Gout
Reading File
Finding Sources
Searching PubMed
"gout"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Reading File
Searching PubMed
gout hyperuricemia urate lowering therapy
Loading Image
Reading File
Finding Sources
Loading Image
Finding Sources
I now have comprehensive content to synthesize a thorough answer. Here is the full review of gout:
Gout
Gout is a crystal deposition arthropathy caused by the precipitation of monosodium urate (MSU) crystals in joints and periarticular tissues. It affects approximately 4% of adults in the US, impacting ~5% of adult males and ~3% of adult females, and becomes more prevalent with age. - Rosen's Emergency Medicine, p. 2337
Pathophysiology
Uric acid is the end product of purine catabolism in humans. Hyperuricemia (plasma urate >6.8 mg/dL) is necessary but not sufficient for gout - only ~10% of hyperuricemic individuals develop the disease.
Uric acid accumulates by two mechanisms:
- Reduced renal excretion (most common, ~90% of primary gout) - uric acid is filtered at the glomerulus, almost completely reabsorbed in the proximal tubule, and a small fraction secreted distally
- Overproduction (~10%) - excessive purine catabolism, dietary purines, or enzymatic defects
Why crystals cause inflammation: Urate crystals precipitate from supersaturated extracellular fluid and are phagocytosed by synovial macrophages → activate the NLRP3 inflammasome → caspase-1 activation → IL-1β production → massive neutrophil recruitment → cytokines, free radicals, proteases, and lysosomal enzyme release. This produces the acute hot, swollen joint. - Robbins & Kumar Basic Pathology, p. 850
Causes and Risk Factors
| Category | Examples |
|---|---|
| Primary gout | Idiopathic reduced renal excretion |
| Enzymatic defects | Partial HGPRT deficiency (gout); complete HGPRT deficiency (Lesch-Nyhan syndrome - hyperuricemia + neurological features) |
| Increased production | Tumor lysis syndrome, myeloproliferative disorders, psoriasis |
| Reduced excretion | Chronic kidney disease, thiazide diuretics, cyclosporin, low-dose aspirin |
| Dietary | Purine-rich foods: red meat, organ meats, shellfish, anchovies, beer, legumes |
| Comorbidities | Obesity, hypertension, diabetes, metabolic syndrome |
Clinical Stages
1. Asymptomatic Hyperuricemia
Elevated serum uric acid without symptoms. May persist for 20-30 years before a gout attack. Serum uric acid level does not correlate well with the frequency or severity of attacks.
2. Acute Gouty Arthritis
- Classic presentation: sudden-onset, exquisite joint pain - often waking the patient from sleep
- Peak symptoms within 1-2 days, self-limited resolution within 1 week
- Podagra (first metatarsophalangeal joint) is the most common site (~50% of first attacks)
- Other common joints: ankle, knee, tarsal joints, wrist, fingers
- Up to 20% of attacks are polyarticular
- Systemic fever may be present - raises concern for septic arthritis
- Associated bursitis, tenosynovitis, or skin erythema can mimic cellulitis

3. Intercritical Gout
Asymptomatic periods between attacks. Without treatment, attacks become more frequent, longer in duration, and involve more joints over time.
4. Chronic Tophaceous Gout
- Tophi - gritty, chalk-like nodules of MSU crystal aggregates + inflammatory tissue
- Common locations: subcutaneous tissue (helix of ear, olecranon, Achilles tendon), bursae, joint space, soft tissue
- Generally painless but can cause bony erosion, joint destruction, and deformity
- Develops after years of untreated hyperuricemia
Diagnosis
Gold Standard: Arthrocentesis
Synovial fluid analysis showing monosodium urate crystals under polarizing microscopy:
- Negatively birefringent under compensated polarized light (yellow when parallel to the axis)
- Needle-shaped
- WBC typically 20,000-100,000 cells/mm³ (neutrophil predominant)
First-time presentations warrant arthrocentesis to exclude septic arthritis. Established gout without risk factors for infection may be treated empirically.
