



Mention etiology agents of pyogenic entities, discuss tge pathogenesis, clinical features and laboratory diagonsis of acute meningitis caused by any on of them meniingcococcal meningitis perfect answer for a 10 marker for micro mbbs exam
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
Addison
Asking for Preferences
Reading File
Finding Sources
Searching the Web
Addison's disease etiology pathogenesis clinical features lab diagnosis MBBS exam
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I have everything needed for a thorough, exam-ready answer. Here it is:
Addison's Disease (Primary Adrenocortical Insufficiency)
Definition
Addison's disease is primary adrenocortical insufficiency caused by destruction or dysfunction of the adrenal cortex bilaterally, leading to deficiency of all three classes of adrenocortical hormones - glucocorticoids (cortisol), mineralocorticoids (aldosterone), and adrenal androgens.
Etiology
1. Autoimmune adrenalitis (most common in developed countries - ~90% of cases)
- Autoimmune destruction of all zones of the adrenal cortex
- Associated with anti-21-hydroxylase antibodies
- May occur as an isolated condition or as part of Autoimmune Polyglandular Syndrome (APS):
- APS Type 2 (most common, ~70%): associated with type 1 DM, autoimmune thyroid disease, celiac disease; linked to HLA-DRB1 mutation
- APS Type 1 (~10%): AIRE gene mutation (chromosome 21q22.3); chronic candidiasis + hypoparathyroidism + Addison's
2. Tuberculosis (most common worldwide)
- Mycobacterium tuberculosis infiltrates and destroys adrenal glands
- Adrenal involvement in ~6% of active TB cases
3. Waterhouse-Friderichsen Syndrome
- Bilateral adrenal hemorrhage due to septicemia (classically Neisseria meningitidis, also Pseudomonas aeruginosa)
- Endotoxin-induced adrenal infarction
4. Other causes:
- Fungal infections (histoplasmosis, cryptococcosis)
- HIV/AIDS
- Metastatic carcinoma (lung, breast, renal - bilateral adrenal metastases)
- Amyloidosis, hemochromatosis
- Drugs inhibiting adrenal steroidogenesis: ketoconazole, fluconazole, etomidate, rifampicin
- Bilateral adrenalectomy
- Vascular: SLE, antiphospholipid syndrome, heparin-induced thrombocytopenia
Pathogenesis
The adrenal cortex has a functional reserve; symptoms appear only when >90% of cortical tissue is destroyed.
Three hormone deficiencies drive the clinical picture:
| Hormone Lost | Consequence |
|---|---|
| Cortisol (glucocorticoid) | Hypoglycemia, weakness, weight loss, nausea/vomiting, inability to mount stress response |
| Aldosterone (mineralocorticoid) | Sodium loss, potassium retention → hyponatremia, hyperkalemia, metabolic acidosis, hypotension, circulatory collapse |
| Adrenal androgens (DHEA, androstenedione) | Decreased pubic/axillary hair and libido in women |
Hyperpigmentation mechanism (key concept):
- Low cortisol → loss of negative feedback → pituitary releases excess ACTH
- ACTH contains the alpha-MSH (melanocyte-stimulating hormone) fragment
- Excess ACTH stimulates melanocytes → bronze hyperpigmentation
- This finding confirms the cause is PRIMARY (adrenal) insufficiency - it would not occur in secondary (pituitary) insufficiency where ACTH is low
Addisonian crisis occurs when glucocorticoid + mineralocorticoid deficiency combine - typically triggered by infection, trauma, surgery, or sudden steroid withdrawal - causing circulatory collapse and life-threatening shock.
