Rigid oesophagoscopy
Reading File
Rigid oesophagoscopy anaesthesia postion and instruments used with images explain in detail
Reading File
Finding Sources
Finding Sources
Searching the Web
rigid oesophagoscopy anaesthesia position instruments used ENT surgery
Reading File
Reading Web Page
https://www.entlecture.com/rigid-oesophagoscopy
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading Web Page
https://www.vumc.org/global-surgical-atlas/sites/default/fil…
Searching the Web
Negus oesophagoscope Chevalier Jackson oesophagoscope instruments images rigid
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive material. Let me compile the full detailed answer.
Rigid Oesophagoscopy - Anaesthesia, Position & Instruments
Definition
Rigid oesophagoscopy is the direct endoscopic examination of the oesophagus using a straight, hollow metal tube (the rigid oesophagoscope) passed through the mouth. It provides superior control for foreign body removal, biopsy, and dilation compared to flexible endoscopy, particularly for the hypopharynx and upper oesophagus. - Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Indications
Diagnostic:
- Dysphagia evaluation (food sticking)
- Biopsy and staging of upper aerodigestive tract (UADT) tumours
- Visualisation of postcricoid area (poorly seen on flexible endoscopy)
- Panendoscopy - to exclude synchronous primaries in squamous cell carcinoma
- Assessment of pharyngeal pouches (Zenker's diverticulum)
Therapeutic:
- Foreign body removal (the gold standard for impacted hard/sharp objects)
- Dilation of complex oesophageal strictures
- Treatment of pharyngeal pouches
Anaesthesia
Rigid oesophagoscopy is performed under general anaesthesia (GA) with endotracheal intubation. This is a shared airway procedure - close communication and cooperation between surgeon and anaesthetist is mandatory.
Key anaesthetic points:
- Induction: Intravenous (e.g., propofol) or inhalational (sevoflurane) induction depending on airway difficulty
- Airway: Oral endotracheal intubation in most cases; the surgeon must be present at induction in case of airway difficulty
- Muscle relaxation: Short to medium-acting agents preferred - inform anaesthetist of expected procedure duration
- The endotracheal tube must be kept in view during scope insertion to avoid displacement
- A tracheostomy set must be ready for difficult airways; the surgeon should be scrubbed before GA induction
In the UK, use of the rigid endoscope to examine the lower one-third of the oesophagus is discouraged due to higher risk of complications (perforation). - Scott-Brown's
Patient Position
The correct position is critical - the goal is to align three axes (oral, pharyngeal, oesophageal) into a single straight line.
"Boyce-Jackson Position" (Modified Sword-Swallowing / Sniffing-Barking Dog Position)
This is the classic position used:

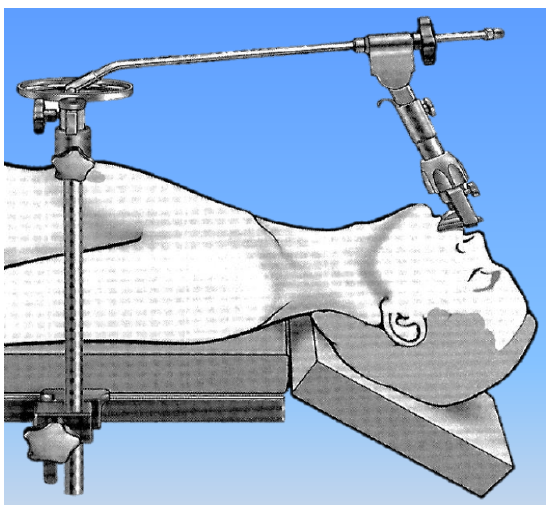
Steps to achieve the position:
- Patient is placed supine on the operating table
- A shoulder roll (sandbag or folded blanket under the shoulders) elevates the shoulders - this causes the cervical spine to extend
- The head rests in a head ring (doughnut ring) to support it - the head ring must be high enough so the head is supported by the ring, NOT by the vertebral column. If pushing gently on the forehead causes the head to move down, the cervical spine is being hyperextended - raise the head ring
- The head is elevated and the neck is extended - this brings the cervical spine into a straight line with the thoracic spine
- The operating table is rotated 90 degrees away from the anaesthetic machine to give the surgeon manoeuvrability at the head end
- The surgeon sits at the head of the table (at a comfortable height)
Why this position?
