Conjugate movements of brain
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the information needed to write a comprehensive answer. Here is the full response:
Conjugate Movements of the Brain (Eye Movements)
Conjugate eye movements (also called version movements) are movements in which both eyes move simultaneously in the same direction. This is in contrast to vergence movements, where the eyes move in opposite directions (e.g., convergence for near vision).
1. Types of Conjugate Eye Movements
| System | Description | Function | Key Anatomic Structures |
|---|---|---|---|
| Saccades | Fast (up to 700°/sec), voluntary | Bring fovea rapidly to a new target | Frontal eye field, superior colliculus, PPRF (horizontal), pretectum (vertical) |
| Smooth Pursuit | Slow (up to 100°/sec), involuntary | Track a moving target smoothly | Occipital/parietal cortex, pons, cerebellar flocculus |
| Vestibulo-ocular reflex (VOR) | Slow, compensatory | Stabilize gaze when the head moves | Pontomedullary region, vestibular nuclei |
| Optokinetic nystagmus | Reflex rhythmic movement | Stabilize image during sustained motion | Brainstem and vestibular nuclei |
- Goldman-Cecil Medicine, p. 4147
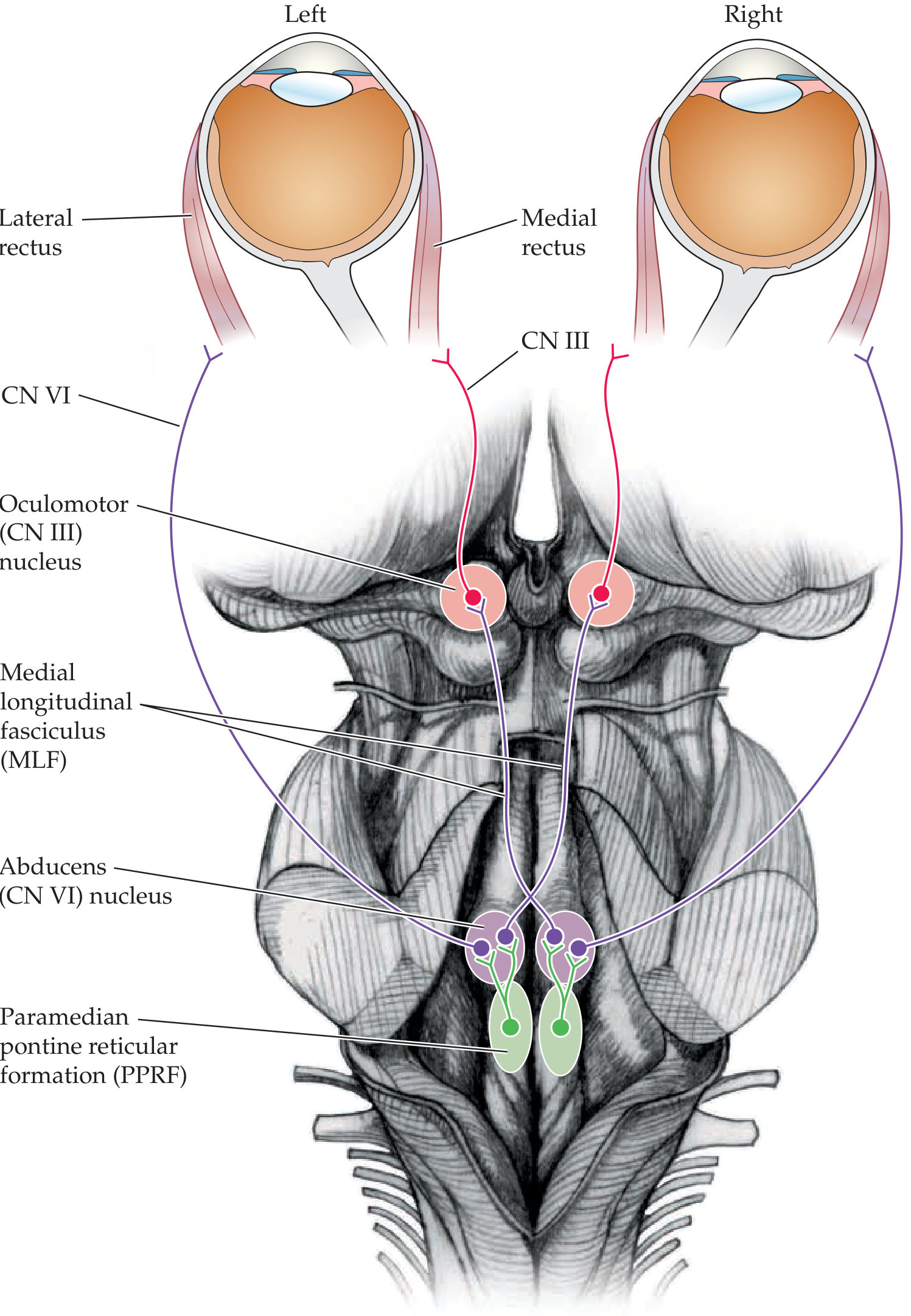
2. Horizontal Conjugate Eye Movements
Key Circuit
The medial longitudinal fasciculus (MLF) is the critical white matter tract that yokes the two eyes together, connecting:
- Abducens nucleus (CN VI) - in the pons
- Oculomotor nucleus (CN III) - in the midbrain
When the right eye abducts (right lateral rectus, CN VI), the left eye simultaneously adducts (left medial rectus, CN III) via the MLF.