Serum Uric Acid
- Unreliable during acute attack (levels may be normal or even low)
- Useful for monitoring treatment targets
- Target: <6 mg/dL (or <5 mg/dL in tophaceous disease)
Imaging
Plain X-ray: Normal in early disease. Late findings - asymmetric, sclerotic "rat-bite" erosions at joint margins (outside the joint capsule, preserving joint space), overhanging edges of bone.
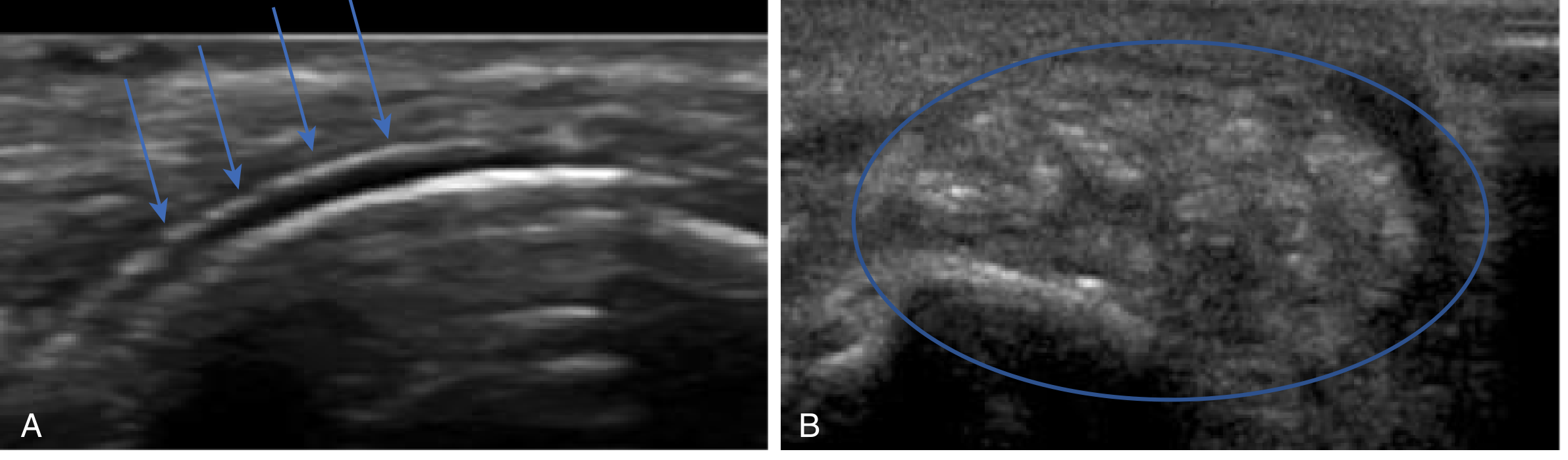
Ultrasound: Increasingly used:
- Double contour sign - irregular hyperechoic line along articular cartilage surface (crystals + bony surface below)
- Tophi appear as "wet clumps of sugar" - heterogeneous center with hypoechoic rim
DECT (Dual Energy CT): Highly specific for urate deposits; can identify tophi throughout the body.
Management
Acute Flare Treatment
There is no strong evidence favoring one agent over another - choice depends on comorbidities and tolerability.