- The proximal oesophagus follows the lordosis of the cervical and thoracic spine
- Neck extension straightens this curve and creates a near-straight axis from mouth to upper oesophagus
- This converts the normal oropharyngeal-oesophageal angle into one straight line - enabling passage of a rigid tube
Important: Pre-operatively assess neck range of motion while the patient is awake. Prominent cervical osteophytes (cervical spondylosis) can impair scope advancement and increase the risk of mucosal trauma.
Instruments Used
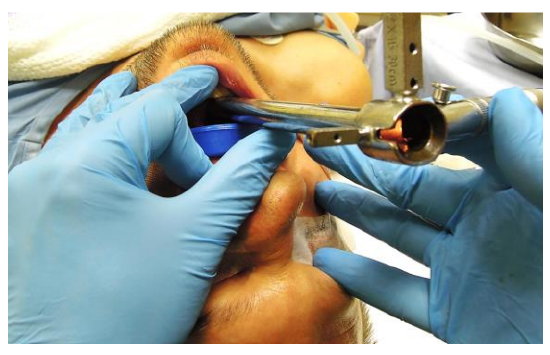
1. The Rigid Oesophagoscope (Main Scope)
The centrepiece of the procedure. Multiple types exist:
Features of a rigid oesophagoscope:
- A long, straight, hollow metal tube (longer than a laryngoscope)
- Oval or round cross-section lumen - usually oval to accommodate the oesophageal shape
- Has a proximal handle and a distal open bevel/tip
- The beveled tip faces posteriorly on insertion - this guides the scope into the upper oesophageal sphincter (cricopharynx)
- Standard adult scope: ~50 cm length, lumen ~10-12 mm
- A light carrier (fibreoptic) is inserted into a slot inside the scope
Named oesophagoscopes:
- Negus oesophagoscope - the most commonly used in the UK; oval lumen; has a handle and a proximal eyepiece; provides good illumination and working channel
- Chevalier Jackson oesophagoscope - the original design by the pioneer of endoscopy; rectangular/oval lumen; no side vents (distinguishes it from the bronchoscope which has side vents); used at the head of the table ("high-low" technique)
- Tucker oesophagoscope - modified Jackson type, beveled anterior lip
2. Light Source and Fibreoptic Cable
- A xenon or LED light source provides illumination
- Connected to the scope via a fibreoptic light cable
- The light carrier (fibreoptic light guide) clips into a slot on the inside of the scope or attaches externally
- Some scopes use a rod-lens telescope inserted through the lumen for magnified visualisation on a camera monitor
3. Suction Tube (Jackson Suction Cannula)

- A long, thin, metal rigid suction tube passed down the lumen of the oesophagoscope
- Clears secretions, blood, and pooled material from the field
- Critical for maintaining clear vision throughout the procedure
4. Biopsy Forceps

- Long, angled forceps passed through the lumen of the scope
- Cup/cupped biopsy forceps - for tissue sampling of mucosal lesions
- Alligator (crocodile) forceps - strong jaw grip for foreign body retrieval
- Rat-tooth forceps - for firm/harder foreign bodies (coins, bones)
- Grasping forceps - general retrieval
5. Foreign Body Forceps (Variety)

Different shapes for different foreign bodies:
- Coin forceps - flat, wide jaws
- Safety pin closer - specially designed to close open safety pins before withdrawal
- Laryngeal punch forceps
- Magnetic retrievers - for metallic objects
6. Proximal End Components
- Eyepiece/proximal cap - closes the proximal end to allow suction/pressure during ventilation if needed; opened for working
- Side arm - for oxygen insufflation or attachment to anaesthetic circuit (apnoeic oxygenation or jet ventilation in some protocols)
