Bladder trauma in details
Reading File
Finding Sources
Finding Sources
Searching PubMed
"bladder trauma" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive data from multiple authoritative surgical textbooks with imaging. Let me compile the full detailed response.
Bladder Trauma - Detailed Overview
Epidemiology and General Principles
Approximately 1-2% of patients with blunt abdominal trauma have associated bladder injuries. The genitourinary tract accounts for 10-15% of all abdominal and pelvic trauma. Isolated bladder injuries are uncommon - the bladder is well protected behind the pubic bone within the pelvis. Importantly:
- Pelvic fracture is associated with 83-95% of bladder injuries
- Conversely, bladder injury occurs in only 5-10% of pelvic fractures (some sources cite 10% of abdominal trauma with pelvic fracture)
- 90% of bladder ruptures are associated with pelvic fractures
- Gross hematuria is present in 75-100% of all bladder injuries - it is the cardinal sign
A high index of suspicion must be maintained in intoxicated individuals with a full bladder who sustain even mild trauma and complain of abdominal pain.
(Sabiston Textbook of Surgery, p. 751; Fischer's Mastery of Surgery, p. 7605)
Etiology / Causes
1. Non-Iatrogenic
| Mechanism | Details |
|---|---|
| Blunt trauma | Most common - motor vehicle accidents, falls, crush injuries |
| Penetrating trauma | Gunshot wounds, stab wounds |
| Pelvic fractures | Shearing forces tear bladder at fascial attachments; bone fragments can directly lacerate the bladder |
2. Iatrogenic
| Procedure | Incidence |
|---|---|
| Transurethral resection of bladder tumor (TURBT) | Most common endoscopic cause |
| Cesarean section | 0.28-0.47% |
| Abdominal hysterectomy | 0.58% |
| Laparoscopic total hysterectomy | 0.75% |
| Vaginal hysterectomy | 0.51% |
| Transvaginal tape (TVT) placement | 3-9% |
| Transobturator tape placement | 0.5% |
| Laparoscopic hernia repair | 1.6% |
| Inguinal hernia repair (open) | 0.08-0.3% |
(Campbell-Walsh-Wein Urology; Bailey & Love's Surgery 28th Ed.)
3. Spontaneous Rupture
Rare - occurs in patients with bladder augmentation who have limited bladder sensation (e.g., spinal cord injury). Results from overdistension; presents with vague abdominal pain, fever, or sepsis.
Classification
By Anatomic Location
1. Extraperitoneal Bladder Rupture (60% of cases)
- Peritoneum remains intact
- Urine extravasates into the retropubic/perivesical space
- Results in flame-shaped extravasation of contrast on cystogram
- If fascial planes are disrupted, contrast can spread to retroperitoneum, scrotum, penis, anterior abdominal wall, and thighs
- Less immediately dangerous than intraperitoneal
2. Intraperitoneal Bladder Rupture (30% of cases)
- Peritoneum over the bladder is violated
- Urine extravasates freely into the peritoneal cavity
- Typically results from blunt trauma to a full bladder, causing rupture at the dome
- Contrast outlines loops of bowel on cystogram
- Carries risk of urinary peritonitis, ileus, sepsis, azotemia, and death if not treated promptly
3. Mixed (remaining ~10%)
- Both intraperitoneal and extraperitoneal components
(Current Surgical Therapy 14e, p. 1391; Bailey & Love's Surgery 28th Ed.)
