Why GFR dec in neohritic syndrome and what is azotemia
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is the full answer:
Why GFR Decreases in Nephritic Syndrome
The core mechanism is glomerular inflammation. Here is how it plays out step by step:
1. Inflammatory cell infiltration and glomerular hypercellularity
In nephritic syndrome, immune-mediated injury (e.g., immune complex deposition in post-streptococcal GN, ANCA-mediated injury, etc.) triggers an inflammatory cascade. Neutrophils and monocytes infiltrate the glomerulus, and endothelial and mesangial cells proliferate. This dramatically increases the cellularity of the glomerular tufts.
2. Damage to the glomerular capillary wall
The inflamed, hypercellular glomerulus physically narrows and compresses the capillary lumens. Capillary wall necrosis can also occur. This reduces the surface area available for filtration and impairs blood flow through the glomerular tuft.
3. Reduced glomerular capillary perfusion pressure
The glomerular inflammation reduces intraglomerular hydrostatic pressure, which is the main driving force for ultrafiltration. Less pressure = less filtration.
4. Net result: Decreased GFR
The combination of:
- Reduced filtration surface area (capillary compression)
- Damaged filtration barrier
- Reduced intraglomerular blood flow
...leads to a fall in GFR, clinically presenting as oliguria (reduced urine output) and azotemia.
"Glomerular diseases that present with the nephritic syndrome are usually associated with significant inflammation in the glomeruli, which damages capillary walls, leading to leakage of red cells (hematuria), and decreased GFR, which results in oliguria and azotemia."
- Robbins & Kumar Basic Pathology, p. 2297
The consequences of reduced GFR are also fluid and sodium retention, which activates the renin-angiotensin-aldosterone system (RAAS), causing hypertension - another classic feature of nephritic syndrome.
What is Azotemia?
Azotemia (from Latin azo = nitrogen, emia = in the blood) is a biochemical abnormality defined as:
Elevation of blood urea nitrogen (BUN) and serum creatinine levels, due largely to a decreased GFR.
- Robbins, Cotran & Kumar - Pathologic Basis of Disease, p. 2688
It reflects the kidney's failure to excrete nitrogenous waste products of protein metabolism (primarily urea and creatinine).
Types of Azotemia
| Type | Cause |
|---|---|
| Prerenal | Hypoperfusion of kidneys (hypotension, shock, dehydration, heart failure) - no parenchymal damage |
| Renal (intrinsic) | Direct glomerular, tubular, interstitial, or vascular damage |
| Postrenal | Obstruction of urine outflow distal to the kidney; corrects when obstruction is relieved |
Azotemia vs. Uremia - Key Distinction
| Term | Definition |
|---|---|
| Azotemia | Purely a lab finding - elevated BUN and creatinine |
| Uremia | Azotemia that is severe enough to cause clinical symptoms |
When azotemia progresses to uremia, patients develop:
- GI involvement: uremic gastroenteritis, nausea, vomiting
- Neurological: peripheral neuropathy, encephalopathy
- Cardiac: uremic fibrinous pericarditis
In Nephritic Syndrome Specifically
In nephritic syndrome, azotemia is a direct consequence of the reduced GFR caused by glomerular inflammation. The kidney can no longer filter BUN and creatinine adequately, so they accumulate in the blood. This is why azotemia is listed as one of the cardinal features of nephritic syndrome alongside hematuria, proteinuria (subnephrotic range), oliguria, and hypertension.
So why azotemia and proteinuria occurs
Finding Sources
Finding Sources
Reading File
Reading File
I now have excellent material from the textbooks. Here is the full explanation:
Why Azotemia and Proteinuria Occur in Nephritic Syndrome
Both arise from the same root cause - glomerular inflammation damaging the filtration barrier - but through two different mechanisms.
1. Azotemia - Why it Occurs
Normal state:
The kidney continuously filters nitrogenous waste products - primarily urea (BUN) and creatinine - out of the blood via the glomerulus. These are small molecules that pass freely through the filtration barrier and are excreted in urine.
