so in a thrombotic stroke due to plaquerupture causes pale infarct , but due to embolic strole that embolus gets lysed and re entered blood causes hamorrhagic infarct ?
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Your understanding is mostly correct but has a few nuances worth clarifying. Here's the full picture:
Pale (Anemic) vs. Hemorrhagic Infarct in Stroke
The Core Concept
All brain infarcts start as pale/anemic infarcts. This is because the brain has end-organ circulation with limited collateral supply. When a vessel is occluded, the tissue simply dies without blood — no blood means no red cells, so the infarct appears pale.
"Occlusive brain infarcts generally start as nonhemorrhagic (pale/anemic)" — Robbins & Cotran Pathologic Basis of Disease
Why Thrombotic Stroke → Stays Pale
In thrombotic stroke (e.g., from atherosclerotic plaque rupture), the thrombus tends to persist at the site of occlusion. The vessel remains blocked, blood never re-enters the infarcted tissue, and the infarct stays pale. No reperfusion = no hemorrhagic transformation.
Why Embolic Stroke → Can Become Hemorrhagic ✓ (You're correct here)
Your mechanism is correct. Here's the step-by-step:
- An embolus (cardiac thrombus, atheromatous debris, etc.) lodges in a cerebral artery → tissue becomes ischemic → initially a pale infarct
- The ischemia damages the small vessel walls (endothelium + basement membrane) in the infarcted zone
- The embolus spontaneously lyses (fibrinolysis) OR breaks up and moves distally → blood flow reperfuses the now-damaged vessels
- Those weakened vessel walls cannot withstand the reperfusion pressure → they leak or rupture → hemorrhagic transformation
"Secondary hemorrhage can occur from ischemia-reperfusion injury following spontaneous or therapeutic dissolution or fragmentation of the intravascular occlusive material. This process (termed secondary hemorrhagic transformation) develops if the ischemic event lasts long enough to damage small blood vessels in the affected area; the resulting reperfusion hemorrhages are largely punctate in nature but may be multiple or even confluent." — Robbins & Cotran Pathologic Basis of Disease
Important Nuances
| Feature | Thrombotic Stroke | Embolic Stroke |
|---|---|---|
| Cause | Atherosclerosis/plaque rupture, in situ thrombosis | Cardiac (AFib, mural thrombus), carotid plaque |
| Infarct type (early) | Pale | Pale |
| Subsequent change | Stays pale | Can undergo hemorrhagic transformation |
| Mechanism | Vessel stays occluded | Embolus lyses → reperfusion → vessel wall damage → bleeding |
| Clinical implication | tPA may be given | Hemorrhagic transformation is a risk; if already hemorrhagic, tPA is contraindicated |
One key correction to your phrasing: The embolus doesn't just "get lysed and re-enter blood" — the embolus dissolves/fragments, which allows blood back into the previously ischemic territory. The problem is the vessel walls in that ischemic zone have been damaged by the preceding ischemia, so reperfusion causes them to bleed. It's the damaged vessel wall + restored blood pressure that causes hemorrhage, not the embolus material itself re-entering.
The Gross Pathology
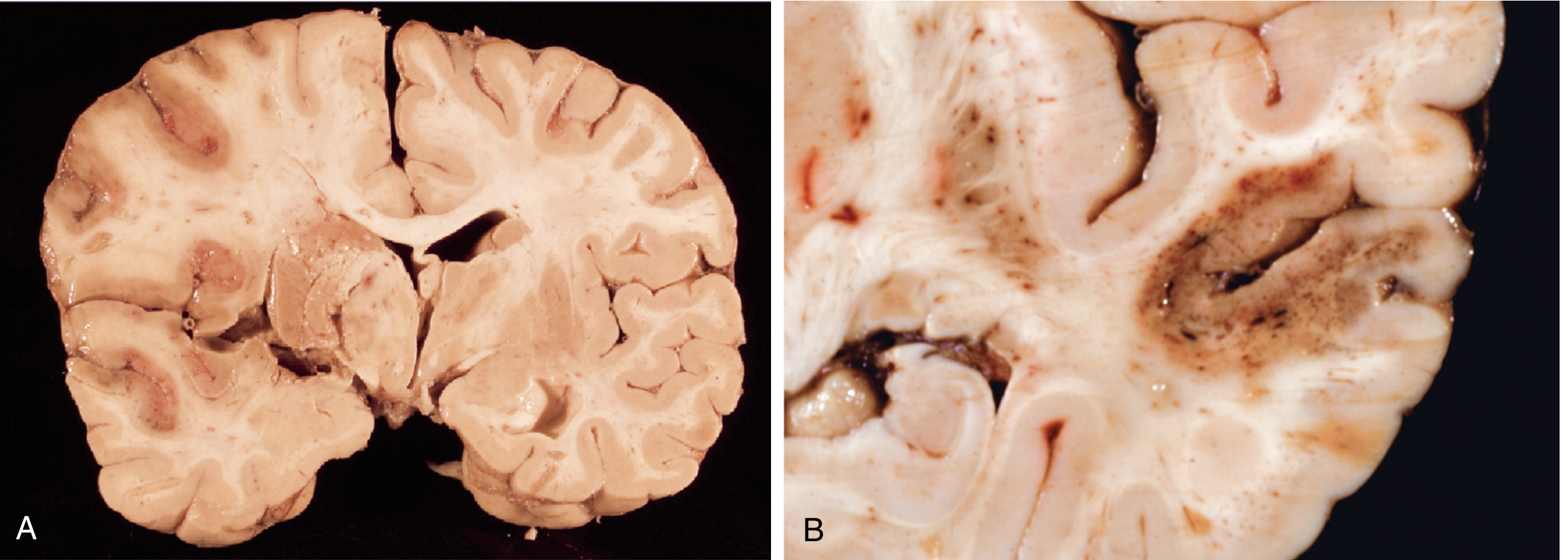
(A) — Pale/anemic infarct: MCA territory, no blood re-entry, tissue appears pale and soft.