- Telescope (Hopkins rod-lens, 0° forward-viewing) - inserted through the scope to project a magnified image onto a monitor via a camera head; allows the entire team to see
7. Tooth Guard / Dental Guard
- A rubber or silicone guard placed over the upper incisors before scope insertion
- Protects teeth from being chipped or fractured as the scope is levered in
- Cotton rolls used as a substitute if the patient is edentulous
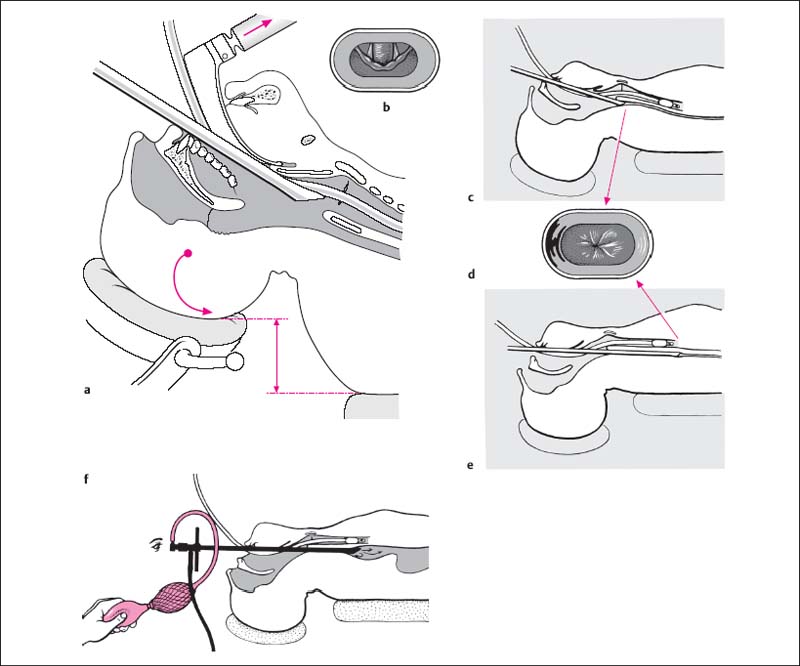
Technique Summary (Step-by-Step)
- Pre-op assessment - assess neck mobility and dentition
- GA + intubation - short/medium acting agents; surgeon present at induction
- Position - supine, shoulder roll, head ring; neck extended; table rotated 90° from anaesthetic machine
- Tooth guard applied
- Scope insertion - bevel facing posteriorly, inserted through the right side of the mouth, protecting lips with fingers of non-dominant hand
- Sequential identification - base of tongue → vallecula → epiglottis → arytenoids → posterior pharyngeal wall → keep endotracheal tube in view
- Passing the cricopharynx - this is the first and tightest natural narrowing (at C6); the beveled tip is angled posteriorly and gently advanced with a caudal-posterior direction; never force
- Three natural narrowings must be navigated:
- Cricopharyngeus (upper oesophageal sphincter, C6) - most common site of FB impaction and perforation
- Aortic arch crossing (~22-25 cm from incisors)
- Diaphragmatic hiatus (~40 cm)
- Inspect pyriform sinuses by directing scope left and right - frequent site of FB lodgement
- Biopsy / intervention performed under direct vision
- Final inspection on withdrawal - check for bleeding, perforation, mucosal tears
- Extubation only after patient is breathing freely; surgeon remains present
Key Anatomical Distances from Upper Incisors
| Landmark | Distance |
|---|---|
| Upper oesophageal sphincter (cricopharynx) | ~15 cm |
| Aortic arch impression | ~22-25 cm |
| Carina | ~25 cm |
| Lower oesophageal sphincter (hiatus) | ~40 cm |
Complications
- Oesophageal perforation - most common at Killian's triangle (Killian's dehiscence, between thyropharyngeus and cricopharyngeus - the weakest point of the posterior pharyngeal wall); also at aortic arch level
- Dental injury (chipped incisors)
- Mucosal lacerations / haematoma
- Aspiration
- Mediastinitis (if perforation missed)
- Recurrent laryngeal nerve injury
- Oesophageal stricture (late, post-dilatation)
Rigid vs Flexible Oesophagoscopy - Quick Comparison
| Feature | Rigid | Flexible |
|---|---|---|
| Anaesthesia | GA required | Topical + IV sedation |
| Postcricoid / hypopharynx view | Excellent | Poor |
| Foreign body removal | Superior (control) | Limited |
| Full oesophageal length | Limited | Full |
| Risk | Higher (perforation) | Lower |
| Setting | OT | Endoscopy suite |
References:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8th edition - Direct pharyngo-oesophagoscopy section
- Fagan J, De Groot M. Rigid Laryngoscopy, Oesophagoscopy and Bronchoscopy in Adults - Open Access Atlas of Otolaryngology, UCT
- Davis R. Rigid Upper Esophagoscopy - VUMC Global Surgical Atlas
This is a shared conversation. Sign in to Orris to start your own chat.