Msa c msa p
Asking for Preferences
Reading File
Finding Sources
Searching PubMed
"multiple system atrophy" MSA-C MSA-P
Reading File
Reading File
Reading File
Reading File
Reading File
Excellent material. Here is a thorough comparison of MSA-C and MSA-P:
Multiple System Atrophy: MSA-C vs MSA-P
What is MSA?
Multiple System Atrophy (MSA) is a sporadic, progressive neurodegenerative disorder (synucleinopathy) characterized by a triad of:
- Autonomic dysfunction (orthostatic hypotension, urogenital failure)
- Parkinsonism
- Cerebellar ataxia
It was previously known by three names that are now considered subtypes of the same disease: Shy-Drager syndrome, striatonigral degeneration, and olivopontocerebellar atrophy (OPCA).
Epidemiology:
- Mean age of onset: ~54 years
- Prevalence: ~4-5 per 100,000
- Annual incidence: ~3 per 100,000
- Mean survival: 5.7-9 years from symptom onset
- No gender predilection
MSA-P vs MSA-C: Side-by-Side Comparison
| Feature | MSA-P (Parkinsonian) | MSA-C (Cerebellar) |
|---|---|---|
| Former name | Striatonigral degeneration | Olivopontocerebellar atrophy (OPCA) |
| Predominant feature | Parkinsonism | Cerebellar ataxia |
| More common in | European populations (~58%) | Japanese populations (~84%) |
| Parkinsonism type | Symmetric, often no resting tremor, poor/absent L-dopa response, rapid progression | Parkinsonism present but cerebellar signs dominate; partial/transient L-dopa response possible |
| Cerebellar signs | Less prominent | Wide-based ataxic gait, limb ataxia, dysarthria (cerebellar) |
| MRI findings | T2 hyperintense lateral putaminal rim; T2 hypointensity of posterior putamen | Atrophy of pons, cerebellum, middle cerebellar peduncles; "hot cross bun" sign on T2 (cruciform pontine hyperintensity); T2 hyperintensity in middle cerebellar peduncles |
| Ataxia progression | Slower | Faster than other degenerative ataxias |
| Falls/instability | Early | Present |
| Diplopia | Less common | Intermittent diplopia may occur |
Shared Features (Both Subtypes)
Autonomic Dysfunction (cardinal feature in both)
- Orthostatic hypotension (OH): Drop of ≥30 mmHg systolic or ≥15 mmHg diastolic on standing - required for probable MSA
- Urinary dysfunction: Urgency, frequency, retention - large post-void residual is a clue favoring MSA over PD
- Erectile dysfunction in males
- Sweating dysfunction / anhidrosis (central pattern on thermoregulatory sweat testing)
- Bowel dysfunction (constipation, fecal incontinence)
- REM sleep behavior disorder (RBD) - strongly associated with MSA
Motor Features
- Pyramidal signs
- Stridor (laryngeal / nocturnal) - important red flag
- Dysarthria (early hypokinetic)
- Dysphagia
- Oculomotor dysfunction
- Orofacial dystonia
- Distal myoclonus
- Pseudobulbar affect / emotional lability
Cognitive/Psychiatric
- Significant dementia is rare and is a red flag against MSA diagnosis
- Executive deficits and slowed processing speed may occur on neuropsychological testing
- Depression and anxiety are common
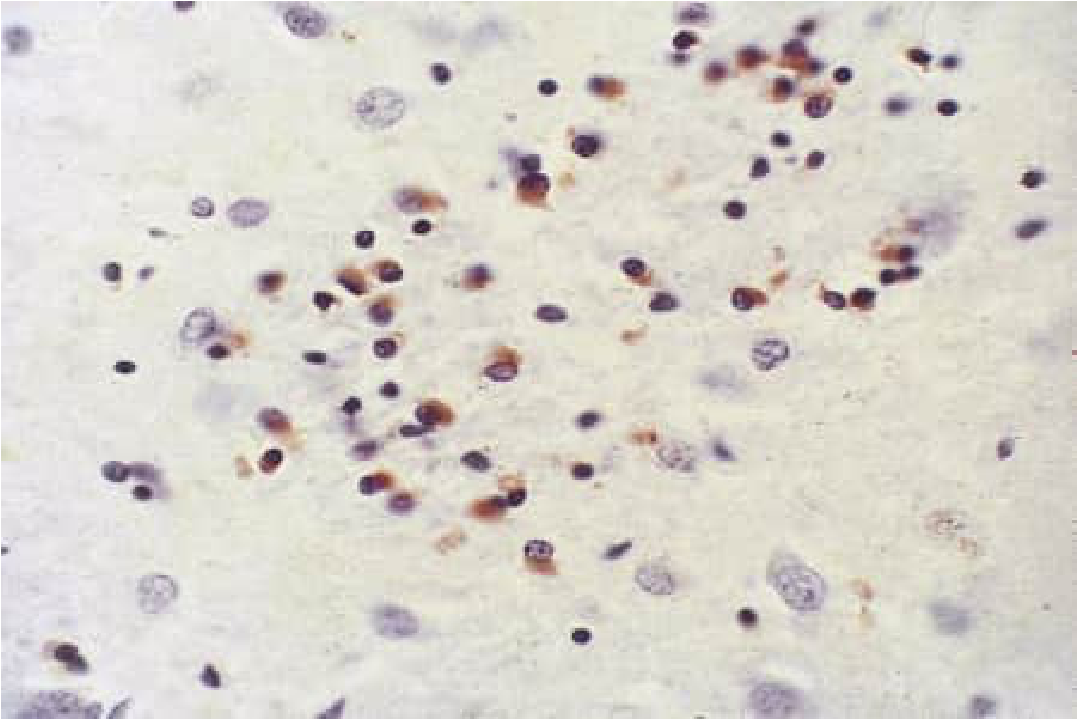
Pathological Hallmark
The defining histological feature is glial cytoplasmic inclusions (GCIs) containing α-synuclein and ubiquitin in oligodendrocytes.
