Hirshsprung disease in neonates
Reading File
Finding Sources
Searching PubMed
Hirschsprung disease neonate diagnosis management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compose the full answer.
Hirschsprung Disease in Neonates
Definition and Epidemiology
Hirschsprung disease (HD) - also called congenital aganglionic megacolon - is a neurocristopathy caused by congenital absence of ganglion cells in the distal bowel wall. It occurs in 1 in 5,000 live births and accounts for approximately 20% of cases of partial intestinal obstruction in early infancy. Males are affected 4-5 times more often than females, though disease tends to be more severe in females. Siblings of affected individuals carry an increased risk.
Associated conditions include:
- Down syndrome (trisomy 21) - 3-10% of HD cases
- Multiple endocrine neoplasia types 2A and 2B
- Ileal/colonic/anorectal atresias, cleft palate, cardiac septal defects, polydactyly
Pathogenesis
During embryogenesis (weeks 5-12), neural crest cells migrate caudally into the developing bowel wall. In HD, this migration fails to reach the distal bowel, resulting in absence of both:
- Meissner's submucosal plexus
- Auerbach's myenteric plexus
The result is a segment of aganglionic bowel that cannot relax or propagate coordinated peristaltic waves, creating a functional obstruction. Crucially, the aganglionic distal segment appears externally normal or contracted, while the normally innervated proximal segment dilates (megacolon).
Genetics: Loss-of-function mutations in the RET receptor tyrosine kinase proto-oncogene (chromosome 10) account for most familial cases and ~15% of sporadic cases. Other mutations affect genes involved in neural crest cell development.
Segment Distribution
| Segment | Frequency |
|---|---|
| Rectosigmoid (short-segment) | ~75-80% |
| Splenic/transverse colon (long-segment) | ~17% |
| Total colonic aganglionosis (TCA) | ~8% |
| Ultrashort segment (anus/internal sphincter only) | Rare |
| Total intestinal HD | Very rare |
The aganglionic region always includes the rectum and extends proximally to a variable degree. The "transition zone" is the segment between aganglionic and normal bowel where ganglion cells begin to appear in reduced numbers.
Clinical Presentation in Neonates
90% of patients present in the neonatal period. Classic triad:
- Failure to pass meconium within the first 24-48 hours of life (most common presentation; >90% of affected neonates)
- Abdominal distension - progressive, prominent
- Bilious vomiting
A digital rectal exam or insertion of a rectal thermometer may trigger an explosive passage of stool ("squirt sign") with decompression, but symptoms recur without definitive treatment.
Later presentations (missed neonatal diagnosis) include:
- Chronic constipation, failure to thrive
- Poor weight gain, irritability
- Alternating diarrhea and obstipation
Key differential diagnoses for delayed meconium passage:
- Meconium ileus (cystic fibrosis)
- Ileal/colonic atresia
- Meconium plug syndrome / small left colon syndrome
- Anorectal malformations
- Megacystis-microcolon-intestinal hypoperistalsis syndrome
- Paralytic ileus (sepsis, drugs, metabolic)
- Hypothyroidism, infantile botulism
Life-Threatening Complication: Hirschsprung Enterocolitis (HAEC)
HAEC is the leading cause of death in Hirschsprung disease. It occurs in 18-50% of patients in both pre- and post-operative periods. Risk is higher with:
- Long-segment disease
- Diagnosis made after the first week of life
Features: Fever, explosive/bloody diarrhea, abdominal distension, sepsis, shock, hematochezia, peritonitis. It can proceed rapidly to death if unrecognized.
Investigations
Imaging
Plain abdominal X-ray: Nonspecific - shows dilated bowel loops, air-fluid levels, evidence of low bowel obstruction. May show fecal impaction with proximal obstruction. Absence of gas in the rectum is a suggestive finding in a neonate.