AAST Grading Scale for Bladder Trauma
| Grade | Injury Type | Description |
|---|---|---|
| I | Hematoma | Contusion, intramural hematoma |
| Laceration | Partial thickness laceration | |
| II | Laceration | Extraperitoneal bladder wall laceration <2 cm |
| III | Laceration | Extraperitoneal ≥2 cm or intraperitoneal <2 cm bladder wall laceration |
| IV | Laceration | Intraperitoneal bladder wall laceration ≥2 cm |
| V | Laceration | Laceration extending into the bladder neck or ureteral orifice (trigone) |
(Bailey & Love's Surgery 28th Ed., Table 83.18)
Clinical Features
| Feature | Description |
|---|---|
| Gross hematuria | Present in >95% - cardinal sign |
| Suprapubic pain/tenderness | Common |
| Inability or difficulty voiding | Common |
| Abdominal distension | Especially with intraperitoneal rupture |
| Clots in urine | Visible on CT |
| Scrotal ecchymosis | Suggests tracking of extravasated urine |
| Low urine output | Can occur with intraperitoneal leak |
| Peritonitis | Delayed presentation of untreated intraperitoneal rupture |
| Iatrogenic: visible during procedure | Leakage of urine/gas from bladder during TURBT or pelvic surgery |
Special populations:
- Intoxicated patients - high index of suspicion even with mild trauma
- Women: vaginal speculum examination essential - vaginal lacerations or traumatic bladder-vaginal communication can be missed with catastrophic consequences
- Bladder augmentation patients - spontaneous rupture can mimic abdominal sepsis
Imaging / Diagnosis
Gold Standard: Retrograde Cystography
