- Brown to violaceous (red-purple), smooth, shiny, indurated plaques and nodules
- Classically symmetric distribution on:
- Tip and alar rim of the nose (most characteristic)
- Cheeks, lips, forehead
- Earlobes
- Digits (fingers)
- Can be very disfiguring
- Lesions rarely resolve spontaneously
- May mimic rhinophyma (rosacea-related nose enlargement)
On diascopy (pressing a glass slide on the skin): Shows "apple-jelly" yellow-brown coloration, reflecting granulomatous nature.
Associated Systemic Involvement (Key Associations)
Lupus pernio is a strong predictor of chronic, multisystem sarcoidosis:
| Association | Frequency |
|---|---|
| Chronic fibrotic pulmonary involvement | ~75% |
| Sinus (paranasal) sarcoidosis | ~50% |
| Upper respiratory tract involvement | ~50% |
| Bone granulomas (punched-out cysts, fingers) | ~43% |
| Chronic ocular lesions | ~37% |
- Nasal mucosal and underlying bone involvement can cause nasal perforation and collapse of the nasal bridge, resembling granulomatosis with polyangiitis (GPA/Wegener's)
- ENT evaluation is always recommended
- Associated with chronic rather than acute sarcoidosis (unlike erythema nodosum, which marks acute/benign disease)
Other Named Sarcoidosis Syndromes (Comparison)
| Syndrome | Features |
|---|---|
| Lupus pernio | Symmetric violaceous plaques on nose, earlobes, cheeks, digits |
| Lofgren syndrome | Erythema nodosum + bilateral hilar adenopathy + arthralgia + fever; acute, good prognosis |
| Heerfordt syndrome | Fever + parotid enlargement + facial palsy + anterior uveitis |
| Darier-Roussy sarcoid | Subcutaneous nodules on extremities |
| Mikulicz syndrome | Granulomas in mucosa/tongue + bilateral lacrimal/parotid/salivary gland enlargement |
Histopathology
Skin biopsy shows non-caseating (naked) epithelioid granulomas in the dermis - the hallmark of sarcoidosis. "Naked" means minimal surrounding lymphocytic infiltrate. There is no central necrosis (unlike TB granulomas).
Diagnosis
Requires all three:
- Compatible clinical and radiologic presentation
- Histologic evidence of non-caseating granulomas on skin biopsy
- Exclusion of other granulomatous conditions (TB, fungal infection, GPA, foreign body reaction)
Workup at diagnosis: chest X-ray/CT, pulmonary function tests, serum ACE, calcium, LFTs, ophthalmology referral, ENT evaluation.
Treatment
- Corticosteroids (oral or intralesional) are first-line - lead to recovery or regression in most patients
- Hydroxychloroquine (antimalarial) - for skin-limited disease
- Methotrexate - for chronic, refractory cases (though caution: can cause ulceration in sarcoidosis skin lesions)
- Tumor necrosis factor (TNF) inhibitors (infliximab, adalimumab) - for severe, refractory disease
- Important caution: Laser treatment (even pulsed dye laser) can cause ulceration of lupus pernio lesions and should be avoided
Prognosis
Lupus pernio follows a chronic, recalcitrant course and is one of the forms of cutaneous sarcoidosis that rarely remits spontaneously. Because of its strong link to pulmonary fibrosis and upper airway disease, long-term systemic monitoring is essential.
- Andrews' Diseases of the Skin, p. 824
- Fitzpatrick's Dermatology, p. 602-603
- Harrison's Principles of Internal Medicine 22E
Explain antrochoanal polyp
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Searching the Web
antrochoanal polyp pathogenesis dumbbell shape posterior fontanelle
Excellent. I now have comprehensive textbook and imaging data. Here is the full explanation:
Antrochoanal Polyp (ACP)
What Is It?
