Explain ICE syndrome in eye I am a postgraduate student in India explain in easy method
Reading File
Finding Sources
Searching the Web
ICE syndrome iridocorneal endothelial syndrome ophthalmology pathogenesis clinical features
Finding Sources
Reading Web Page
https://eyewiki.org/Iridocorneal_Endothelial_Syndrome_and_Se…
Reading File
Reading Web Page
https://eyesoneyecare.com/resources/iridocorneal-endothelial…
Loading Image
Here is a complete, exam-oriented explanation of ICE syndrome for a postgraduate student in India.
ICE Syndrome (Iridocorneal Endothelial Syndrome)
ICE stands for Iridocorneal Endothelial syndrome. It is a group of three related conditions all sharing the same underlying problem: abnormal corneal endothelial cells that proliferate and migrate where they should not.
The "One Liner" to Remember
ICE syndrome = Abnormal corneal endothelial cells migrate onto iris & angle → Corneal edema + Iris changes + Secondary angle-closure glaucoma; unilateral, middle-aged women.
Epidemiology (High-yield)
| Feature | Detail |
|---|---|
| Age | 20-50 years (middle-aged) |
| Sex | Females >> Males |
| Laterality | Unilateral (almost always) |
| Heredity | Sporadic (non-familial) |
| Aetiology | Possible Herpes Simplex Virus (HSV) (PCR shows HSV DNA in corneal and trabecular meshwork specimens) |
Pathogenesis - The Core Concept
Think of it in 3 simple steps:
Step 1 - The ICE Cell Problem
Normal corneal endothelial cells are replaced by abnormal cells (called "ICE cells"). These cells undergo an "endothelial-to-epithelial" transformation - they start behaving like epithelial cells, gaining:
- Desmosomes and tonofilaments (epithelial markers)
- Migratory ability
- Contractile properties
Step 2 - Migration
These ICE cells migrate posteriorly across Schwalbe's line → onto the trabecular meshwork → onto the iris surface (forming an abnormal membrane).
Step 3 - Damage
The contractile membrane:
- Blocks the trabecular meshwork → raised IOP → glaucoma
- Pulls the iris → corectopia, iris atrophy, holes
- Covers the iris → nodules (Cogan-Reese)
- Reduces corneal endothelial pump function → corneal edema
The Three Subtypes - Easy Memory Method
Use the mnemonic "C-E-N" (Chandler, Essential/Progressive, Nevus/Cogan-Reese)
1. Chandler Syndrome (Most Common - ~50%)
- Main feature: CORNEA (most corneal involvement of the three)
- "Hammered silver" or "beaten bronze" endothelium on slit lamp
- Microcystic corneal edema - even with normal IOP (classic exam point!)
- Iris changes are mild or absent (60% have no iris changes)
- Glaucoma is least severe of the three
Memory tip: Chandler = Cornea affected most, iris spared most
2. Progressive (Essential) Iris Atrophy
- Main feature: IRIS destruction
- Sequence: Corectopia (displaced pupil) → iris atrophy → pseudopolycoria (false extra pupil) → full-thickness holes in iris
- Broad-based PAS extending anterior to Schwalbe's line (on gonioscopy)
- Severe glaucoma in late stages
- Ectropion uveae present
Memory tip: Progressive = Pupil pulled, Polycoria, Perforations
3. Iris Nevus / Cogan-Reese Syndrome
- Main feature: Iris NODULES
- Tan/brown pedunculated nodules or diffuse pigmented lesions on anterior iris surface
- Iris atrophy is absent in 50% or mild
- Can mimic diffuse iris melanoma (important differential!)