Retrograde cystography (plain film or CT cystogram) is the gold standard for diagnosing bladder injury. Both have similar specificity and sensitivity.
Protocol for adequate cystography:
- Retrograde filling with a minimum of 300-400 mL of contrast or until patient tolerance
- Imaging at maximal fill
- Post-drainage views mandatory - small extravasation can be missed with a full bladder
Important: Antegrade distention by clamping a urethral catheter after standard CT with delayed imaging is NOT adequate - this does not provide sufficient distention and will miss ruptures.
Ultrasound is not effective for diagnosing bladder rupture.
CT Cystogram Findings
Extraperitoneal rupture - flame-shaped extravasation of contrast in the perivesical space:
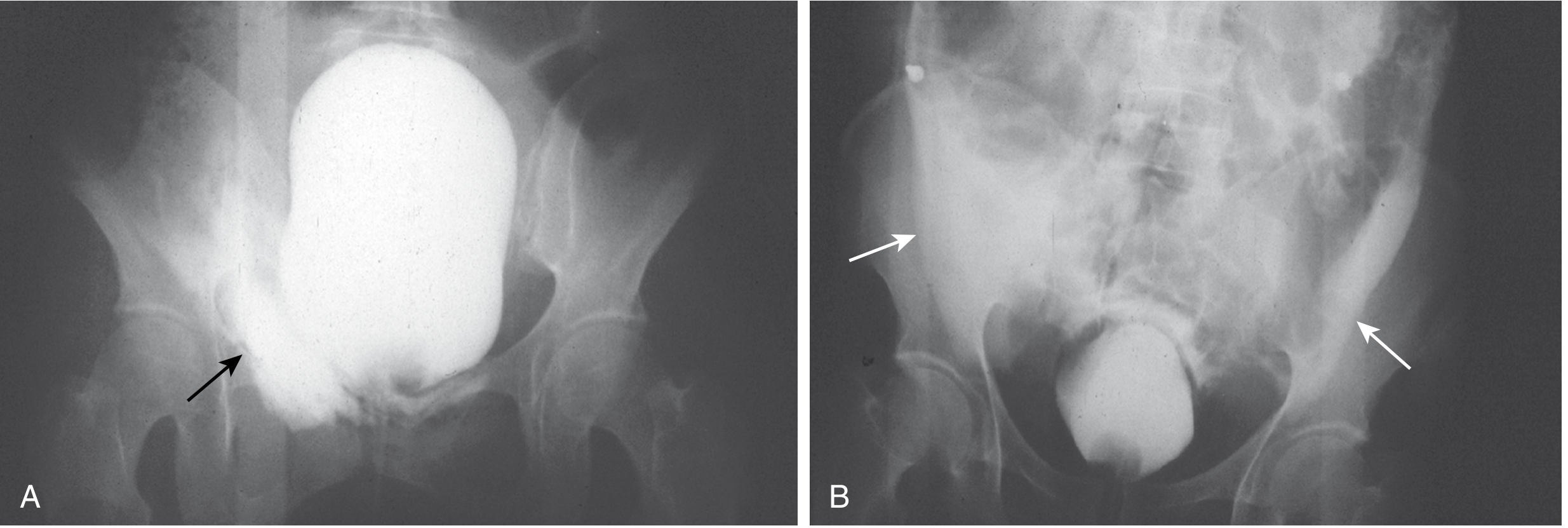
Plain film cystogram: (A) Extraperitoneal injury - localized flame-shaped extravasation (black arrow); (B) Intraperitoneal injury - contrast outlining paracolic gutters (white arrows). (Sabiston Textbook of Surgery, Fig. 39.3)
Intraperitoneal rupture - contrast tracks freely into the peritoneal cavity, outlining bowel loops:
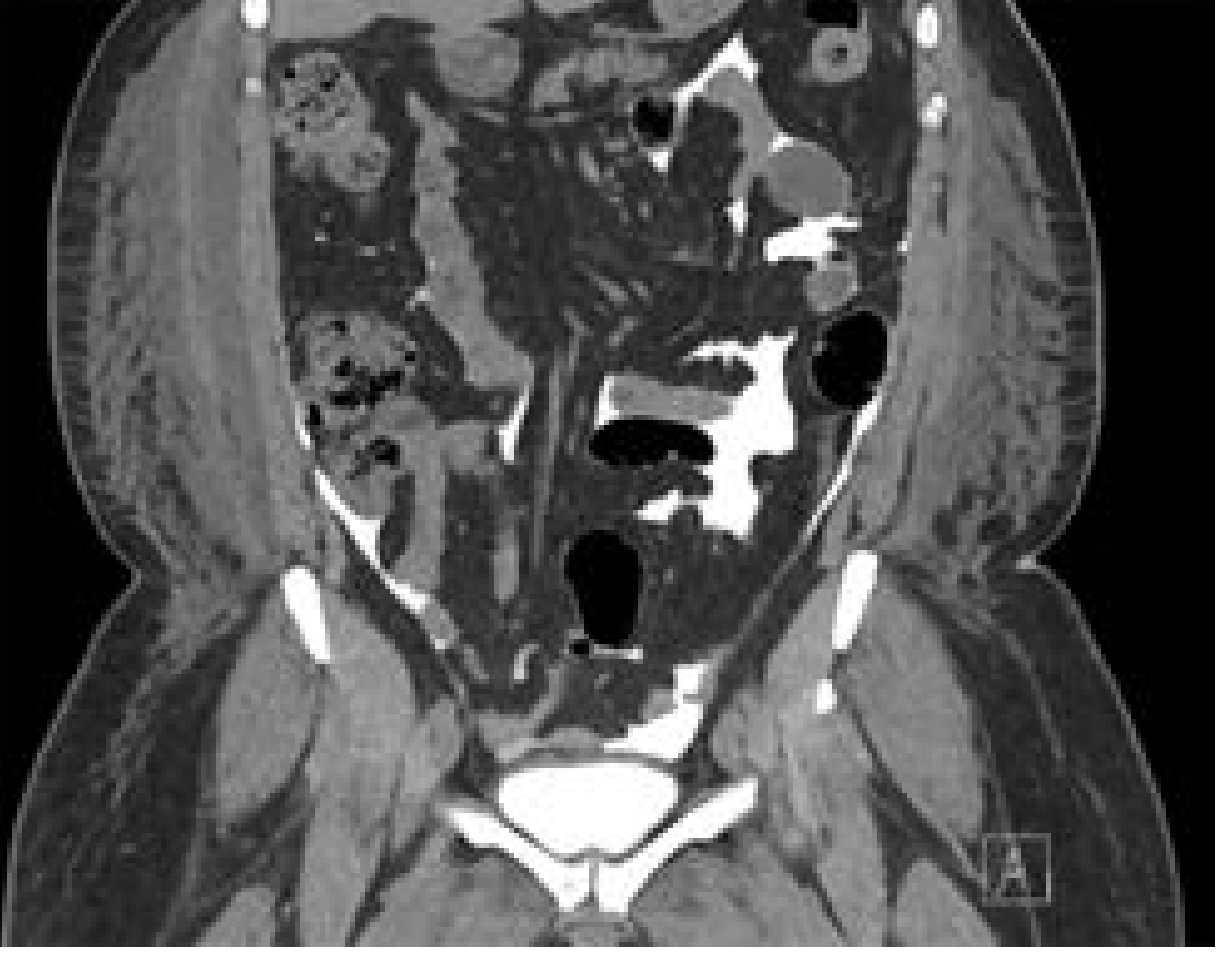
CT cystogram: Intraperitoneal rupture - contrast freely outlining bowel. (Current Surgical Therapy 14e, Fig. 1)
Extraperitoneal rupture with tracking - contrast spread to retroperitoneum, anterior abdominal wall, penis, scrotum, and thighs:
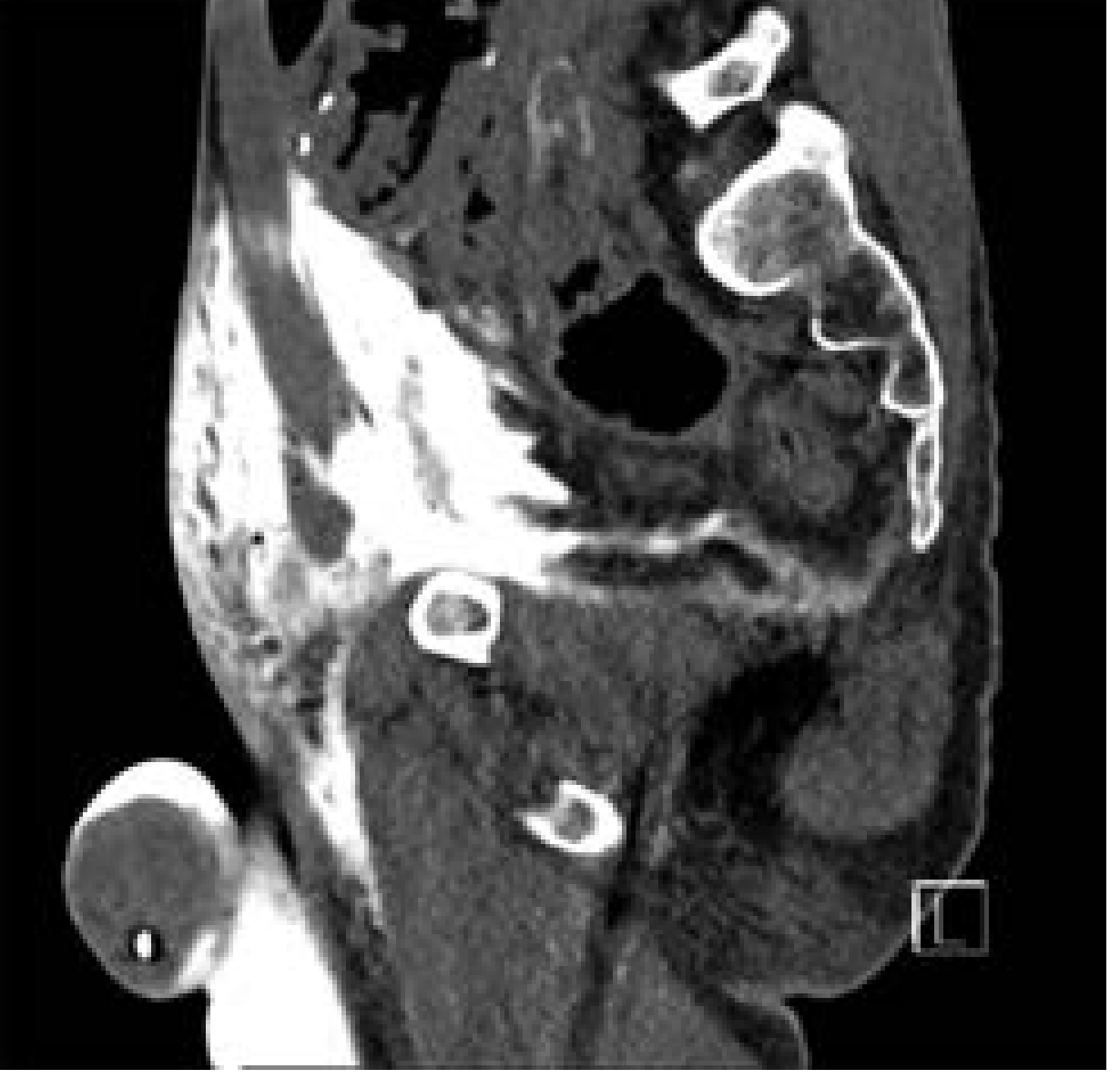
CT cystogram: Extraperitoneal rupture with contrast tracking into retroperitoneum, anterior abdominal wall, penis, scrotum, and thighs. (Current Surgical Therapy 14e, Fig. 2)