Clinical Features
Onset is insidious and progressive (incubation/symptom onset over months-years):
Constitutional (from cortisol deficiency)
- Fatigue, weakness, lethargy (most common presenting complaint)
- Anorexia, nausea, vomiting
- Weight loss
- Hypoglycemia (especially in fasting states)
Cardiovascular (from aldosterone deficiency)
- Postural hypotension / dizziness on standing (orthostatic hypotension)
- Salt craving
- Low blood pressure
Skin/Mucosal (from excess ACTH)
- Hyperpigmentation - pathognomonic finding
- Most prominent at: elbows, knees, knuckles, nail beds, nipples, areolae, buccal mucosa (oral pigmentation), and recent scars
- "Bronze skin" appearance
Reproductive (from androgen deficiency - females only)
- Decreased pubic and axillary hair
- Decreased libido
Neuropsychiatric
- Depression, psychosis, cognitive impairment
In children
- Predominantly genetic (>80% of cases in children)
Addisonian Crisis (acute, life-threatening)
- Severe weakness, vomiting, abdominal pain
- Profound hypotension, tachycardia
- Circulatory collapse and shock
- Triggered by stress (infection, trauma, surgery)
Laboratory Diagnosis
Routine Blood Tests (screening clues)
| Test | Finding in Addison's |
|---|---|
| Serum sodium | Hyponatremia (↓) |
| Serum potassium | Hyperkalemia (↑) |
| Blood glucose | Hypoglycemia (↓) |
| Serum calcium | Hypercalcemia (↑) |
| Blood count | Eosinophilia, lymphocytosis |
| Metabolic panel | Metabolic acidosis |
Specific Hormonal Tests
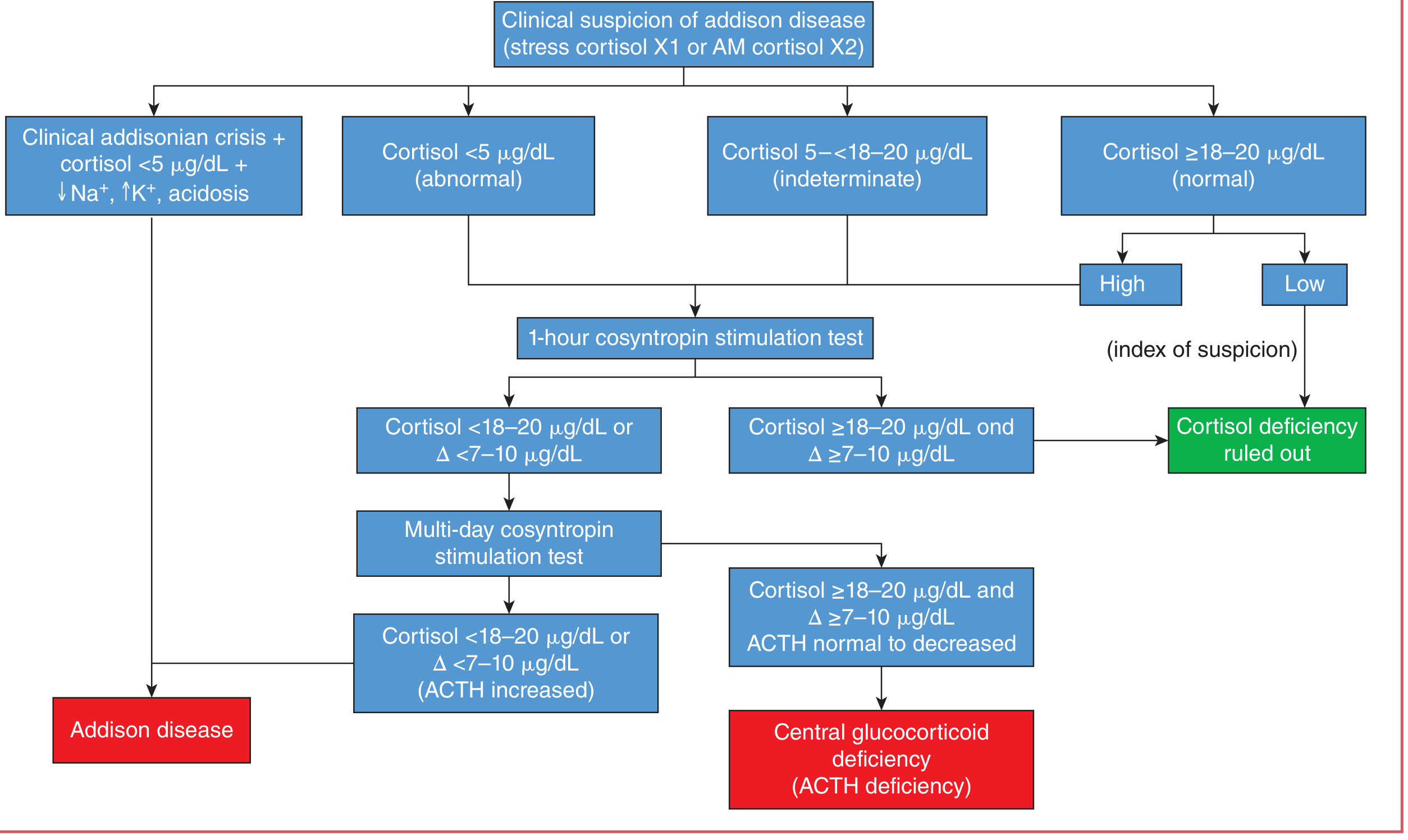
1. Morning plasma cortisol (8 AM)
- Low cortisol (<5 µg/dL) is strongly suggestive
- Normal (≥18-20 µg/dL) with high suspicion still needs stimulation testing
- Indeterminate (5-18 µg/dL) → proceed to stimulation test
2. Plasma ACTH level
- Markedly ELEVATED in primary Addison's (compensatory pituitary response)
- This distinguishes primary from secondary adrenal insufficiency (where ACTH is low/normal)