(B) — Hemorrhagic infarct: punctate (petechial) hemorrhages from reperfusion injury — the classic appearance after embolic stroke with embolus lysis.
Bottom line: Your reasoning is correct. Embolic stroke → embolus lyses → reperfusion of ischemia-damaged vessels → hemorrhagic transformation. Thrombotic stroke → thrombus persists → no reperfusion → stays pale. The key mechanistic detail is that it's the vessel wall damage from prolonged ischemia that makes reperfusion dangerous — those same vessels that would normally handle blood flow can no longer do so after being ischemic.
why dont a thrombus lyses and cause hi
Great question. The short answer: a thrombus CAN lyse and cause hemorrhagic transformation too — but it does so much less commonly than an embolus, for several structural and biological reasons.
Why Thrombotic Strokes Rarely Undergo Hemorrhagic Transformation
1. Thrombus is Large, Adherent, and Fibrin-Rich
- An in situ thrombus (from plaque rupture) forms directly on the vessel wall, is tightly adherent, and is rich in cross-linked fibrin — it's structurally robust and resists spontaneous lysis
- An embolus (especially a cardiac one) is often a looser, platelet-rich or red thrombus that travels far from its origin, lodges in a smaller distal vessel, and is more susceptible to endogenous fibrinolysis
2. Collateral Circulation is More Likely to Be Poor
- In atherosclerotic thrombotic stroke, the vessel has been gradually narrowing over months to years — the brain has often developed some collateral flow already. This paradoxically means the infarct may be less dense, but reperfusion through those collaterals is sluggish, not a sudden rush
- In embolic stroke, the vessel was suddenly and completely occluded in a previously normal artery — no collaterals had time to form. When the embolus lyses, reperfusion is sudden and forceful → greater risk of hemorrhage
3. Location of Occlusion
- Thrombotic strokes tend to occur in large proximal vessels (e.g., ICA, proximal MCA) where the thrombus burden is large and spontaneous lysis is unlikely
- Emboli travel distally and lodge at branching points in smaller vessels, where they are more exposed to fibrinolytic enzymes in the blood and more likely to fragment
4. Spontaneous Lysis Rate
- Emboli — especially cardiac emboli from atrial fibrillation — have a documented high rate of spontaneous lysis within hours to days
- In situ thrombi on ruptured plaques are organized and reinforced over time, making spontaneous lysis far less likely without intervention
The Key Principle
| In Situ Thrombus | Embolus | |
|---|---|---|
| Attachment | Adherent to vessel wall | Free-floating, lodged distally |
| Composition | Fibrin-rich, organized | Looser, platelet/red cell mix |
| Spontaneous lysis | Uncommon | Common |
| Reperfusion risk | Low (unless tPA given) | High (spontaneous or tPA) |
| Hemorrhagic transformation | Less common | More common |
One Important Caveat
A thrombotic stroke can undergo hemorrhagic transformation if:
- tPA (thrombolytics) are given therapeutically — this forcibly lyses the thrombus and causes the same ischemia-reperfusion mechanism
- The patient has hypertension at the time of reperfusion
- There is extensive collateral reperfusion after partial recanalization
This is exactly why CT scan is mandatory before giving tPA — you must rule out existing hemorrhage, and you must weigh the risk of inducing hemorrhagic transformation even in an ischemic stroke.
So the distinction isn't absolute — it's a matter of probability. Emboli lyse spontaneously and frequently; thrombi usually don't, unless you lyse them pharmacologically.
This is a shared conversation. Sign in to Orris to start your own chat.