Etiopathogenesis of the chronic complication of diabetes mellitus.
Reading File
Finding Sources
Finding Sources
Searching PubMed
"diabetes mellitus" AND "chronic complications" AND pathogenesis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive material from authoritative textbooks. Let me compile the full answer.
Etiopathogenesis of Chronic Complications of Diabetes Mellitus
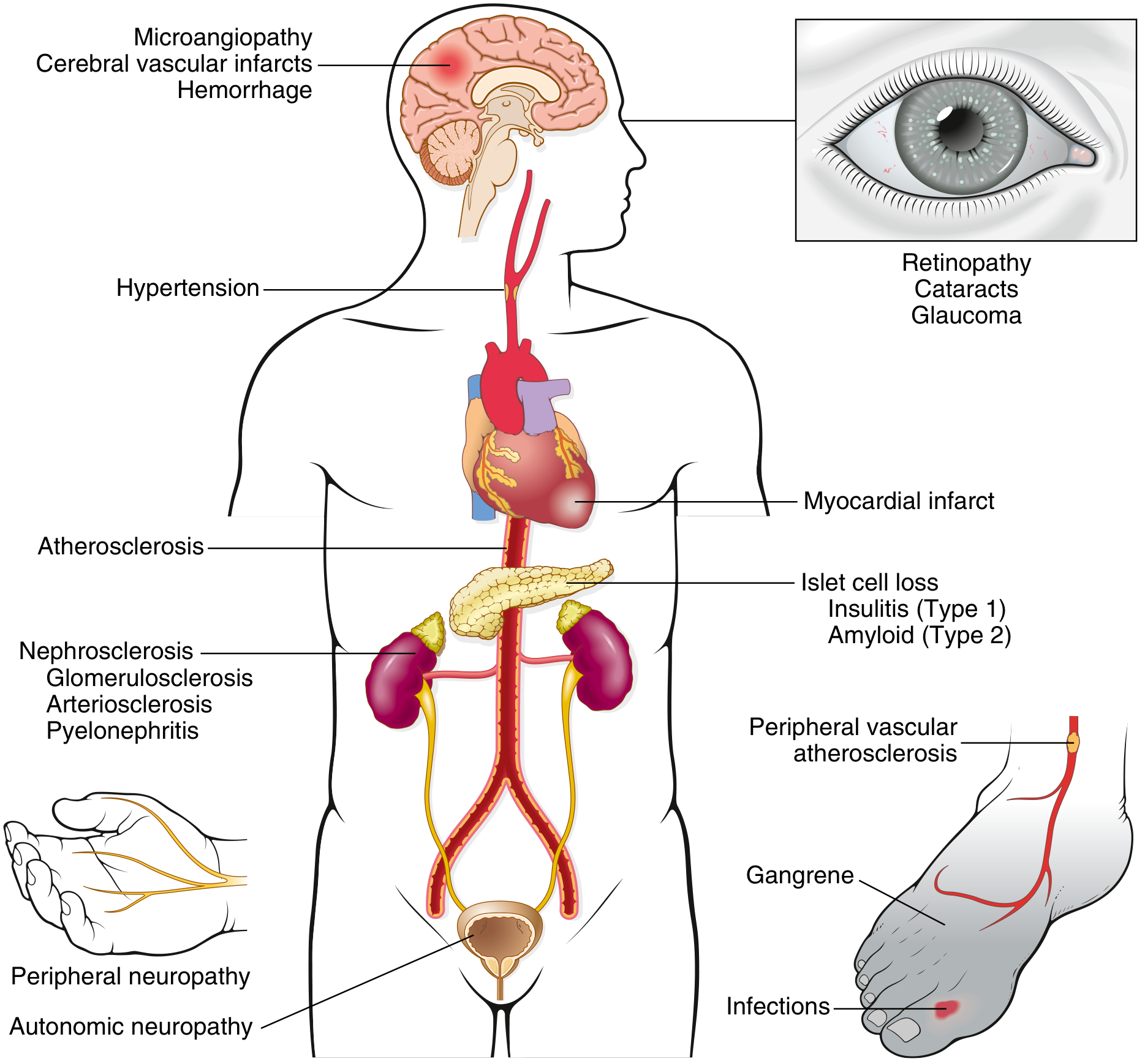
Fig. Long-term complications of diabetes - Robbins & Kumar Basic Pathology
Overview
The morbidity associated with long-standing diabetes (both Type 1 and Type 2) results from damage to large- and medium-sized muscular arteries (macrovascular disease) and small vessels (microvascular disease). The effects of microvascular disease are most profound in the retina, kidneys, and peripheral nerves, producing the classic triad of retinopathy, nephropathy, and neuropathy. Macrovascular disease causes accelerated atherosclerosis, leading to increased risk of myocardial infarction, stroke, and lower-extremity ischemia.