Memory tip: Cogan-Reese = Chocolate-colored nodules/Café-au-lait spots on iris
Clinical Features Summary Table
| Feature | Chandler | Progressive Iris Atrophy | Cogan-Reese |
|---|---|---|---|
| Corneal edema | +++ (most severe) | ++ | ++ |
| Iris atrophy | Mild/absent | Severe | Mild/absent |
| Corectopia | Mild | Severe | Mild-severe |
| Iris holes | No | Yes (late) | No |
| Iris nodules | No | No | Yes |
| Glaucoma severity | Mild | Severe | Moderate |
Clinical Image from Kanski's Ophthalmology
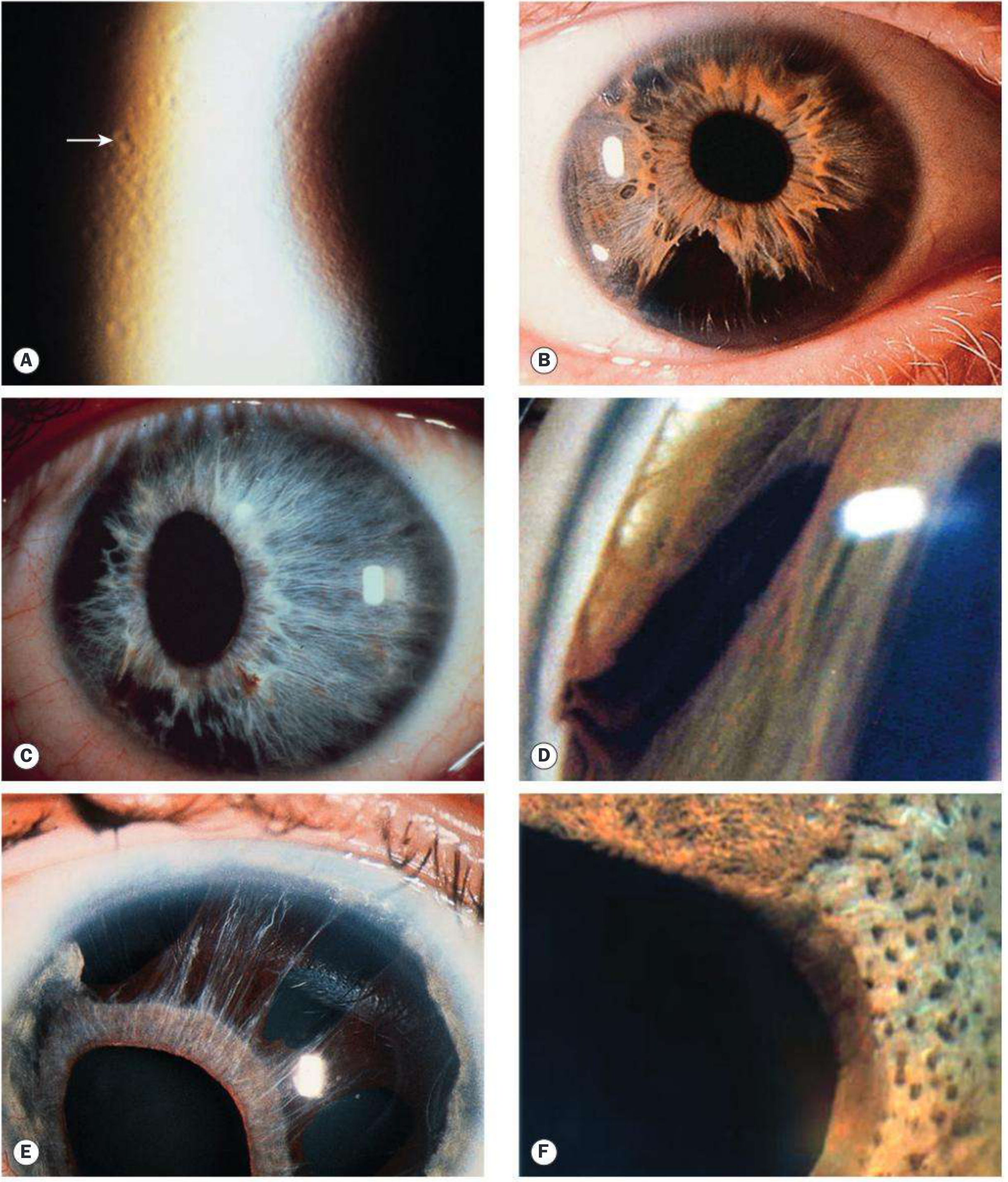
(A) Chandler syndrome - "hammered silver" endothelial changes (arrow) | (B) Iris atrophy | (C) Corectopia with pseudopolycoria | (D) Gonioscopy: broad peripheral anterior synechiae | (E) Progressive iris atrophy with polycoria (full holes) | (F) Iris nodules in Cogan-Reese syndrome
Diagnosis
1. Slit Lamp Examination
- Hammered silver/beaten bronze corneal appearance
- Iris changes (as per subtype)
2. Specular Microscopy (Key investigation)
- Shows large, pleomorphic, dark "ICE cells" - the hallmark
- Easy to mistake for guttata (Fuchs dystrophy)
3. Gonioscopy
- Broad-based PAS extending anterior to Schwalbe's line
- Subtle in early disease despite elevated IOP
4. AS-OCT / UBM - shows angle compromise and membrane extension
Differentials (Exam-relevant)
| Condition | How to distinguish from ICE |
|---|---|
| Fuchs' Endothelial Dystrophy | Bilateral, older age, true guttata on specular microscopy, no iris changes |
| Primary Angle-Closure Glaucoma | Bilateral, no iris atrophy, no ICE cells |
| Anterior Uveitis | Posterior synechiae (not PAS), keratic precipitates |
| Rieger Anomaly/Syndrome | Bilateral, developmental/congenital, posterior embryotoxon |
| Diffuse Iris Melanoma | No corneal changes, no ICE cells |
Treatment
For Glaucoma (the main challenge):
- Medical therapy alone is usually ineffective (Kanski's)
- Trabeculectomy with Mitomycin C - can be tried but long-term results are poor
- Aqueous shunt/tube surgery (e.g., Ahmed valve) - better long-term IOP control
- Laser iridotomy - NOT effective (the membrane re-closes the angle)
For Corneal Edema:
- Hypertonic saline drops/ointment (5% NaCl) - for mild edema
- Descemet's Membrane Endothelial Keratoplasty (DMEK) / DSAEK - for corneal decompensation (preferred over PK)
- Penetrating Keratoplasty (PK) - older option, reserved for severe cases
High-Yield Exam Points Summary
- ICE = Unilateral disease in middle-aged women (bilateral is a red flag against ICE)
- Aetiology = HSV (PCR evidence)
- All three subtypes share: ICE cells on specular microscopy + PAS on gonioscopy
- Chandler = most common, worst cornea, best iris
- Progressive iris atrophy = worst iris destruction, worst glaucoma
- Cogan-Reese = nodules (do not mistake for melanoma)
- Glaucoma in ICE = secondary angle-closure (not open-angle)
- Medical treatment for glaucoma is usually ineffective - surgical approach preferred
- Corneal transplant of choice today = DSAEK/DMEK (not full PK)
- Laser PI is NOT effective in ICE (unlike primary angle closure)
Sources: Kanski's Clinical Ophthalmology - A Systematic Approach 10th ed., p. 412; EyeWiki - ICE Syndrome; Eyes on Eyecare
This is a shared conversation. Sign in to Orris to start your own chat.