Indications for Retrograde Cystography
- Gross hematuria + pelvic fracture (~30% of these patients have bladder injury)
- Pubic symphysis diastasis + obturator ring fracture + clinical findings suggestive of bladder injury
- Suspected bladder injury by any mechanism
(Sabiston Textbook of Surgery, p. 751-752)
Management
Extraperitoneal Bladder Rupture
Conservative (Non-Operative) Management - First Line:
- Urethral catheterization with free bladder drainage for 10-14 days
- Use a large catheter (22 Fr) to ensure adequate drainage
- Antibiotics to reduce risk of infected pelvic hematoma or abscess
- Follow-up cystogram at 2 weeks to confirm healing before catheter removal
- If not healed after 4 weeks of catheter drainage, consider operative repair
Iatrogenic extraperitoneal injury recognized intraoperatively at open or laparoscopic surgery: repair at same time in two layers with 2/0 Vicryl absorbable suture.
Indications for Operative Repair of Extraperitoneal Injury
| Indication | Rationale |
|---|---|
| Concurrent bladder neck laceration | Prevent urinary incontinence |
| Concurrent rectal or vaginal laceration | Prevent fistula formation |
| Bone spicules/fragments in the bladder | Risk of perforation/non-healing |
| Significant hematuria causing clot obstruction of catheter | Catheter drainage insufficient |
| Failed conservative management after ~4 weeks | Persistent leak |
| Patient undergoing ORIF of pelvic fracture | Reduce theoretical risk of hardware infection |
| Patient undergoing abdominal exploration for other reasons | Opportunistic repair |
| Open pelvic fracture | High contamination risk |