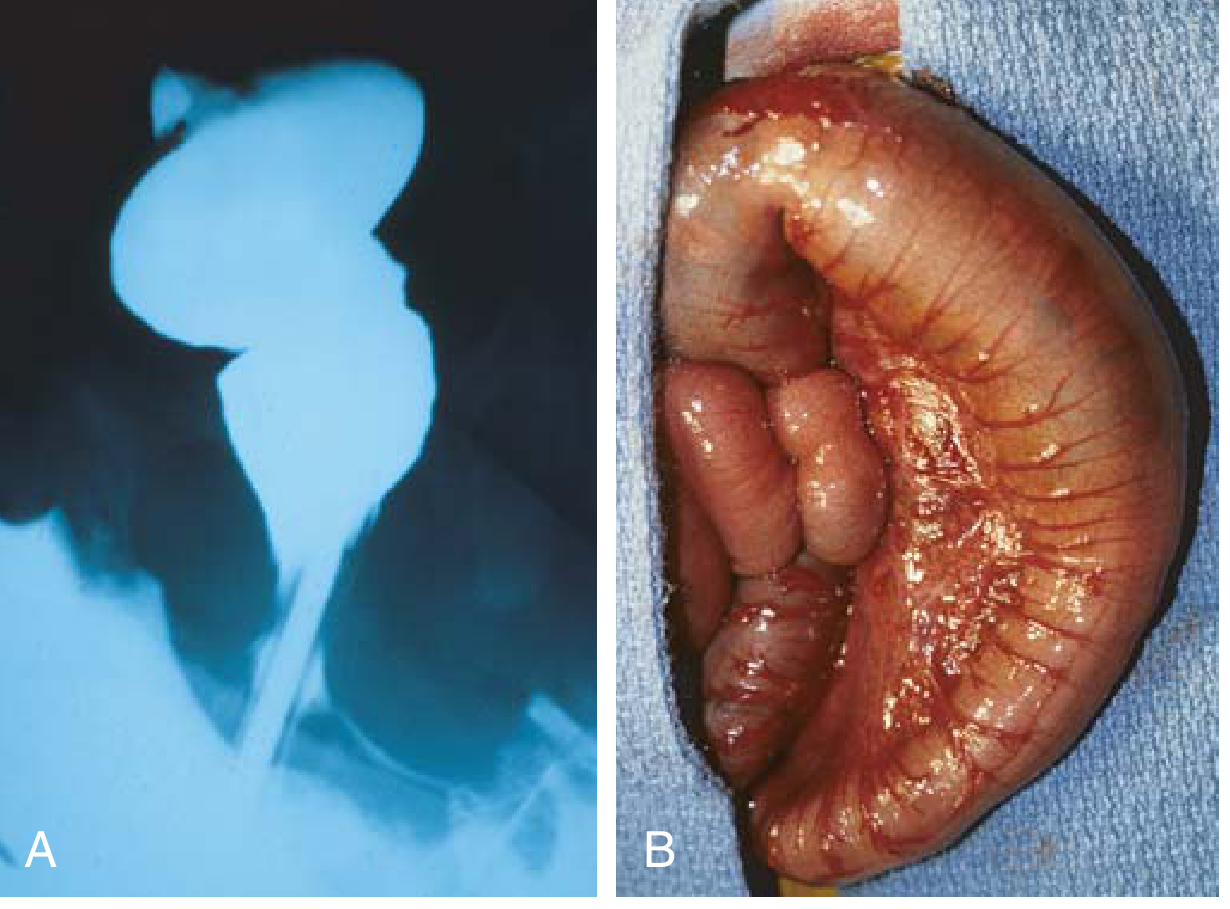
Contrast enema (study of choice in newborns):
- Narrow caliber aganglionic distal rectum
- Proximal dilation of normally innervated colon
- "Transition zone" - abrupt caliber change
- The rectosigmoid ratio is reversed (normally rectum > sigmoid; in HD, sigmoid > rectum)
- Failure to evacuate contrast within 24 hours is highly suggestive
- Sensitivity ~70%, specificity ~83%
- In TCA, the enema may be entirely normal (difficult to diagnose radiologically)
Anorectal Manometry
In toddlers, failure of the internal anal sphincter to relax on rectal balloon distension (absent recto-anal inhibitory reflex, RAIR) may be diagnostic. Not routinely used in neonates.