The Abducens Nucleus as a Gaze Center
The abducens nucleus does more than just abduct the ipsilateral eye. It is a horizontal gaze center for both eyes:
- Some neurons project to the ipsilateral lateral rectus (via CN VI)
- Other neurons project via the MLF to the contralateral oculomotor nucleus, activating the contralateral medial rectus
PPRF (Paramedian Pontine Reticular Formation)
Located adjacent to the abducens nucleus, the PPRF is an additional horizontal gaze center that receives inputs from the cortex and relays them to the abducens nucleus to generate lateral conjugate gaze.
3. Vertical Conjugate Eye Movements
Vertical gaze centers are located in the rostral midbrain reticular formation and pretectal area:
- Upgaze center: dorsal region, near the posterior commissure
- Downgaze center: ventral region - the rostral interstitial nucleus of the MLF (riMLF) is the key nucleus here; other contributing nuclei include the nucleus of Darkschewitzh and the interstitial nucleus of Cajal
Vertical eye movements are normally coupled with upper eyelid movements (mediated by the M-group of neurons near these nuclei).
4. Cortical and Supranuclear Control
| Region | Role |
|---|---|
| Frontal Eye Fields (FEF) - Brodmann area 6/8, at superior frontal-precentral sulcus junction | Generate saccades toward the contralateral direction, via projections to the contralateral PPRF |
| Parieto-occipito-temporal cortex | Primarily mediates smooth pursuit in the ipsilateral direction, via connections with vestibular nuclei, cerebellum, and PPRF |
| Cerebellum (flocculus, dorsal vermis, fastigial nuclei) | Coordinates accuracy and gain of eye movements; adjusts saccadic amplitude; ensures precise conjugate movements |
| Basal ganglia | Modulatory control; dysfunction causes characteristic eye movement disorders |
5. Clinical Correlations - Lesions of Conjugate Gaze
The following diagram summarizes the effects of different lesions:
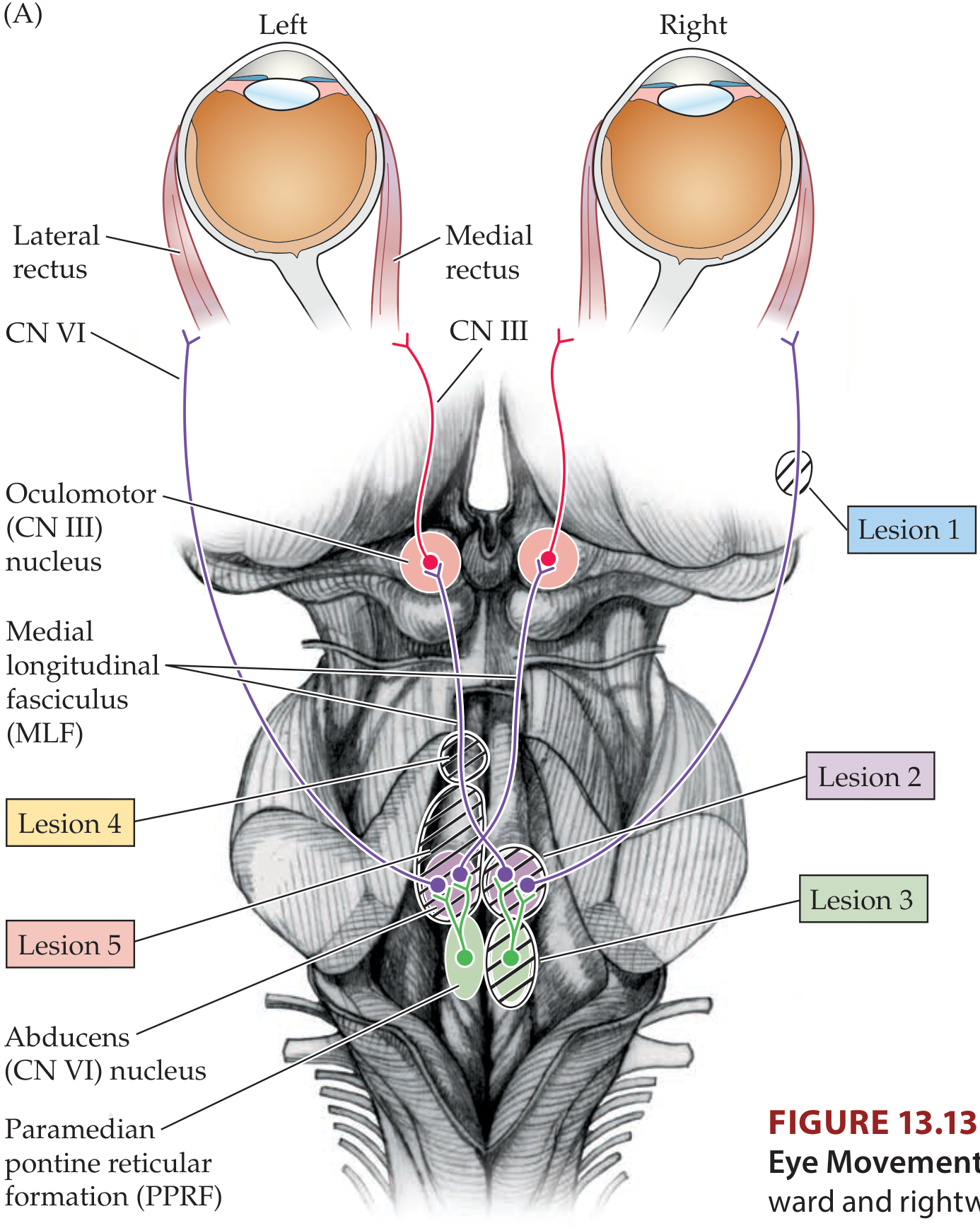
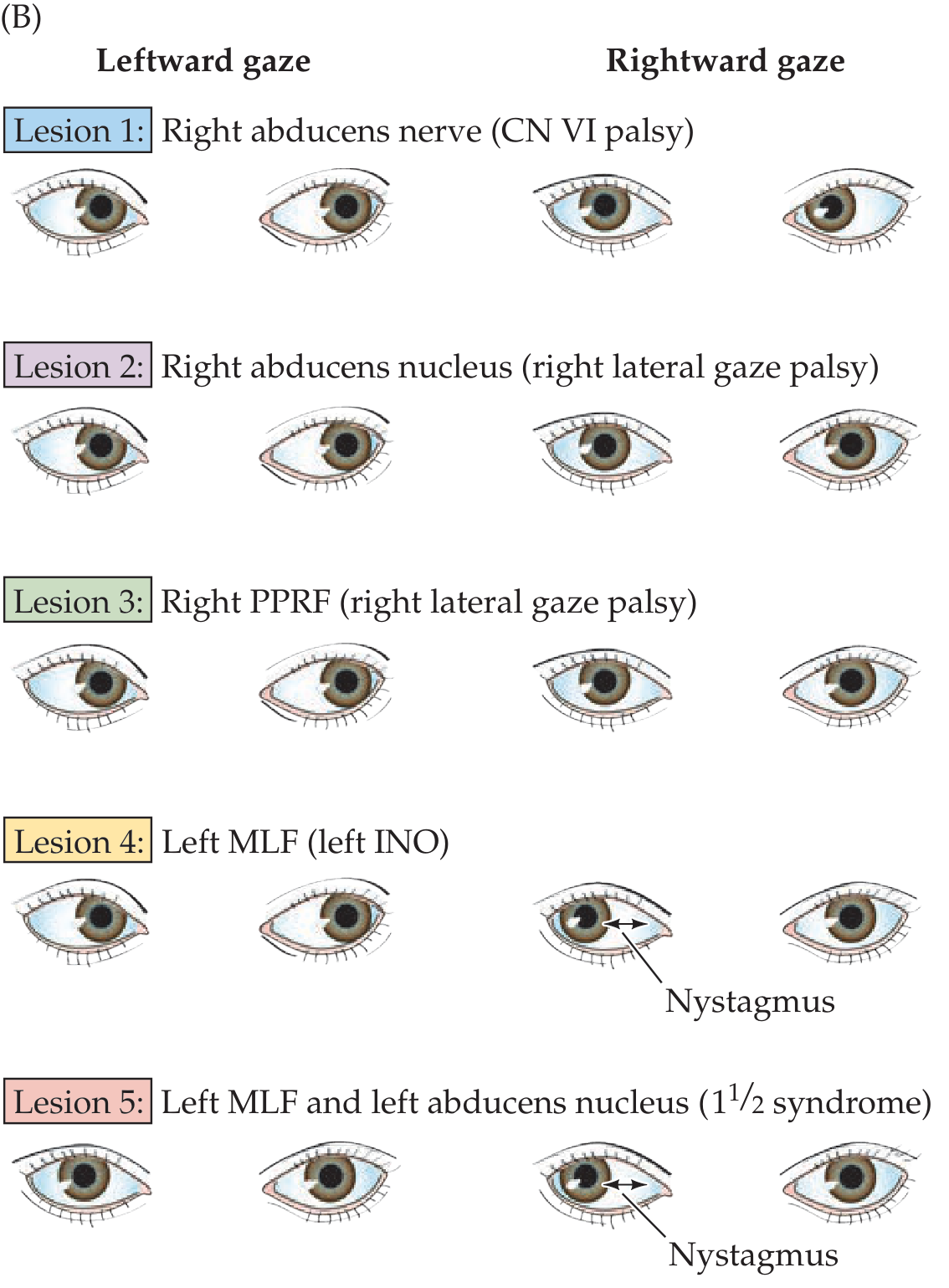
Summary of Important Lesions
| Lesion | Effect |
|---|---|
| CN VI (abducens nerve) | Impaired abduction of the ipsilateral eye only |