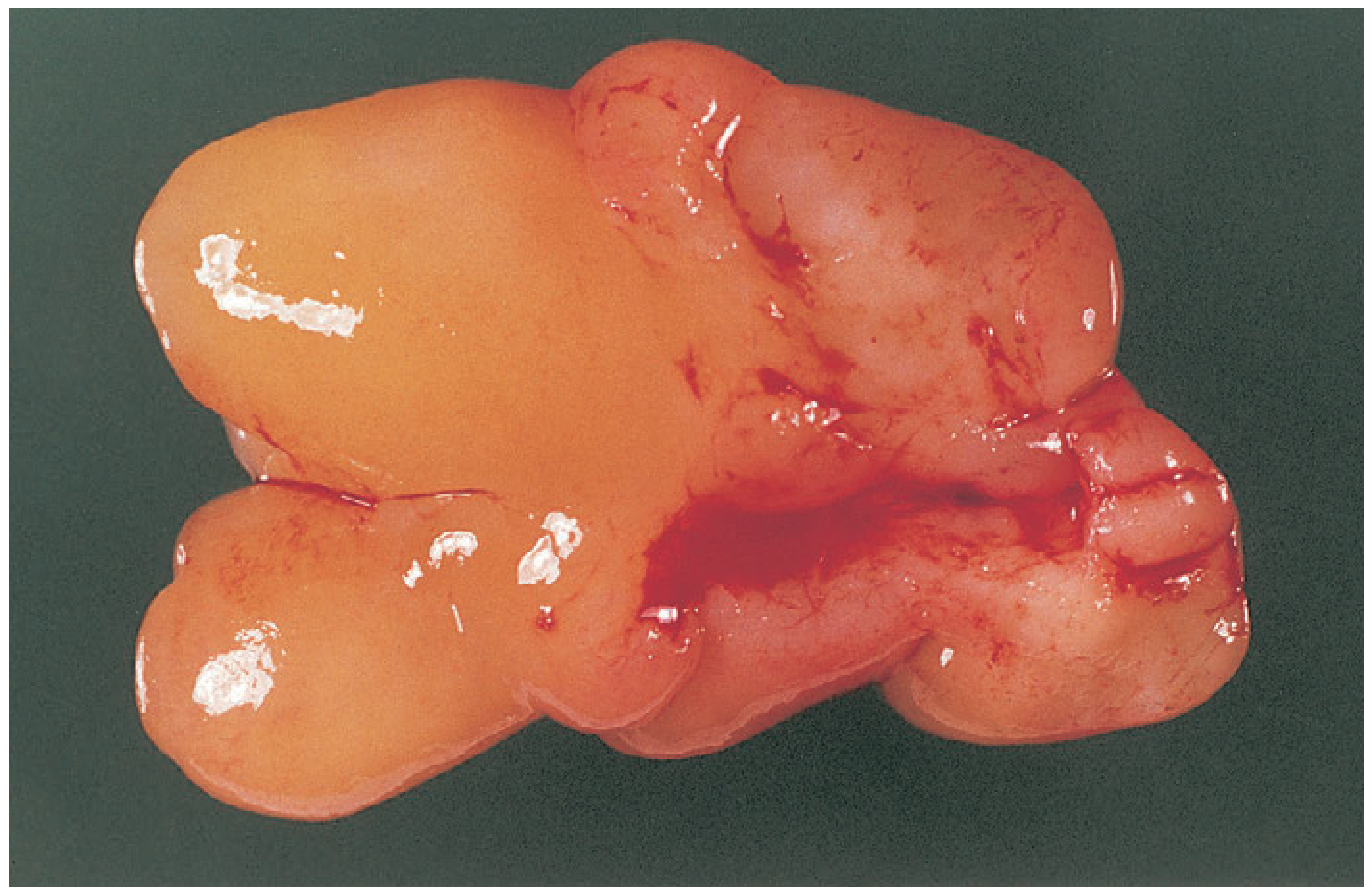
An antrochoanal polyp is a solitary, benign, unilateral mucosal polyp that originates in the maxillary antrum (sinus), passes through the sinus ostium, fills the nasal cavity, and extends posteriorly through the choana into the nasopharynx - sometimes reaching even the oropharynx.
The name describes its path: antrum (maxillary sinus) → nasal cavity → choana (the posterior opening of the nasal cavity into the nasopharynx).
The Characteristic "Dumbbell" Shape
A defining anatomical feature: the polyp has three components connected through a narrow waist at the sinus ostium:
| Component | Location |
|---|---|
| Antral (cystic) | Fills the maxillary sinus - usually cystic/fluid-filled |
| Nasal | Passes through the ostium into the nasal cavity - usually solid |
| Nasopharyngeal (choanal) | Extends through the choana into the nasopharynx - solid |
This gives it a classic dumbbell shape on imaging. The cystic antral portion exits through either the natural maxillary ostium or, more commonly, the posterior fontanelle (an area of thin mucosa in the medial wall of the maxillary sinus, lacking bony support).