GCIs differ from Lewy bodies (seen in PD) in three key ways:
- Shape: GCIs are irregular; Lewy bodies are concentric/target-shaped
- Cell type: GCIs are in glia (oligodendrocytes); Lewy bodies are in neurons
- Location in neuraxis: GCIs dominate in basal ganglia and pons; Lewy bodies dominate in midbrain, cortex, and autonomic ganglia
At autopsy, neuronal loss and gliosis are seen in: striatum, substantia nigra, locus coeruleus, inferior olive, pontine nuclei, Purkinje cells, intermediolateral cell column, and Onuf's nucleus (sacral cord).
Diagnosis
Probable MSA requires:
- Autonomic failure (OH or urinary dysfunction)
- Plus parkinsonism (poor L-dopa response) OR cerebellar ataxia
Red Flags for MSA-P (any 2 of 6 increase specificity):
- Early instability/falls
- Rapid progression
- Abnormal postures (Pisa syndrome, anterocollis, hand/foot contractures)
- Bulbar dysfunction (dysphonia, dysarthria, dysphagia)
- Respiratory dysfunction (inspiratory stridor, inspiratory sighs)
- Emotional incontinence (inappropriate crying/laughing)
Investigations:
- Autonomic testing: Heart rate variability, head-up tilt, thermoregulatory sweat test
- MRI brain: Patterns differ by subtype (see table above) - "hot cross bun" sign is characteristic of MSA-C
- Rectal sphincter EMG: Denervation is characteristic
- FDG-PET: Hypometabolism in basal ganglia and cerebellum
- Growth hormone response to clonidine: Blunted in MSA
- CSF/serum neurofilament light (NFL) protein: Elevated in MSA (not PD) but doesn't differentiate from other atypical parkinsonism
Differentiating MSA from Parkinson's Disease
| Feature | MSA | PD |
|---|---|---|
| Rest tremor | Typically absent (MSA-P) | Classic feature |
| L-dopa response | Poor/absent or transient | Good, sustained |
| Dementia | Rare | Common later |
| Autonomic dysfunction | Early, severe | Present but later/milder |
| Post-void residual | Large early | Less prominent |
| Progression | Faster | Slower |
| Wheelchair dependency | ~5 years from onset | Much later |
Treatment (Symptomatic Only - No Disease-Modifying Therapy Exists)
| Symptom | Management |
|---|---|
| Orthostatic hypotension | Liberal salt/water, compression stockings, head-up sleeping; pharmacotherapy: fludrocortisone, midodrine, droxidopa |
| Parkinsonism | L-dopa (partial/short-lived benefit early in MSA-P); dopamine agonists poorly tolerated due to OH |
| Cerebellar signs | No effective treatment |
| Urinary retention | Self-catheterization if severe |
| Depression | SSRIs |
| Supine hypertension | Carefully manage (often worsened by OH treatment) |
Prognosis: Poor. 10-year survival is rare. Common causes of death: pulmonary embolism, apnea (Ondine curse from sleep apnea/respiratory drive failure), aspiration pneumonia, intercurrent infection.
Sources: Bradley and Daroff's Neurology in Clinical Practice, Chapters on Autonomic Disorders and Movement Disorders
This is a shared conversation. Sign in to Orris to start your own chat.