I love you
I appreciate the kind words! I'm here and ready to help you with anything you need - questions, research, writing, analysis, or just a good conversation. What's on your mind today?
Uterus
Reading File
Asking for Preferences
Uterus parts content ligament clinical
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of the uterus covering its parts, wall layers, ligaments, and clinical correlates.
The Uterus
1. Position and Relations
The uterus is a thick-walled, intraperitoneal muscular organ in the midline of the pelvis, sitting posterior to the bladder and anterior to the rectum. The nonpregnant uterus weighs 40-80 g. - Gray's Anatomy for Students
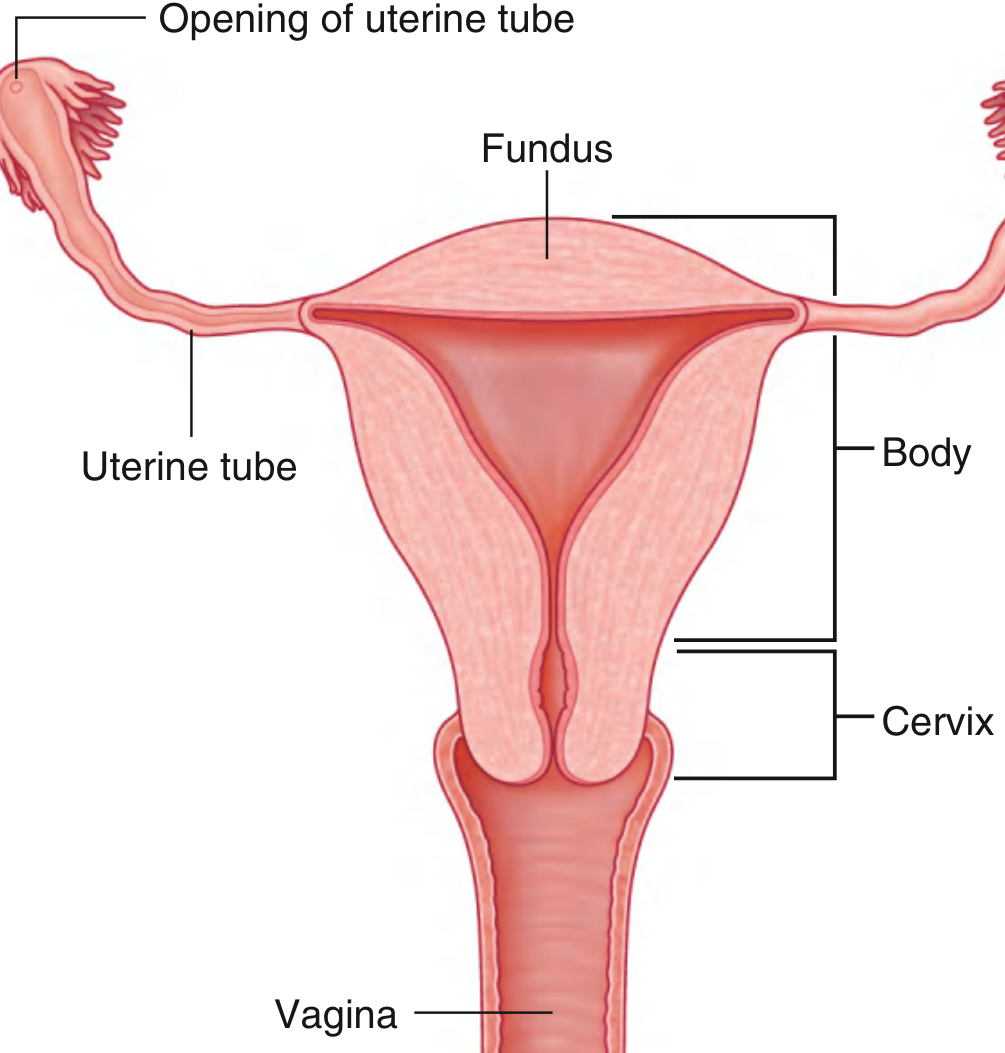
2. Parts of the Uterus
| Part | Description |
|---|---|
| Fundus | The rounded superior end above the level of uterine tube openings |
| Body (Corpus) | The main flattened part; contains the uterine cavity |
| Isthmus | Narrow junction between body and cervix |
| Cervix | The lower cylindrical part that projects into the vagina |
- The uterine cavity is a narrow slit when viewed laterally, and an inverted triangle when viewed anteriorly.
- Each superior corner of the cavity (the cornua) opens into a uterine tube; the inferior corner leads into the cervical canal.
- Implantation of the blastocyst normally occurs in the body. - Gray's Anatomy for Students
3. Wall Layers (3 Layers)
A. Perimetrium (Serosa)
- Outermost layer; a thin peritoneal covering continuous with the broad ligaments and pelvic peritoneum.