3. Cosyntropin (ACTH) Stimulation Test - Gold Standard
- 250 µg synthetic ACTH (cosyntropin) is given IV
- Cortisol measured at baseline and at 30-60 minutes
- Normal response: cortisol rises to ≥18-20 µg/dL with an increment of ≥7-10 µg/dL
- Positive (abnormal) = failure to rise appropriately → confirms adrenal insufficiency
4. Serum aldosterone and plasma renin
- Aldosterone: low/absent
- Renin: elevated (compensatory, as mineralocorticoid feedback is lost)
Autoimmune Markers
- Anti-21-hydroxylase antibodies: present in ~90% of autoimmune Addison's - highly specific marker
Imaging
- CT abdomen: bilateral adrenal atrophy (autoimmune) OR bilateral adrenal enlargement/calcification (TB/fungal)
- Chest X-ray: may show TB features
Diagnostic Algorithm
Treatment (Brief)
- Glucocorticoid replacement: Hydrocortisone 15-25 mg/day in divided doses (two-thirds morning, one-third evening)
- Mineralocorticoid replacement: Fludrocortisone 0.05-0.2 mg/day
- Addisonian crisis: IV hydrocortisone 100 mg bolus + normal saline + dextrose + treat precipitating cause
- Patients need stress dosing (2-3x their usual dose) during illness, surgery, or trauma
Key Exam Points to Remember
- Hyperpigmentation + hypotension + hyponatremia + hyperkalemia = classic triad pointing to Addison's
- Autoimmune is the #1 cause in developed countries; TB is #1 worldwide
- High ACTH = primary; Low ACTH = secondary (pituitary) insufficiency
- Gold standard test = cosyntropin stimulation test
- Anti-21-hydroxylase antibodies confirm autoimmune etiology
- Waterhouse-Friderichsen syndrome = acute Addisonian crisis from N. meningitidis sepsis with bilateral adrenal hemorrhage
Sources: Costanzo Physiology 7th Ed., p. 440; Tietz Textbook of Laboratory Medicine 7th Ed., p. 2274-2276; Current Surgical Therapy 14e
This is a shared conversation. Sign in to Orris to start your own chat.