| Abducens nucleus | Ipsilateral lateral gaze palsy (both eyes cannot look ipsilaterally) |
| PPRF | Ipsilateral lateral gaze palsy (same as abducens nucleus lesion) |
| MLF (unilateral) | Internuclear ophthalmoplegia (INO): impaired adduction ipsilateral to lesion + contralateral abducting nystagmus; convergence often spared |
| MLF + abducens nucleus (same side) | One-and-a-half syndrome: ipsilateral eye cannot move horizontally at all; contralateral eye can only abduct |
| Frontal eye field (acute lesion, e.g., stroke) | Transient inability to gaze contralaterally; eyes deviate toward side of lesion ("eyes look toward the lesion") |
| Bilateral frontal eye fields | Oculomotor apraxia: loss of voluntary horizontal and vertical eye movements with preserved reflex eye movements |
| Dorsal midbrain/pretectum | Parinaud's syndrome: impaired upgaze, convergence-retraction nystagmus on attempted upgaze, light-near dissociation of pupils |
| Pontine lesion (e.g., hemorrhage) | "Wrong-way eyes": eyes deviate contralateral to lesion (toward weakness), due to PPRF disruption with preserved frontal lobe drive |
- Neuroanatomy through Clinical Cases, 3rd Edition, pp. 612-617
- Goldman-Cecil Medicine, p. 4147
6. Vergence (Disconjugate) - For Contrast
Vergence movements are NOT conjugate - both eyes move in opposite directions:
- Convergence (adduction of both eyes): for near focus; mediated by the medial recti
- Divergence (abduction of both eyes): for far focus; mediated by the lateral recti
- Centers are in the midbrain reticular formation (separate pools for convergence and divergence), controlled by descending occipital and parietal cortex inputs
- These fibers do NOT travel in the caudal MLF, which is why convergence is often preserved in INO
Key takeaway: Conjugate eye movements are co-ordinated by the MLF, which links the abducens nucleus in the pons to the oculomotor nucleus in the midbrain. The PPRF serves as the horizontal gaze center receiving cortical commands, while the riMLF in the midbrain serves as the vertical gaze center. The frontal eye fields generate voluntary saccades contralaterally; smooth pursuit is mediated ipsilaterally by the parieto-occipital cortex.