B. Myometrium
- The thickest layer; composed of smooth muscle arranged in three distinct sublayers:
- Inner (subvascular) layer - thin
- Middle layer - thickest; rich vascular supply (sponge-like); muscle cells form a 3D meshwork. This is the main layer responsible for expelling the fetus during birth.
- Outer (supravascular) layer - thin
Clinical note: During pregnancy, smooth muscle cells enlarge, allowing the uterus to grow 7-10x its original size. Benign tumors of myometrium are called leiomyomas (fibroids). - Color Atlas of Human Anatomy
C. Endometrium (Mucosa)
- The innermost layer lining the uterine cavity.
- Cell-rich connective tissue with simple columnar epithelium.
- Contains uterine glands (tubular invaginations).
- Divided into two layers:
- Basalis (Basal layer) - not shed during menstruation; regenerates the endometrium each cycle.
- Functionalis (Functional layer) - undergoes cyclic changes; shed during menstruation.
Menstrual cycle phases of the endometrium:
- Proliferative phase (Days 5-14): Functional layer restored under estradiol influence; glands enlarge.
- Secretory phase (Days 15-28): Glands continue growing under progesterone + estrogen; produce viscous secretion; blood vessels multiply. Spongy layer (II) and compact layer (III) become distinct.
- Ischemic/Desquamation phase (Days 1-4): Hormone withdrawal causes tissue degeneration and shedding (menstruation). - Color Atlas of Human Anatomy
Clinical note: Curettage removes only the functional layer, leaving the basal layer intact. When endometrial tissue migrates outside the uterine cavity to the ovary or pelvic peritoneum, the result is endometriosis. - Color Atlas of Human Anatomy
4. Cervix - Special Features
- The cervical mucosa does NOT undergo cyclic shedding.
- Has branching tubular cervical glands that produce alkaline mucus.
- Ectocervix (vaginal portion): covered by stratified non-keratinized squamous epithelium.
- Endocervical canal: lined by columnar epithelium.
- The junction between the two is the Squamo-columnar junction (transformation zone).
Clinical note: The transformation zone is the most common site of cervical carcinoma. It is visible on colposcopy in women of childbearing age, but migrates into the cervical canal with increasing age. - Color Atlas of Human Anatomy
5. Ligaments of the Uterus
| Ligament | Attachment | Function/Contents |
|---|---|---|
| Broad ligament | Extends laterally off the uterine corpus to the pelvic peritoneum | Envelops the uterus, fallopian tube, round ligament, and ovarian ligament; separates pelvis into anterior and posterior compartments |
| Round ligament | Uterine cornua → laterally through broad ligament → inguinal ring → labia majora | Maintains anteversion of the uterus |
| Cardinal ligament (Mackenrodt's ligament) | Cervix → lateral pelvic wall (pelvic diaphragm), fuses medially with vagina | Supports the uterus at the level of the cervix; the uterine arteries travel within it |
| Uterosacral ligament | Upper posterior cervix → 3rd sacral vertebra | Forms an arch framing the rectum; important for apical support |
Note: Of all these, anatomically only the round ligament and broad ligament are clearly defined structures. The uterus is mainly supported by the pelvic floor muscles, not the ligaments. - Color Atlas of Human Anatomy, Sabiston Textbook of Surgery
6. Blood Supply
- Uterine arteries - branches of the internal iliac arteries; travel within the cardinal ligament then superiorly along the lateral uterine body.
- Ovarian arteries - arise directly from the abdominal aorta; travel to the uterus adjacent to the ovary.
Clinical note: During hysterectomy, the distal ureters must be carefully identified because the uterine arteries pass very close to them (the ureter is at risk of ligation). - Gray's Anatomy for Students
7. Nerve Supply
| Type | Pathway |
|---|---|
| Sympathetic | Hypogastric and ovarian plexus |
| Parasympathetic | Lumbosacral plexus (S2-S4) |
| Afferent (pain) | Travel with sympathetic fibers via lumbosacral plexus (T11-T12) |
8. Clinical Correlates Summary
| Condition | Key Point |
|---|---|
| Fibroids (Leiomyomas) | Benign smooth muscle tumors of the myometrium |
| Endometriosis | Endometrial tissue outside the uterus (ovary, peritoneum) |
| Cervical carcinoma | Arises at the squamo-columnar transformation zone |
| Uterine prolapse | Failure of cardinal-uterosacral complex support |
| Hysterectomy | Surgical removal of uterus; care needed to protect ureters near the uterine artery |
| Curettage (D&C) | Removes functional layer only; basal layer remains and regenerates |
Sources: Gray's Anatomy for Students; Sabiston Textbook of Surgery; Color Atlas of Human Anatomy Vol. 2; SCHWARTZ'S Principles of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.