(Sabiston Table 39.2; Current Surgical Therapy 14e; Fischer's Mastery of Surgery)
Intraperitoneal Bladder Rupture
All intraperitoneal injuries require surgical repair, regardless of mechanism. Free spillage of urine into the peritoneal cavity causes peritonitis, sepsis, azotemia, and death if untreated.
- Exception: Very small injuries without significant fluid extravasation in clinically stable patients may be attempted with catheterization and close monitoring, with cystogram at 2 weeks to confirm healing.
Surgical Technique
Approach: Lower midline incision, extending laparotomy if already performed.
Steps:
- Identify anterior bladder wall in the midline
- Extend the cystotomy to examine integrity of bladder neck and ureteral orifices
- Assess ureters - use IV indigo carmine, methylene blue, fluorescein, or retrograde ureteral catheterization
- Two-layer repair with slowly absorbable suture (e.g., 2-0 Vicryl to 4-0 Vicryl):
- Layer 1: Mucosa + muscularis
- Layer 2: Muscularis + serosa
- Achieve watertight closure
- Place closed suction drain in pelvis
- Leave Foley catheter for drainage (suprapubic tube rarely needed unless complex laceration or concurrent spinal cord injury)
- If concomitant pelvic injuries: use tissue interposition flaps to separate suture lines
For extraperitoneal injuries during open exploration:
- Can be closed intravesically using absorbable suture by entering through the anterior bladder wall
- Avoid disturbing pelvic hematoma if possible
Follow-up: Cystogram at 10-14 days to confirm healing before catheter removal.