Internuclear ophtalmopkegia and external ophtalmoplegia
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I have comprehensive information. Let me now compile the full answer.
Internuclear Ophthalmoplegia (INO) and External Ophthalmoplegia
PART 1: INTERNUCLEAR OPHTHALMOPLEGIA (INO)
Definition
INO is a disorder of conjugate horizontal gaze caused by a lesion in the medial longitudinal fasciculus (MLF) - the white matter tract that connects the abducens nucleus (CN VI, pons) to the contralateral oculomotor nucleus (CN III, midbrain).
Anatomy of the MLF Lesion
The MLF carries the signal from one abducens nucleus across to the contralateral medial rectus subnucleus of CN III. When the MLF is damaged:
- The ipsilateral eye fails to adduct on attempted horizontal gaze (medial rectus does not receive the command)
- The contralateral eye abducts with nystagmus (ataxic/dysmetric nystagmus - an overshoot due to increased innervation compensating for the weak medial rectus, per Hering's Law of dual innervation)
Key rule: INO is named for the side of the adduction deficit = the side of the MLF lesion
- Neuroanatomy through Clinical Cases, p. 614
- Kanski's Clinical Ophthalmology, p. 7058
Clinical Features
Symptoms:
- Most patients surprisingly have no symptoms
- When present: diplopia (horizontal), oscillopsia, blurred vision
Signs on examination:
| Feature | Detail |
|---|---|
| Adduction deficit | Weakness or complete paralysis of adduction ipsilateral to the lesion |
| Abducting nystagmus | Contralateral eye nystagmus on abduction (ataxic/dysmetric) |
| Convergence | Often preserved (convergence fibers travel separately, not in the caudal MLF) |
| Skew deviation | Vertical ocular misalignment (ipsilesional hypertropia); otolith-ocular pathway damage |
| Vertical pursuit | Abnormal - MLF also carries vertical pursuit and vertical VOR signals |
| Upbeat nystagmus | May be present on upgaze in both unilateral and bilateral INO |
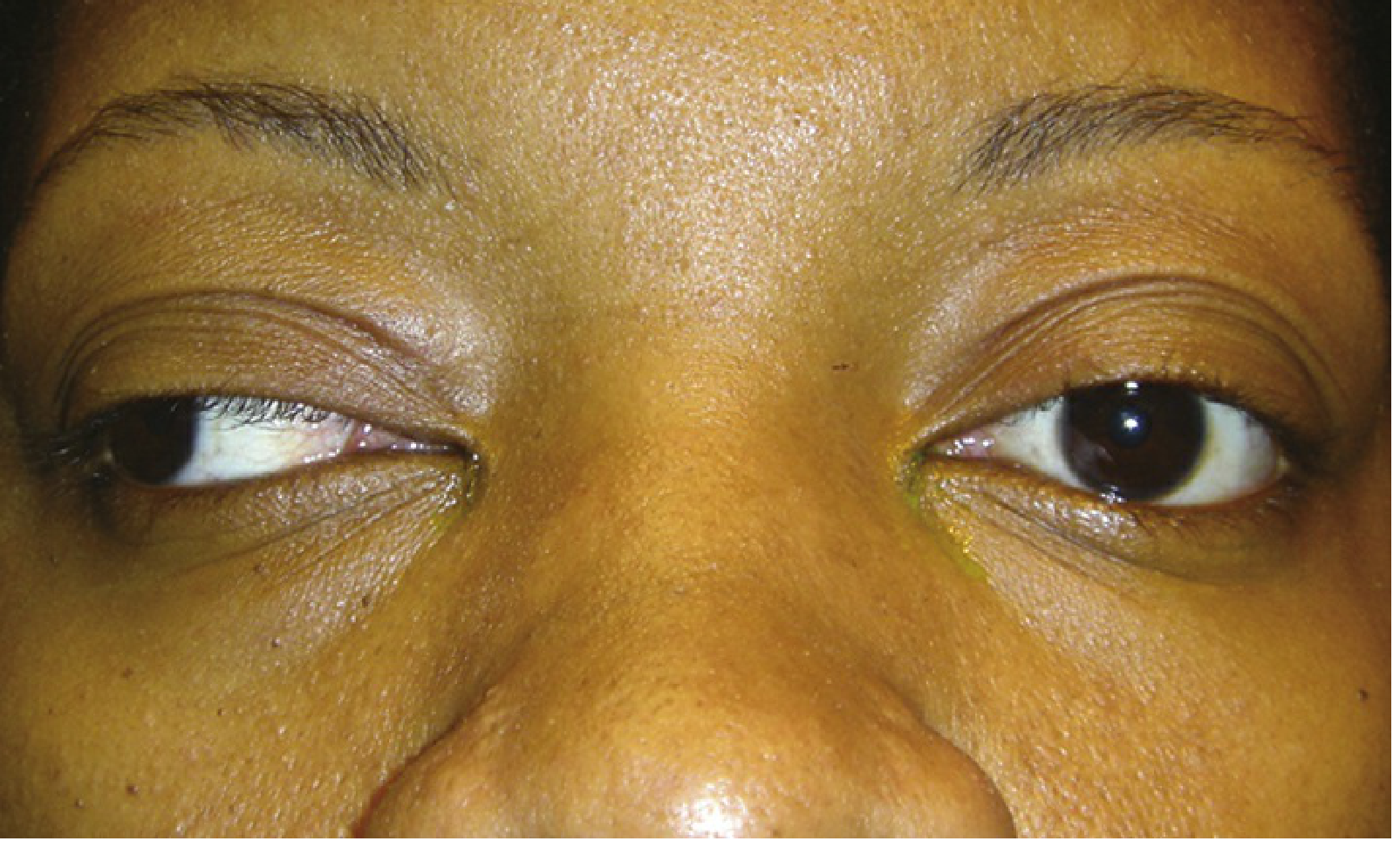
Figure: Left INO - Primary gaze (full abduction)

Figure: Left INO - Right gaze with severe adduction deficit of the left eye
Unilateral vs Bilateral INO
| Unilateral INO | Bilateral INO | |
|---|---|---|
| Adduction | One eye fails to adduct | Both eyes fail to adduct |
| Gaze to lesion side | Normal | Impaired |
| Primary position | Straight | Usually straight; may be exotropic |
| WEBINO | - | Yes, if bilateral exotropia present |
WEBINO (Wall-Eyed Bilateral INO):
-
Bilateral INO with bilateral exotropia (both eyes deviated laterally)
-
Usually from a rostral midbrain lesion causing additional convergence deficit
-
Bilateral INO + bilateral exotropia + abducting nystagmus
-
Kanski's Clinical Ophthalmology, p. 7067
-
Localization in Clinical Neurology, p. 615
Causes of INO
| Category | Specific causes |
|---|---|
| Young patients | Multiple sclerosis (most common - typically bilateral) |
| Older patients | Brainstem stroke (pontine infarct - typically unilateral) |
| Infections | Meningitis (TB, HIV, syphilis, brucellosis) |
| Tumors | Primary or metastatic brainstem tumors |
| Drugs/Toxic | Anticonvulsants, phenothiazines, tricyclics (coma); lithium (awake) |
| Inflammatory | Vasculitis, sarcoid, paraneoplastic, Wernicke encephalopathy |
| Neurodegenerative | Progressive supranuclear palsy, spinocerebellar degeneration |
| Metabolic | Fabry disease |
| Structural | Herniation (subdural/epidural hematoma), vascular malformations |