Gross Appearance - Specimen
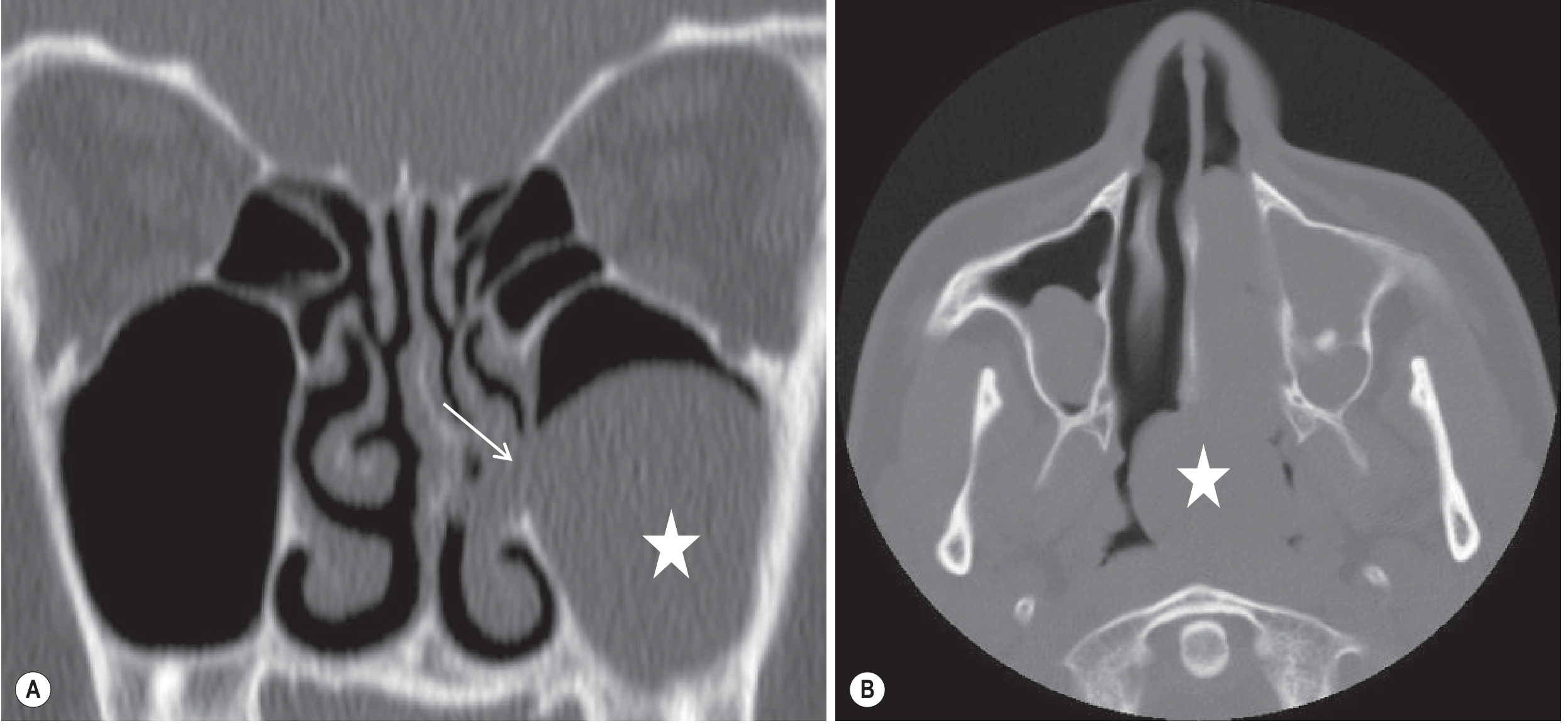
CT Imaging
Epidemiology
- Represents only ~4-6% of all nasal polyps
- Most common in young adults (3rd-5th decade), but also seen in children/adolescents
- More common in non-allergic patients (contrast with ethmoidal polyps, which are allergy-driven)
- Females slightly > males
- Always unilateral and solitary
Pathogenesis
The exact cause is not fully understood. Proposed theories include:
- Infection theory - chronic low-grade maxillary sinus infection triggers mucosal oedema and polyp formation (infection plays a bigger role than in ethmoidal polyps)
- Vasomotor imbalance - autonomic dysfunction causing mucosal swelling
- Retention cyst expansion - a mucus retention cyst in the antrum gradually enlarges, herniates through the posterior fontanelle, and develops a solid nasal/choanal tail
- Nitric oxide - recent research implicates altered NO metabolism in the sinus mucosa
The antral component is cystic (fluid-filled retention cyst), while the nasal and choanal portions are solid polypoid tissue.