Rectal Biopsy (Gold Standard)
- Performed at bedside using a suction rectal biopsy kit in neonates
- Must be obtained at least 5 mm to 1 cm above the dentate line (to avoid the normal aganglionic anoderm zone)
- Two or more specimens, 1 cm apart in the posterior rectum, are recommended
- Older children require full-thickness biopsy under general anesthesia
Histopathologic criteria:
- Absent ganglion cells
- Hypertrophied nerve trunks
- Robust acetylcholinesterase (AChE) immunostaining
- Calretinin immunostaining - a standard adjunct (negative/absent staining in aganglionic segment)
Management
Immediate / Pre-operative
- Daily rectal irrigations with a soft red rubber catheter and warm normal saline - performed 1-2x/day until effluent is clear
- Decompresses the bowel and reduces risk of enterocolitis
- May not be feasible in long-segment disease, certain comorbidities, or poor family circumstances - in these cases, leveling colostomy with intraoperative biopsies is performed
Definitive Surgery: Pull-Through Procedures
All three major techniques aim to resect the aganglionic segment and anastomose normally innervated colon to the anal canal, confirmed intraoperatively by frozen section biopsy.
| Procedure | Technique |
|---|---|
| Swenson (1949, original) | Full-thickness dissection of rectum freed from sphincter mechanism; coloanal anastomosis |
| Soave (most commonly used) | Endorectal mucosal dissection of aganglionic rectum via transanal approach; ganglionated colon pulled through the remnant muscular cuff with posterior myotomy; coloanal anastomosis |
| Duhamel | Aganglionic anterior rectal cuff preserved; ganglionated colon pulled posterior to the cuff; side-to-side anastomosis creating a neorectum |
All three procedures can be performed laparoscopically or as a completely transanal (single-stage) approach. Functional results are comparable across techniques when performed by experienced surgeons. A recent 2025 meta-analysis (PMID 41454984) compared Soave vs. Swenson outcomes.
Two- or three-stage approach (leveling colostomy then pull-through) is reserved for cases with severe enterocolitis, long-segment disease, significant comorbidities, or when single-stage is not feasible.
Postoperative Issues
- Constipation (common), soiling, incontinence, postoperative enterocolitis
- Intermittent rectal decompression may be needed
- Stool softeners and laxatives for persistent constipation
- Up to 10% of patients eventually require permanent colostomy
- If symptoms persist, histologic re-evaluation to confirm normal ganglionated pull-through and rule out transition zone at anastomosis
- Anastomotic leaks, fistulae, abscesses, stenoses are recognized complications
Summary Table
| Feature | Details |
|---|---|
| Incidence | 1 in 5,000 live births |
| M:F ratio | 4-5:1 |
| Pathology | Absent Auerbach + Meissner plexus in distal bowel |
| Gene | RET proto-oncogene (chromosome 10) |
| Most common segment | Rectosigmoid (~75-80%) |
| Classic neonatal presentation | Failure to pass meconium >24h, abdominal distension, bilious vomiting |
| Gold standard diagnosis | Suction rectal biopsy (absent ganglia, AChE staining) |
| Imaging of choice (newborn) | Contrast enema (transition zone, reversed rectosigmoid ratio) |
| Adjunct histology | Calretinin immunostaining |
| Lethal complication | Hirschsprung enterocolitis (HAEC) |
| Definitive treatment | Pull-through procedure (Soave/Swenson/Duhamel) |
Sources:
- Sabiston Textbook of Surgery, block 28 (p. 2687-2688)
- Robbins Basic Pathology, block 6 (p. 563)
- Rosen's Emergency Medicine, block 30
- Grainger & Allison's Diagnostic Radiology, block 13 (p. 1797-1798)
Recent evidence: A 2025 systematic review and meta-analysis (PMID 41454984, Pediatric Surgery International) compared Soave vs. Swenson pull-through procedures - no update to core diagnostic or pathophysiologic guidelines was identified.