| Mimics (Pseudo-INO) | Myasthenia gravis (MG), Guillain-Barré, Miller Fisher syndrome, thyroid eye disease, orbital tumor |
- Bradley and Daroff's Neurology, p. 914-944
Related Syndromes
One-and-a-Half Syndrome
- Lesion involves both the PPRF/abducens nucleus AND the ipsilateral MLF
- Result: Ipsilateral gaze palsy ("one") + ipsilateral INO ("half")
- The only remaining horizontal movement is abduction of the contralateral eye (with nystagmus)
- Vertical movements and convergence are preserved
- The contralateral eye is often exotropic (paralytic pontine exotropia)
Lutz Posterior INO (INO of Abduction)
- Rare; caused by rostral pontine or mesencephalic lesion (not the classic MLF)
- Abduction is impaired (not adduction); adducting eye may show nystagmus
- Mechanism: impaired inhibition of the antagonist medial rectus via uncrossed PPRF-oculomotor fibers
Workup & Treatment
- MRI with thin cuts through the brainstem (may miss isolated INO on standard cuts)
- Exclude MG unless obligatory brainstem signs are present (ice test, rest test, edrophonium)
- Treat the underlying cause (MS: immunotherapy; stroke: risk factor management)
- Persistent diplopia: strabismus surgery may be considered
PART 2: EXTERNAL OPHTHALMOPLEGIA
Concept: Internal vs External Ophthalmoplegia
| Type | Structures Affected | Examples |
|---|---|---|
| External ophthalmoplegia | Extraocular muscles (moves the globe) | PEO, CN III/IV/VI palsies |
| Internal ophthalmoplegia | Intraocular muscles (pupil + ciliary body) | Argyll Robertson pupil, Adie's pupil |
| Total ophthalmoplegia | Both internal + external | Complete CN III palsy with blown pupil |
Chronic Progressive External Ophthalmoplegia (CPEO)
Definition: Slowly progressive, symmetrical paralysis of the extraocular muscles (and levator palpebrae), primarily of mitochondrial or myopathic origin.
Key features:
- Ptosis is usually the first sign (levator palpebrae affected first)
- Followed by progressive, symmetric ophthalmoplegia (all extraocular muscles involved symmetrically)
- No diplopia in most cases (because both eyes are equally affected and remain aligned)
- Normal pupils and accommodation
- Eyes eventually become motionless in central position
- Hutchinsonian facies: head thrown back, frontalis muscle contracted to lift lids
- Orbicularis oculi weakness (eye closure AND opening weakness = hallmark myopathic sign)
- ~25% have additional weakness of facial muscles, masseters, sternocleidomastoid, deltoids, peronei
Signs (Wills Eye Manual):
-
Critical: Ptosis + limitation of ocular motility + normal pupils + orthophoric
-
Other: Weak orbicularis, exposure keratopathy, limb/facial muscle weakness
-
Adams and Victor's Principles of Neurology, p. 1408-1409
Causes of CPEO
1. Mitochondrial DNA Disorders (Most Common)
| Disorder | Genetics | Key Features |
|---|---|---|
| Sporadic CPEO | Single large mtDNA deletion | CPEO + ptosis only; no systemic features |
| Kearns-Sayre Syndrome (KSS) | Sporadic mtDNA deletion | See below |
| MELAS | A3243G tRNA point mutation | Stroke-like episodes, lactic acidosis |
| Maternally inherited PEO | tRNA point mutations (Leu, Ile, Asn, Trp) | CPEO + variable systemic |
2. Nuclear Gene Disorders (Autosomal)
| Gene | Inheritance | Function |
|---|---|---|
| POLG (most common) | AD or AR | mtDNA polymerase - replication |
| Twinkle | AD | mtDNA helicase - replication |
| ANT1 | AD | Adenine nucleotide transporter across inner mitochondrial membrane |
These cause multiple mtDNA deletions (unlike sporadic mtDNA single deletions).