Central Etiology: Glucotoxicity (Persistent Hyperglycemia)
Persistent hyperglycemia is the primary driver of all chronic complications. Evidence from major randomized trials (DCCT, UKPDS) shows that tight glycemic control (HbA1c <7%) delays or prevents the onset of complications. HbA1c, formed by nonenzymatic covalent addition of glucose to hemoglobin, measures glycemic control over ~120 days and is the standard surrogate marker. Continuous glucose monitoring has added a new goal - "time-in-range" - which may be a better predictor of complication risk.
Importantly, hyperglycemia is not the only factor. Insulin resistance, obesity, hypertension, dyslipidemia, smoking, and genetic susceptibility all contribute.
Four Core Mechanisms of Hyperglycemic Tissue Damage
1. Advanced Glycation End Products (AGEs)
AGEs form from nonenzymatic reactions between intracellular glucose-derived precursors (glyoxal, methylglyoxal, 3-deoxyglucosone) and the amino groups of intracellular and extracellular proteins. The rate of AGE formation is accelerated by hyperglycemia.
- AGEs bind to a specific receptor called RAGE (receptor for AGEs), expressed on inflammatory cells (macrophages, T cells), endothelium, and vascular smooth muscle.
- Endothelium-specific overexpression of RAGE in diabetic mice accelerates large vessel injury and microangiopathy; RAGE-null mice show attenuation of these features.
- AGEs also directly cross-link extracellular matrix proteins (collagen, elastin), leading to vascular stiffness and basement membrane thickening; LDL gets trapped in AGE-modified large vessel walls (accelerating atherosclerosis), and albumin is trapped in capillary walls (contributing to microangiopathy).
Effects of AGE-RAGE signaling:
- Release of TGF-β - deposition of excess basement membrane material
- Release of VEGF - neovascularization in diabetic retinopathy
- Generation of reactive oxygen species (ROS) in endothelial cells
- Increased procoagulant activity on endothelial cells and macrophages
- Enhanced proliferation of vascular smooth muscle cells and extracellular matrix synthesis
2. Activation of Protein Kinase C (PKC)
Intracellular hyperglycemia stimulates de novo synthesis of diacylglycerol (DAG) from glycolytic intermediates, which in turn causes excessive activation of protein kinase C (PKC).
Downstream effects of PKC activation include:
- Production of VEGF (neovascularization in retinopathy)
- Production of TGF-β (fibrogenesis, increased extracellular matrix)
- Production of PAI-1 (plasminogen activator inhibitor-1) - procoagulant state
- Enhanced angiogenesis, vasoconstriction, vascular permeability, cytokine activation
Note: the effects of AGEs and activated PKC overlap, and both contribute to diabetic microangiopathy.
3. Oxidative Stress and Polyol Pathway Disturbances
In tissues that do not require insulin for glucose transport (nerves, lens, kidneys, blood vessels), persistent hyperglycemia leads to increased intracellular glucose, which is metabolized by aldose reductase to sorbitol (a polyol) and then to fructose.
- This reaction consumes NADPH as a cofactor.
- NADPH is also required by glutathione reductase to regenerate reduced glutathione (GSH), a key cellular antioxidant.
- Sustained hyperglycemia depletes intracellular NADPH, compromises GSH regeneration, and increases cellular susceptibility to oxidative stress.
- Sorbitol accumulation in the lens contributes to cataract formation.
4. Hexosamine Pathway Activation
Hyperglycemia drives glycolytic intermediates into the hexosamine pathway, generating glucosamine-6-phosphate and ultimately causing post-translational modification of cytoplasmic and nuclear proteins. This is associated with:
- Upregulation of TGF-α and TGF-β1
- Upregulation of PAI-1
- Dysregulation of endothelial nitric oxide synthase (eNOS)
- Resulting in insulin resistance and vascular complications
Morphology of Chronic Complications
Pancreas
- T1D: Reduction in number/size of islets; insulitis (leukocytic - predominantly T lymphocyte - infiltration of islets)
- T2D: Subtle islet mass reduction; amyloid deposition (islet amyloid polypeptide/amylin) within islets, beginning around capillaries and eventually obliterating islets; fibrosis may also be present
- Nondiabetic newborns of diabetic mothers: islet hyperplasia in response to maternal hyperglycemia
Diabetic Macrovascular Disease
- Accelerated atherosclerosis involving the aorta and large/medium-sized arteries (morphologically indistinguishable from non-diabetic atherosclerosis)
- Myocardial infarction - most common cause of death in diabetes (2-4x higher coronary risk)
- Gangrene of lower extremities - ~100x more common than in the general population
- Cerebrovascular accidents
- Hypertension (present in ~75% of T2D) and diabetic dyslipidemia potentiate cardiovascular risk
Diabetic Microangiopathy
The hallmark morphologic feature is diffuse basement membrane thickening, most evident in capillaries of the:
- Skin, skeletal muscle, retina, renal glomeruli, renal medulla
- Also in nonvascular structures: renal tubules, Bowman capsule, peripheral nerves, placenta
Despite thickened basement membranes, capillaries remain leakier than normal to plasma proteins - this paradox underlies much of the end-organ damage.