Postoperative complications of fentanyl and atracurium in neonates
Finding Sources
Finding Sources
Searching PubMed
fentanyl atracurium neonatal postoperative complications
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Now I have comprehensive textbook content on both drugs in neonates. Note that the textbooks specifically cover cisatracurium (not atracurium) in neonates. I'll compose the full detailed answer covering both fentanyl AND atracurium (including the distinction between atracurium and cisatracurium).
Postoperative Complications of Fentanyl and Atracurium in Neonates
Why Neonates Are Uniquely Vulnerable
Before discussing drug-specific complications, it is essential to understand the physiologic features that make neonates susceptible to adverse effects from both agents:
| Factor | Clinical Relevance |
|---|---|
| Immature hepatic enzyme systems | Reduced clearance of fentanyl and laudanosine (atracurium metabolite) |
| Immature renal function | Reduced excretion; prolongs drug/metabolite half-lives |
| Larger extracellular fluid (ECF) volume | Larger volume of distribution - may require higher mg/kg dosing but prolongs effect |
| Lower plasma protein binding (albumin, α1-acid glycoprotein) | Higher free drug fraction; enhanced pharmacodynamic effects |
| Highly compliant, cartilaginous chest wall | Especially vulnerable to chest wall rigidity from opioids |
| Immature brainstem respiratory control | Exaggerated respiratory depression, apnea at lower doses |
| Sensitive neuromuscular junction | More sensitive to nondepolarizing blockade; unpredictable recovery |
FENTANYL - Postoperative Complications in Neonates
Fentanyl is the most widely used opioid in neonatal ICU and perioperative settings, given as 2-4 mcg/kg/hr infusion or 5-10 mcg/kg boluses.
1. Respiratory Depression
The most common and most dangerous postoperative complication. Neonates are listed as a high-risk group for opioid-induced respiratory depression (along with elderly, sleep, high dose, and CNS depressant co-administration).
Mechanisms:
- μ-receptor activation in the brainstem respiratory center
- Raises the apneic threshold (less sensitive to CO2 rise)
- Blunts the hypoxic ventilatory drive
- Even mild hypocapnia (from anxious or pain-driven hyperventilation pre-op) enhances and prolongs postoperative respiratory depression after fentanyl - because hypocapnia increases un-ionized (brain-penetrant) fentanyl and decreases cerebral blood flow, slowing clearance
Key points:
- Continuous infusions cause respiratory depression more frequently than bolus doses in neonates
- Postoperative mechanical ventilation is required when high-dose fentanyl (>20 mcg/kg) is used
- Pulse oximetry may fail to detect early respiratory depression during hyperoxia - SpO2 remains normal in the first minutes
2. Chest Wall Rigidity (Fentanyl-Induced Muscle Rigidity / "Wooden Chest")
A particularly dangerous complication in neonates:
- Doses as small as 1-2 mcg/kg can cause significant chest wall and glottic rigidity in neonates
- Results in desaturation and inability to ventilate with bag-mask
- May require neuromuscular blocking agent and emergency intubation
- Mechanism: μ-opioid receptor activation causing increased muscle spindle activity; more pronounced with rapid IV bolus administration
- The highly compliant neonatal chest wall makes the rigid thorax particularly difficult to ventilate manually
3. Hemodynamic Instability
- When used with benzodiazepines (e.g., midazolam), fentanyl can cause hypotension in neonates
- In isolation at standard doses, fentanyl maintains good cardiovascular stability
- Causes bradycardia by reducing sympathetic tone and enhancing parasympathetic activity
- Combination of opioids + benzodiazepines for >1 week is associated with worse neurodevelopmental outcomes compared to either agent alone
4. Tolerance and Withdrawal
- Neonates receiving prolonged fentanyl infusions (>5-7 days) develop opioid tolerance and physical dependence
- Abrupt discontinuation causes a neonatal opioid withdrawal syndrome: irritability, tachycardia, diaphoresis, feeding difficulty, tremors, high-pitched cry