Kearns-Sayre Syndrome (KSS) - The Classic CPEO Syndrome
Diagnostic Triad:
- CPEO (onset before age 20)
- Pigmentary retinopathy (salt-and-pepper appearance, not typical RP)
- At least ONE of: cardiac conduction defect (heart block), cerebellar ataxia, or CSF protein >100 mg/dL
Additional features:
-
Hearing loss, short stature, cognitive impairment, delayed puberty
-
Nephropathy, vestibular abnormalities
-
Ragged-red fibers on muscle biopsy (Gomori trichrome stain) - mitochondrial accumulation
-
Cause: Sporadic single large mtDNA deletion (arising in mother's oocyte)
-
Course: Progressive; many die in 3rd-4th decade from cardiac or CNS complications
-
Pacemaker often required for AV block (risk of sudden death)
-
Bradley and Daroff's Neurology, p. 1598
Differential Diagnosis of CPEO
| Condition | Key Distinguishing Features |
|---|---|
| Myasthenia gravis | Ptosis + fatigability + diurnal variation; ptosis worsens with sustained upgaze; orbicularis weakness; responds to edrophonium/ice test |
| Progressive supranuclear palsy | Downgaze affected first; axial rigidity; "staring" expression; vertical > horizontal |
| Oculopharyngeal dystrophy | Late onset (>45 yrs); dysphagia; autosomal dominant; PABPN1 mutation |
| Abetalipoproteinemia | Acanthocytosis; retinal pigmentation; ataxia; elevated CSF protein |
| Refsum disease | Retinitis pigmentosa; elevated phytanic acid; polyneuropathy |
| Thyroid eye disease | Exophthalmos; lid retraction; pain; restriction (not paralysis) |
| MELAS | Children/young adults; stroke-like episodes; lactic acidosis on MRI |
- The Wills Eye Manual, pp. 690-691
Workup of CPEO
- History: rate of onset (gradual = myopathic; sudden = CN disease), family history
- Examine pupils and ocular motility carefully
- Test orbicularis strength
- Fundus: look for diffuse pigmentary changes (KSS)
- Check swallowing (oculopharyngeal dystrophy)
- Ice test / rest test / edrophonium to exclude MG
- ECG (yearly) if KSS suspected - AV block can cause sudden death
- Serum CK, lactate; CSF lactate and protein
- Muscle biopsy: ragged-red fibers
- Genetic testing: mtDNA deletion screen (blood if <20 yrs), POLG/Twinkle/ANT1 sequencing
- Lipoprotein electrophoresis if abetalipoproteinemia suspected; serum phytanic acid if Refsum suspected
Key Comparison: INO vs External Ophthalmoplegia
| Feature | INO | CPEO |
|---|---|---|
| Level of lesion | White matter tract (MLF) - supranuclear | Muscle/mitochondria - myopathic |
| Type | Specific adduction failure + contralateral nystagmus | Symmetric, progressive, all movements |
| Diplopia | Often yes (at least transiently) | Rarely (symmetric involvement) |
| Pupils | Normal | Normal |
| Convergence | Often preserved | Affected eventually |
| Cause | MS, stroke | Mitochondrial disease, nuclear gene mutations |
| Associated signs | Other brainstem signs | Ptosis, ragged-red fibers, systemic features |
Clinical evaluation of nystagmus
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
I now have all the essential content. Here is the comprehensive answer:
Clinical Evaluation of Nystagmus
1. Definition
Nystagmus is an involuntary, biphasic, rhythmic oscillation of the eyes in which one or both phases are slow. It reflects an imbalance in one or more of the systems that maintain gaze stability:
- Systems maintaining steady gaze in primary position
- The neural integrator (NI) - holds eyes in eccentric gaze positions
- The vestibulo-ocular reflex (VOR) - maintains foveal fixation during head movement
The slow phase is the pathological component (initiates/generates nystagmus). The fast phase is corrective (saccadic reset). By convention, nystagmus is named by the direction of the fast phase - described as "beating" in that direction.