Specific Organ Complications
Diabetic Nephropathy
- Leading cause of end-stage renal disease (ESRD); second only to MI as cause of death in diabetes
- Affects ~30-40% of all diabetic patients
- Earliest manifestation: microalbuminuria (30-300 mg/day); progresses to macroalbuminuria (>300 mg/day) with hypertension
- Three major lesions:
- Glomerular lesions: capillary basement membrane (GBM) thickening, diffuse mesangial sclerosis (most common), nodular glomerulosclerosis (Kimmelstiel-Wilson nodules) - pathognomonic but not the most common lesion
- Renal vascular lesions: arteriolosclerosis of both afferent and efferent arterioles (efferent arteriolar hyalinosis is virtually pathognomonic of diabetes)
- Pyelonephritis: including necrotizing papillitis (renal papillary necrosis)
- Ethnic susceptibility: Native Americans, Hispanics, and African Americans have higher risk of ESRD
Diabetic Retinopathy
- Eventually affects >50-80% of patients with long-standing diabetes; leading cause of adult blindness in the United States
- Pathogenesis: Loss of retinal pericytes (supporting cells), basement membrane thickening, altered retinal blood flow; damaged capillaries leak protein, RBCs, and lipids causing retinal edema; chronic hypoxia from capillary occlusion promotes VEGF-driven neovascularization (new abnormal vessels prone to rupture)
- Classification:
- Nonproliferative (background) retinopathy (NPDR): microaneurysms, intraretinal hemorrhages (blot/flame), hard exudates (lipid deposits), cotton-wool spots (soft exudates from ischemia), venous beading, IRMA (intraretinal microvascular abnormalities)
- Proliferative diabetic retinopathy (PDR): neovascularization, pre-retinal/vitreous hemorrhage, traction retinal detachment, potential blindness
- Diabetic macular edema: can occur at any stage; retinal thickening/hard exudates involving the macula
Diabetic Neuropathy
- Clinical peripheral neuropathy affects ~50% of all diabetic patients, and up to 80% of those with disease >15 years
- Three compartments are affected:
- Peripheral sensorimotor neuropathy: "stocking-glove" sensory loss, pain, paresthesias; predisposes to Charcot joint (neuropathic arthropathy) and diabetic foot ulcers
- Autonomic neuropathy: postural hypotension, gastroparesis, impotence, bladder dysfunction, diarrhea/constipation
- Mononeuropathy (cranial or peripheral): acute onset, e.g., CN III or CN VI palsy causing diplopia
Infections (Increased Susceptibility)
Diabetics are prone to bacterial and fungal infections due to:
- Impaired neutrophil function (chemotaxis, phagocytosis, killing)
- Poor tissue perfusion
- Hyperglycemic environment favoring microbial growth
Common infections include cutaneous/soft tissue infections, mucormycosis (rhinocerebral), emphysematous cholecystitis, malignant otitis externa (Pseudomonas), and necrotizing fasciitis.
Summary: Pathogenesis in a Unifying Framework
Persistent Hyperglycemia (Glucotoxicity)
|
┌─────┴────────────────────────────┐
│ │
AGE Formation PKC Activation (via DAG)
+ RAGE signaling Polyol pathway (sorbitol/NADPH depletion)
+ Cross-linking Hexosamine pathway activation
│ │
└──────────── Oxidative Stress ────┘
|
┌──────────────┼──────────────┐
│ │ │
Endothelial Basement Vascular
Dysfunction Membrane Smooth Muscle
(leaky vessels) Thickening Proliferation
│ │ │
┌────┴───────────────┴──────────────┴────┐
│ END-ORGAN DAMAGE │
├─ Macrovascular: Atherosclerosis │
│ (MI, stroke, peripheral vascular) │
├─ Microangiopathy: Nephropathy │
│ Retinopathy, Neuropathy │
└─────────────────────────────────────────┘
Sources:
- Robbins & Kumar Basic Pathology, p. 749-750
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1023-1026
- Goldman-Cecil Medicine, Chapter 210
This is a shared conversation. Sign in to Orris to start your own chat.