| Drug | Mechanism | Notes |
|---|---|---|
| NSAIDs (indomethacin, naproxen, ibuprofen) | COX inhibition → reduced prostaglandins | First-line if no contraindications; start promptly; continue 24h after resolution. Avoid in PUD, GI bleeding, renal insufficiency |
| Colchicine | Inhibits microtubule polymerization → blocks neutrophil migration and inflammasome | Low-dose preferred (1.2 mg then 0.6 mg 1h later); avoid in renal/hepatic failure; narrow therapeutic window; GI side effects common |
| Corticosteroids | Broad anti-inflammatory | Oral prednisone 40 mg/day x 5-7 days, or intra-articular injection; use when NSAIDs/colchicine contraindicated; avoid intra-articular in possible septic arthritis |
- Combination therapy (e.g., intra-articular steroid + colchicine) for debilitating or polyarticular attacks
- Do not start urate-lowering therapy during an acute flare (can prolong it), but continue existing therapy if already on it
Long-Term Urate-Lowering Therapy (ULT)
Indications for ULT:
- ≥2 attacks/year
- Chronic kidney disease
- Urolithiasis
- Tophi present
- Serum urate persistently very high
Goal: Serum urate <6 mg/dL (symptomatic disease); <5 mg/dL (tophaceous disease)
| Drug | Mechanism | Dosing | Notes |
|---|---|---|---|
| Allopurinol | Xanthine oxidase inhibitor (purine analog) | Start 100 mg/day; titrate by 100 mg q4 weeks. Dose-adjust for renal function | First-line; risk of severe hypersensitivity (DRESS) - HLA-B*5801 testing in high-risk populations (Han Chinese, Thai, Korean) |
| Febuxostat | Xanthine oxidase inhibitor (non-purine) | 40-80 mg/day; no renal dose adjustment | Use in allopurinol intolerance; the CARES trial showed higher CV mortality vs. allopurinol in high-CV-risk patients |
| Probenecid | Uricosuric - inhibits URAT1 reabsorption | 500 mg BID, titrate to max 2g/day | Avoid in urolithiasis or GFR <30 mL/min |
| Pegloticase | Recombinant pegylated uricase - converts urate → allantoin | IV infusion q2 weeks | Reserved for refractory tophaceous gout; anti-drug antibodies cause loss of efficacy and infusion reactions |
Flare prophylaxis during ULT initiation (first 3-6 months): low-dose colchicine 0.6 mg/day or low-dose NSAIDs to prevent mobilization flares as urate dissolves from tissues.
Lifestyle Modifications
- Limit purine-rich foods (organ meats, shellfish, red meat)
- Avoid beer and spirits; moderate wine intake acceptable
- Increase hydration
- Avoid fructose-sweetened beverages
- Weight loss in obese patients
- Review and substitute uricogenic medications (thiazides, low-dose aspirin) when possible
Special Situations
Renal transplant recipients: NSAIDs generally avoided; colchicine or increased steroids preferred. Allopurinol must be used cautiously and at lower doses (reduced GFR → oxypurinol toxicity). Critical interaction: allopurinol + azathioprine - reduce azathioprine dose by 75% or switch to mycophenolate. - Comprehensive Clinical Nephrology, p. 1452
CKD patients: A 2024 meta-analysis (PMID: 38395818) found that urate-lowering therapy may have renoprotective effects in CKD patients with asymptomatic hyperuricemia, though the magnitude of benefit remains uncertain.
Cardiovascular outcomes: A 2024 meta-analysis (PMID: 39636389) found urate-lowering therapy was associated with reduced all-cause and CVD-specific mortality in gout patients, though febuxostat carries a specific CV safety concern in high-risk patients.
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Pseudogout (CPPD) | Calcium pyrophosphate crystals - positively birefringent, rhomboid-shaped; affects larger joints (knee > wrist) |
| Septic arthritis | Joint fluid WBC >50,000-100,000; gram stain/culture positive; fever; IV antibiotics required urgently |
| Cellulitis | No joint effusion; uric acid normal; no crystals |
| Rheumatoid arthritis | Symmetric small joint involvement; RF/anti-CCP positive; morning stiffness |
Key Crystal Comparison
| Feature | Gout (MSU) | Pseudogout (CPPD) |
|---|---|---|
| Crystal shape | Needle-shaped | Rhomboid |
| Birefringence | Negatively birefringent (yellow parallel) | Positively birefringent (blue parallel) |
| Common joint | 1st MTP (podagra) | Knee, wrist |
| X-ray | Erosions, overhanging edges | Chondrocalcinosis |
Sources: Robbins & Kumar Basic Pathology; Rosen's Emergency Medicine; Comprehensive Clinical Nephrology, 7th Edition; Swanson's Family Medicine Review
This is a shared conversation. Sign in to Orris to start your own chat.