- Adams and Victor's Principles of Neurology, p. 292
2. Classification by Waveform
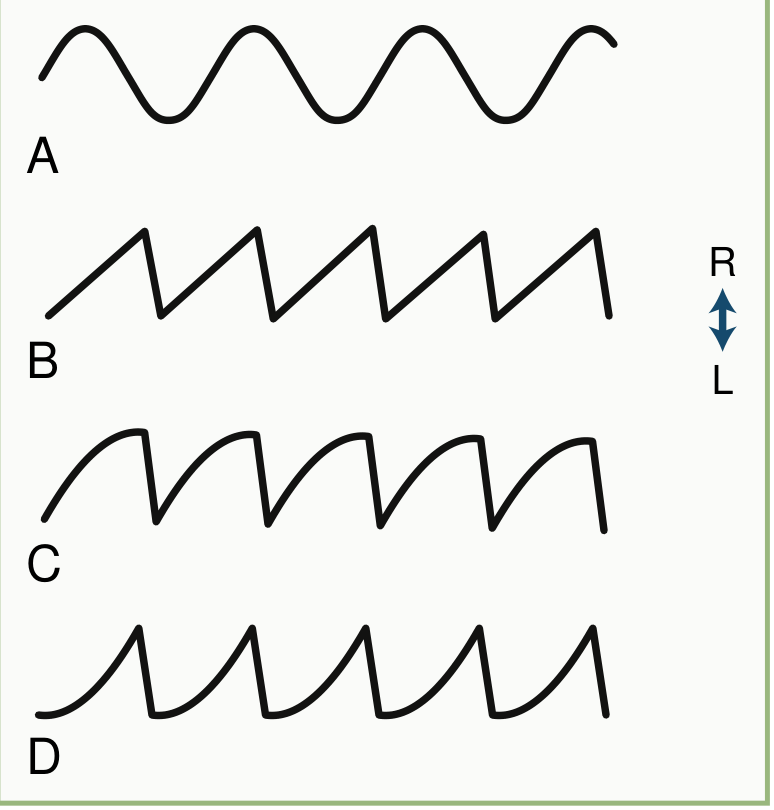
Fig. 18.26 - Nystagmus Waveforms: A=Pendular, B=Jerk/linear slow phase (vestibular), C=Jerk/decreasing velocity (leaky NI/gaze-paretic), D=Jerk/increasing velocity (congenital/central)
| Waveform | Description | Origin |
|---|---|---|
| Pendular | Back-to-back slow phases; quasi-sinusoidal; no distinct fast phase | Always central (brainstem/cerebellum) or congenital/visual loss |
| Jerk | Slow drift + fast corrective saccade | Peripheral OR central |
| Jerk - linear slow phase (constant velocity) | Sawtooth waveform | Vestibular (peripheral or central) imbalance |
| Jerk - decreasing velocity exponential | Slow phase slows toward end | "Leaky" neural integrator - gaze-paretic nystagmus |
| Jerk - increasing velocity exponential | Slow phase accelerates | Central; typical of congenital/infantile nystagmus (INS) |
Key rule: Pendular nystagmus = always central; Jerk nystagmus = peripheral OR central
- Bradley and Daroff's Neurology, p. 312
3. Clinical Examination Checklist (BOX 18.12)
A structured approach to examining nystagmus:
- Is nystagmus present in primary position, or only with eccentric gaze?
- Is it binocular/conjugate, or dissociated (different in each eye)? - Dissociated = brainstem lesion (MLF)
- Waveform: pendular or jerk? - If jerk, what direction is the fast phase?
- Plane: Horizontal / vertical / torsional / mixed?
- Is there a latent component? (intensifies when one eye covered = latent nystagmus)
- Is there a torsional component?
- Does direction alternate spontaneously? - Periodic alternating nystagmus (PAN)
- Is there a null zone? (direction where nystagmus is minimal) - suggests congenital nystagmus
- Does convergence damp or alter the nystagmus?
- Is it positional? (Dix-Hallpike, supine roll)
- Provocative maneuvers: elimination of fixation (Frenzel glasses), head shaking, hyperventilation, mastoid vibration
- Effect of optokinetic stimulation (paradoxical in INS - fast phase goes with slow target)
- Associated rhythmic movements: palate (oculopalatal myoclonus), limbs, face
- Bradley and Daroff's Neurology, p. 312-313
4. Peripheral vs Central Nystagmus - Key Differentiation
| Feature | Peripheral Vestibular | Central |
|---|---|---|
| Direction | Unidirectional (never changes) | May be bidirectional (changes with gaze direction) |
| Plane | Mixed horizontal + torsional | Can be purely vertical, horizontal, or torsional |
| Fixation | Suppressed by visual fixation | Not suppressed (or minimal effect) |
| Frenzel glasses | Nystagmus increases in dark | Little change or may decrease |
| Fast phase direction | Alexander's law: increases with gaze toward fast phase | Variable |
| Associated symptoms | Severe vertigo, nausea, vomiting, hearing loss, tinnitus | Milder vertigo; headache, ataxia, diplopia, pyramidal signs |
| Onset | Abrupt; resolves in days | Often persistent or progressive |
| Head impulse test (HIT) | Positive (corrective saccade seen) | Negative (no corrective saccade - eye stays on target) |
Important rule: Purely vertical nystagmus always indicates brainstem dysfunction (central)
- Scott-Brown's Otorhinolaryngology, p. 837
- Bradley and Daroff's Neurology, p. 4101
5. The HINTS Exam (for Acute Vestibular Syndrome)
Used in patients with continuous vertigo + nystagmus (lasting hours to days) to distinguish vestibular neuritis (peripheral) from cerebellar stroke (central). More sensitive than early MRI.