- Management requires weaning via methadone (long-acting opioid) in the NICU setting
- Methadone use requires ECG monitoring for QT prolongation
5. Renarcotization After Naloxone
- Fentanyl has a longer plasma half-life than naloxone
- After reversal with naloxone bolus, re-sedation and respiratory depression can recur ("renarcotization") as the naloxone effect wanes
- Requires continuous naloxone infusion or repeated dosing, with careful monitoring
6. Opioid-Induced Pulmonary Vasoconstriction Blunting
- Fentanyl blocks stimulus-induced pulmonary vasoconstriction, which can be beneficial in neonates with reactive pulmonary vascular beds (e.g., after CDH repair, CHD surgery)
- In the postoperative period, loss of this effect upon drug clearance may trigger rebound pulmonary hypertensive crises if fentanyl is weaned too quickly
7. Neurodevelopmental Concerns
- No significant maturational change in brain sensitivity to fentanyl (unlike morphine, where morphine-6-glucuronide sensitivity increases with age)
- Sedation with combined opioids and benzodiazepines >1 week in neonates is associated with worse neurodevelopmental outcomes
ATRACURIUM - Postoperative Complications in Neonates
Atracurium is a bisbenzyltetrahydroisoquinolinium class intermediate-acting nondepolarizing neuromuscular blocking agent (NMBA). Its sister compound cisatracurium (the 1R-cis, 1'R-cis isomer) is used more commonly in neonates due to less histamine release. Both share Hofmann elimination.
1. Prolonged Neuromuscular Blockade
The most critical postoperative complication:
- The neonatal NMJ is more sensitive to nondepolarizing agents, meaning a lower dose achieves block
- However, this is counterbalanced by the larger ECF volume (larger volume of distribution), so mg/kg dosing is similar to older children
- Organ maturation has a tremendous impact on clearance - there is considerable variability and unpredictability in duration of action in neonates
- Postoperative residual neuromuscular blockade can cause respiratory failure, upper airway obstruction, and inability to extubate
Why atracurium is unique: It undergoes Hofmann elimination (spontaneous, pH- and temperature-dependent chemical degradation) and ester hydrolysis - both organ-independent. This means renal and hepatic immaturity in neonates does not significantly prolong its elimination. This makes it more predictable than vecuronium or pancuronium in neonates.
However, postoperative complications still occur due to:
- Hypothermia - slows Hofmann elimination (requires normal body temperature for reliable degradation)
- Acidosis - also slows Hofmann elimination
- Altered pH - since elimination is pH-dependent, any acid-base disturbance (common postoperatively in sick neonates) can prolong block
2. Histamine Release (Atracurium > Cisatracurium)
Atracurium (the parent compound, not cisatracurium) causes histamine release - a significant concern:
- Manifests as: skin flushing, urticaria, hypotension, bronchospasm, tachycardia
- Neonates, especially those with reactive airways or congenital lung disease, are at higher risk
- Cisatracurium, which specifically lacks histamine release, is preferred in neonates for this reason
- Histamine-mediated bronchospasm can lead to severe postoperative respiratory compromise
3. Laudanosine Accumulation (Metabolite Toxicity)
Atracurium is metabolized via Hofmann elimination to laudanosine (and acrylates):
- Laudanosine is a CNS stimulant that can lower the seizure threshold
- Accumulates with prolonged infusions in neonates, particularly in hepatic failure (laudanosine is cleared hepatically)
- Although not clinically significant at typical single doses, prolonged NICU infusions raise concern for seizure activity in neonates
- Cisatracurium produces approximately 5-fold less laudanosine than atracurium at equipotent doses
4. Inadequate Reversal and Postoperative Apnea
The unpredictable nature of NMBAs in the neonatal population, combined with difficulty assessing neuromuscular function (reliable nerve stimulator monitoring is challenging in small neonates), mandates reversal of all nondepolarizing agents.