(Sabiston Textbook of Surgery, p. 752; Current Surgical Therapy 14e)
Iatrogenic Bladder Injury - Special Considerations
Intraoperative Recognition
- If recognized at time of TURBT: stop procedure, achieve hemostasis, catheterize
- If recognized during open/laparoscopic surgery: repair immediately in two layers
Risk Factors for Iatrogenic Injury
- Operating within or near the bladder (endoscopic surgery)
- Prior surgery, radiation therapy, or tumor mass effect causing anatomic distortion
- Pelvic organ prolapse (vaginal approach)
- Fixed pelvic space limiting exposure and retractor placement
Fistula Prevention
In vaginal approach surgery with high fistula risk, interpose peritoneum, omentum, or labial fat between the anterior vaginal wall and the bladder/urethra.
(Campbell-Walsh-Wein Urology; Berek & Novak's Gynecology)
Complications
| Complication | Context |
|---|---|
| Urinary peritonitis | Untreated intraperitoneal rupture |
| Sepsis / death | Delayed diagnosis of intraperitoneal rupture |
| Azotemia | Absorption of urinary constituents from peritoneal cavity |
| Vesicovaginal fistula | Missed vaginal laceration + bladder injury |
| Rectovesical fistula | Concurrent rectal injury + bladder injury |
| Urinary incontinence | Bladder neck injury |
| Pelvic abscess | Infected pelvic hematoma |
| Hardware infection | Unrepaired bladder injury near ORIF hardware |
| Ileus | Urinary peritonitis |
| Non-healing of bladder | Inadequate drainage or missed complex injury |
Summary Algorithm
Suspected Bladder Trauma
|
↓
Hemodynamic stabilization → Rule out urethral injury first (retrograde urethrogram if concerned)
|
↓
Retrograde Cystogram (minimum 300-400 mL contrast) + post-drainage views
|
_____________
| |
Negative Positive
| |
No rupture Classify: Extraperitoneal vs Intraperitoneal
| |
Extraperitoneal Intraperitoneal
| |
Simple? ——→ Yes SURGICAL REPAIR
|
Catheter 10-14 days
+ Antibiotics
+ Cystogram at 2 wks
|
Complicated? ——→ SURGICAL REPAIR
(bladder neck, rectum, vagina, bony spicules,
clot obstruction, ORIF setting, failed conservative Rx)
Key Points Summary
- Bladder rupture is rarely isolated - always assess for associated injuries
- Pelvic fracture is present in 83-95% of bladder injuries
- Gross hematuria (>95%) is the cardinal sign; always investigate thoroughly
- Retrograde cystography with 300-400 mL contrast is the gold standard; passive/antegrade filling is unacceptable
- Extraperitoneal rupture: managed conservatively with catheter drainage (10-14 days) in uncomplicated cases
- Intraperitoneal rupture: requires surgical repair in nearly all cases
- Operative repair uses two-layer watertight closure with absorbable suture
- Vaginal speculum exam is mandatory in women - vaginal laceration with bladder injury can form devastating fistula
- Suprapubic tube is rarely needed except in complex cases or spinal cord injury
Sources: Sabiston Textbook of Surgery (Biological Basis of Modern Surgical Practice), p. 750-752 | Bailey & Love's Short Practice of Surgery 28th Ed., p. 1541-1542 | Current Surgical Therapy 14e, p. 1391-1392 | Fischer's Mastery of Surgery 8th Ed., p. 7605-7606 | Campbell-Walsh-Wein Urology | AAST Organ Injury Scale (updated 2020 AUA/EAU guidelines)
This is a shared conversation. Sign in to Orris to start your own chat.