Clinical Features
Symptoms:
- Progressive unilateral nasal obstruction - the dominant symptom
- Mouth breathing, especially in children
- Nasal discharge (watery or mucoid)
- Snoring, sleep disturbance
- Postnasal drip
- In large polyps - sensation of something in the throat or difficulty swallowing (oropharyngeal extension)
- Pain is generally not a feature
Examination:
- Endoscopy/anterior rhinoscopy: pale, smooth, gelatinous/semitransparent mass in the nasal cavity, often seen emerging from the middle meatus
- Posterior rhinoscopy/nasopharyngoscopy: mass seen prolapsing into or filling the nasopharynx
- The mass is avascular and pale (distinguishing it from angiofibroma, which is vascular and red/pink)
- Mobile and insensitive to probing (distinguishing from hypertrophied turbinate or tumour)
Comparison: ACP vs. Ethmoidal Polyps
| Feature | Antrochoanal Polyp | Ethmoidal Polyp |
|---|---|---|
| Number | Solitary | Multiple, bilateral |
| Origin | Maxillary antrum | Ethmoidal sinuses |
| Laterality | Unilateral | Usually bilateral |
| Age group | Young adults, children | Adults/elderly |
| Allergy association | Not prominent | Strong |
| Components | Three (antral/nasal/choanal) | One |
| Pathogenesis | Infection-related | Allergy/eosinophilic |
Differential Diagnosis
- Juvenile nasopharyngeal angiofibroma - most important DD in young males; vascular, bleeds easily, red/purple, arises from posterior nasal wall
- Nasal tumours (inverted papilloma, malignancy) - must be excluded especially in adults with unilateral disease; requires imaging and biopsy
- Meningocele/encephalocele - in children; CT of anterior skull base mandatory before biopsy
- Mucous retention cyst - stays within the antrum, does not prolapse into nasal cavity
Investigations
-
CT scan (paranasal sinuses) - investigation of choice
- Shows the dumbbell-shaped mass filling the antrum, passing through the ostium, and extending to the choana/nasopharynx
- No bony destruction (distinguishes from malignancy)
- Soft tissue density with the antral component appearing hypodense (cystic)
-
Nasal endoscopy - confirms origin, extent, and character of the lesion; mandatory to exclude sinister pathology before "simple polypectomy"
-
MRI - better soft-tissue contrast; useful when CT is inconclusive or malignancy is suspected
Treatment
Treatment is always surgical. Medical treatment (steroids) is not effective.
Preferred approach: Functional Endoscopic Sinus Surgery (FESS)
- Endoscopic removal via the middle meatus with complete excision of both the nasal/choanal portion AND the antral cystic component
- The antral portion is the key - if left behind, the polyp will recur
- A middle meatal antrostomy provides access to the maxillary sinus to remove the antral component
- Curved powered instruments (microdebriders) or grasping forceps under endoscopic visualisation help retrieve the intrasinus portion
- If needed, a small inferior meatal antrostomy can be created temporarily for additional access
Other approaches (less common/historical):
- Sublabial (transcanine) approach or inferior meatus approach - as supplementary routes when endoscopic access is limited
- Caldwell-Luc surgery (open approach via canine fossa) - historically used; now reserved for exceptional cases only. Stripping of the maxillary sinus mucosa is NOT necessary and should be avoided
Recurrence
- If completely removed including the antral component - recurrence is unlikely
- If only the nasal/choanal portion is avulsed (simple polypectomy) without removing the intrasinus cyst, recurrence is the rule
Sources: Bailey and Love's Short Practice of Surgery 28th Ed., p. 792, 805; Cummings Otolaryngology Head and Neck Surgery; Grainger & Allison's Diagnostic Radiology, p. 1603
This is a shared conversation. Sign in to Orris to start your own chat.