Neostigmine reversal complications:
- Neostigmine administered without an anticholinergic agent (atropine or glycopyrrolate) is the most common drug error leading to perioperative cardiac arrest in the pediatric population - causes profound bradycardia and bronchospasm
- Neostigmine requires ~10 minutes for 90% reversal at 0.07 mg/kg
Sugammadex does NOT reverse atracurium (it only reverses aminosteroid NMBAs - rocuronium, vecuronium). Reversal of atracurium/cisatracurium requires neostigmine.
5. Cardiovascular Effects
- Unlike pancuronium, atracurium and cisatracurium have minimal to no direct cardiovascular effects on the neonatal myocardium
- However, histamine release from atracurium can cause tachycardia, hypotension, and vasodilation postoperatively
- Cisatracurium has essentially no cardiovascular side effects
6. Temperature and pH Dependence
A unique concern in neonates who commonly become hypothermic or acidotic postoperatively:
- Hofmann elimination slows dramatically with hypothermia and acidosis
- A neonate who was blocked intraoperatively and then becomes cold or acidotic postoperatively may have unexpectedly prolonged paralysis
- Active warming and acid-base correction are essential to restore predictable recovery
Summary Comparison Table
| Complication | Fentanyl | Atracurium |
|---|---|---|
| Respiratory depression | Major - dose-dependent, amplified by hypocapnia | Via residual blockade (indirect) |
| Chest wall rigidity | Yes - even at 1-2 mcg/kg | Not applicable |
| Histamine release | No | Yes (atracurium > cisatracurium) |
| Bronchospasm | No (mild bronchoconstriction at high doses) | Yes - via histamine (atracurium) |
| Hypotension | With benzodiazepine combo | Yes - via histamine (atracurium) |
| Bradycardia | Yes - parasympathetic effect | No (atracurium); Yes - reversal agent (neostigmine without anticholinergic) |
| Prolonged blockade | Prolonged sedation/resp depression with infusion | Yes - hypothermia, acidosis slow Hofmann elimination |
| Seizure risk | No | Laudanosine accumulation (prolonged infusion) |
| Tolerance/dependence | Yes - with prolonged infusion | No |
| Withdrawal | Yes - NAS-like syndrome | No |
| Neurodevelopmental risk | Yes - with benzodiazepine co-use >1 week | Not established |
Monitoring and Reversal Essentials
- Nerve stimulator monitoring mandatory but technically challenging in neonates
- All nondepolarizing NMBAs must be reversed in neonates given unpredictability
- Neostigmine must always be paired with atropine or glycopyrrolate
- Maintain normothermia and correct acidosis postoperatively to ensure Hofmann elimination proceeds normally
- Fentanyl-treated neonates require continuous SpO2 and respiratory rate monitoring; have naloxone and ventilation equipment at bedside
- In cases of fentanyl chest wall rigidity: succinylcholine 3 mg/kg IV + immediate intubation
Sources:
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e (pp. 3594-3599) - Neonatal opioids and NMBAs
- Miller's Anesthesia, 10e (pp. 10765-10768) - Fentanyl in neonatal cardiac surgery; opioid-induced respiratory depression
- Miller's Anesthesia, 10e (Box 22.2) - Factors increasing opioid respiratory depression
This is a shared conversation. Sign in to Orris to start your own chat.