| Test | Peripheral (reassuring) | Central (alarming - suggests stroke) |
|---|---|---|
| H - Head Impulse Test | Positive (corrective saccade) | Negative (no saccade) |
| IN - Nystagmus type | Unidirectional, horizontal-torsional | Direction-changing with gaze (bidirectional) |
| TS - Test of Skew | Absent (no vertical realignment) | Present (skew deviation on cover-uncover test) |
| (+) Hearing loss | May be present in vestibular neuritis | Suggests AICA territory stroke |
A negative HIT + direction-changing nystagmus + skew deviation = "HINTS positive" = HIGH risk of stroke
- Tintinalli's Emergency Medicine, p. 1191
6. Localizing Value of Specific Nystagmus Syndromes
(Table 10.4 from Bradley & Daroff)
| Nystagmus Type | Localization |
|---|---|
| Downbeat nystagmus | Bilateral cervicomedullary junction (flocculus); Arnold-Chiari; spinocerebellar diseases |
| Upbeat nystagmus | Bilateral pontomesencephalic junction; Wernicke encephalopathy; MS |
| Periodic alternating nystagmus (PAN) | Floor of fourth ventricle (nodulus/uvula) |
| Pendular nystagmus | Medial medulla; MS; bilateral visual loss |
| Torsional nystagmus (jerk) | Central vestibular system |
| Torsional nystagmus (pendular) | Medial medulla; olivary hypertrophy |
| Rebound nystagmus | Cerebellum (ONLY form specific for cerebellar lesions) |
| Gaze-evoked nystagmus | Non-specific; drugs, MS, myasthenia gravis, cerebellar atrophy |
| Bruns nystagmus | Cerebellopontine angle, AICA territory stroke |
| Seesaw nystagmus | Parasellar (bitemporal visual loss), midbrain; congenital |
| Convergence-retraction nystagmus | Dorsal midbrain (Parinaud syndrome) |
7. Key Nystagmus Types in Detail
A. Gaze-Evoked Nystagmus (GEN)
- Present only on eccentric gaze, in the direction of gaze
- Most common cause: drugs (phenobarbital, phenytoin, alcohol, benzodiazepines)
- Also: MS, myasthenia gravis, cerebellar atrophy
- Asymmetric GEN with larger amplitude on one side (Bruns nystagmus) = cerebellopontine angle lesion (lesion on side of larger amplitude nystagmus)
- Rebound nystagmus: GEN that reverses direction when eyes return to primary position = specific for cerebellum
B. Downbeat Nystagmus
- Slow upward drifts + fast downward resets; worsened in lateral gaze and head-hanging
- Most common: idiopathic; Arnold-Chiari malformation; cerebellar degeneration; drugs (lithium, anticonvulsants, amiodarone)
- Perverted nystagmus (downbeat after horizontal head shaking) = definite CNS disease
- Treat: 4-aminopyridine/dalfampridine, clonazepam, chlorzoxazone; base-out prisms if convergence damps it
C. Upbeat Nystagmus
- Spontaneous; fast phase upward in primary position; increases on upgaze
- Most common: Wernicke encephalopathy, MS
- Upbeat converting to downbeat = specific for Wernicke
- Bilateral pontomesencephalic lesions affecting perihypoglossal nuclei
D. Periodic Alternating Nystagmus (PAN)
- Nystagmus that spontaneously reverses direction every ~90-120 seconds
- Localization: nodulus/uvula of cerebellum; Arnold-Chiari
- Treatment: baclofen (very effective)
E. Peripheral Vestibular (Labyrinthine) Nystagmus
- Mixed horizontal + torsional (horizontal component dominant due to horizontal canal asymmetry)
- Unidirectional - never changes direction
- Alexander's Law: nystagmus increases looking toward fast phase, decreases looking toward slow phase
- Suppressed by fixation
- Associated with severe vertigo, nausea, hearing loss, tinnitus
F. Pendular Nystagmus (Acquired)
- Most common cause: multiple sclerosis (horizontal or elliptical, 3-5 Hz)
- Also: brainstem vascular disease, Whipple disease, Pelizaeus-Merzbacher disease, toluene abuse
- Mechanism: disruption of cerebellar nuclear feedback to neural integrators; inferior olive instability
- Treatment: memantine, gabapentin, clonazepam
G. Congenital/Infantile Nystagmus Syndrome (INS)
- High frequency, pendular waveform; null zone present (position of least nystagmus)
- Horizontal even on vertical gaze; absent in sleep
- Increasing velocity exponential slow phase on oculography
- Paradoxical OKN response (fast phase toward slow-moving target)
- Patients often unaware of it despite wide amplitude
H. Positional Nystagmus - BPPV
- Dix-Hallpike test: patient sits, head turned 45° toward affected ear, then quickly lowered to head-hanging position
- Posterior canal BPPV: upbeat + torsional nystagmus toward the affected (lower) ear
- Latency: 1-5 sec after positioning
- Duration: <1 minute
- Fatigues with repeated testing
- Horizontal canal BPPV (roll test): horizontal nystagmus beating toward the ground (geotropic) or away from the ground (apogeotropic) in the lateral head position
8. Oscillopsia
The subjective sensation of environmental movement (objects appear to oscillate). Caused by:
- Coarse nystagmus of any type
- Impaired VOR (aminoglycoside toxicity) - oscillopsia only during movement (walking, riding)
- Superior oblique myokymia - episodic, monocular, brief torsional oscillopsia
9. Summary: Quick Diagnostic Framework
NYSTAGMUS
|
├── Pendular → CENTRAL (MS, brainstem/cerebellar lesion, congenital, visual loss)
|
└── Jerk
|
├── Purely Vertical (up/downbeat) → ALWAYS CENTRAL (brainstem/cerebellum)
|
├── Unidirectional, horizontal-torsional, suppressed by fixation
| → PERIPHERAL VESTIBULAR (labyrinth or VIII nerve)
|
├── Direction-changing with gaze → CENTRAL
|
├── Only on eccentric gaze (gaze-evoked) → NI dysfunction (drugs, cerebellum)
|
└── Positional (Dix-Hallpike) → BPPV (torsional-upbeat + latency + fatigues)
- Goldman-Cecil Medicine, p. 4148
- Bradley and Daroff's Neurology, pp. 312-316
This is a shared conversation. Sign in to Orris to start your own chat.