In nephritic syndrome:
- Glomerular inflammation causes endothelial and mesangial cell proliferation + neutrophil infiltration, massively increasing cellularity inside the glomerular tuft
- This compresses and occludes the glomerular capillary lumens
- GFR falls - less blood is filtered per minute
- Urea and creatinine accumulate in the blood because the kidney cannot filter them fast enough
- Result: elevated BUN and serum creatinine = Azotemia
"Azotemia is a biochemical abnormality that refers to an elevation of blood urea nitrogen (BUN) and creatinine levels, related largely to a decreased GFR."
- Robbins, Cotran & Kumar - Pathologic Basis of Disease
In short: Low GFR → less filtration of waste → waste builds up in blood → azotemia.
2. Proteinuria - Why it Occurs
To understand this, you need to understand the normal glomerular filtration barrier and how it keeps proteins OUT of urine.
The normal filtration barrier has 3 layers:
| Layer | Role in keeping proteins out |
|---|---|
| Fenestrated endothelial cells (covered by glycocalyx) | Glycocalyx is negatively charged - electrically repels albumin (also negatively charged), preventing it from even reaching the GBM |
| Glomerular Basement Membrane (GBM) | Contains heparan sulfate proteoglycans (negative charge) + collagen type IV mesh - acts as a size and charge barrier |
| Podocyte foot processes + slit diaphragm (nephrin protein) | Final size-selective barrier; slit diaphragm is only 20-30 nm wide - too narrow for albumin (radius ~3.6 nm) to pass in significant amounts |
"The normal glomerulus is highly permeable to water and small solutes... and is impermeable to proteins of the size of albumin (~3.6-nm radius; 70 kDa) or larger."
- Robbins, Cotran & Kumar - Pathologic Basis of Disease
In nephritic syndrome:
Glomerular inflammation directly damages all three layers:
-
Endothelial injury - disrupts the glycocalyx, removing the electrostatic repulsion of albumin. Albumin can now reach the GBM in higher concentrations.
-
GBM disruption - inflammatory mediators and neutrophil enzymes (proteases, reactive oxygen species) degrade the GBM collagen and heparan sulfate, losing both size and charge selectivity.
-
Podocyte/slit diaphragm injury - foot process effacement and nephrin loss opens up "large pores" in the slit diaphragm, allowing proteins to spill through.
"Glomerular diseases are characterized by breaks in the glomerular capillary wall, thereby leading to hematuria with proteinuria because of loss of the selective barrier to particles based on size and charge."
- Goldman-Cecil Medicine
Why is proteinuria SUBNEPHROTIC (not massive) in nephritic syndrome?
This is a key distinction from nephrotic syndrome:
- In nephritic syndrome, the barrier disruption is partial and patchy - caused by inflammation
- In nephrotic syndrome (e.g., minimal change disease), there is diffuse, severe podocyte injury causing massive protein leak (>3.5 g/day)
- In nephritic syndrome, proteinuria is typically <3.5 g/day (subnephrotic range) because the primary injury is to the mesangium and endothelium, with less severe podocyte damage
Summary Table
| Feature | Mechanism | Result |
|---|---|---|
| Azotemia | Glomerular inflammation → ↓GFR → urea & creatinine not filtered | Elevated BUN + creatinine in blood |
| Proteinuria | Capillary wall damage → loss of size & charge selectivity of filtration barrier | Protein leaks into urine (subnephrotic range) |
| Hematuria | Same capillary wall damage → RBCs squeeze through | RBCs and RBC casts in urine |
| Hypertension | ↓GFR → Na & water retention → RAAS activation | Raised BP |
| Oliguria | ↓GFR → less filtrate formed | Reduced urine output |
All five cardinal features of nephritic syndrome trace back to a single event: inflammatory destruction of the glomerular capillary wall.

IMG_0132.jpg
I cant get 3rd immunoflorrnce of IgA nephropathy
Finding Sources
Loading Image
Reading File
Reading File
Got everything you need. Here is the full immunofluorescence picture of IgA nephropathy:
IgA Nephropathy - Immunofluorescence (IF) Pattern
The IF pattern is the defining diagnostic feature of IgA nephropathy (Berger disease).
What you see on IF:
Dominant/codominant mesangial IgA deposits - bright green granular fluorescence confined to the mesangial regions of the glomerulus (not along the GBM like in PSGN or Goodpasture).
Here is the actual IF image from Goldman-Cecil Medicine:
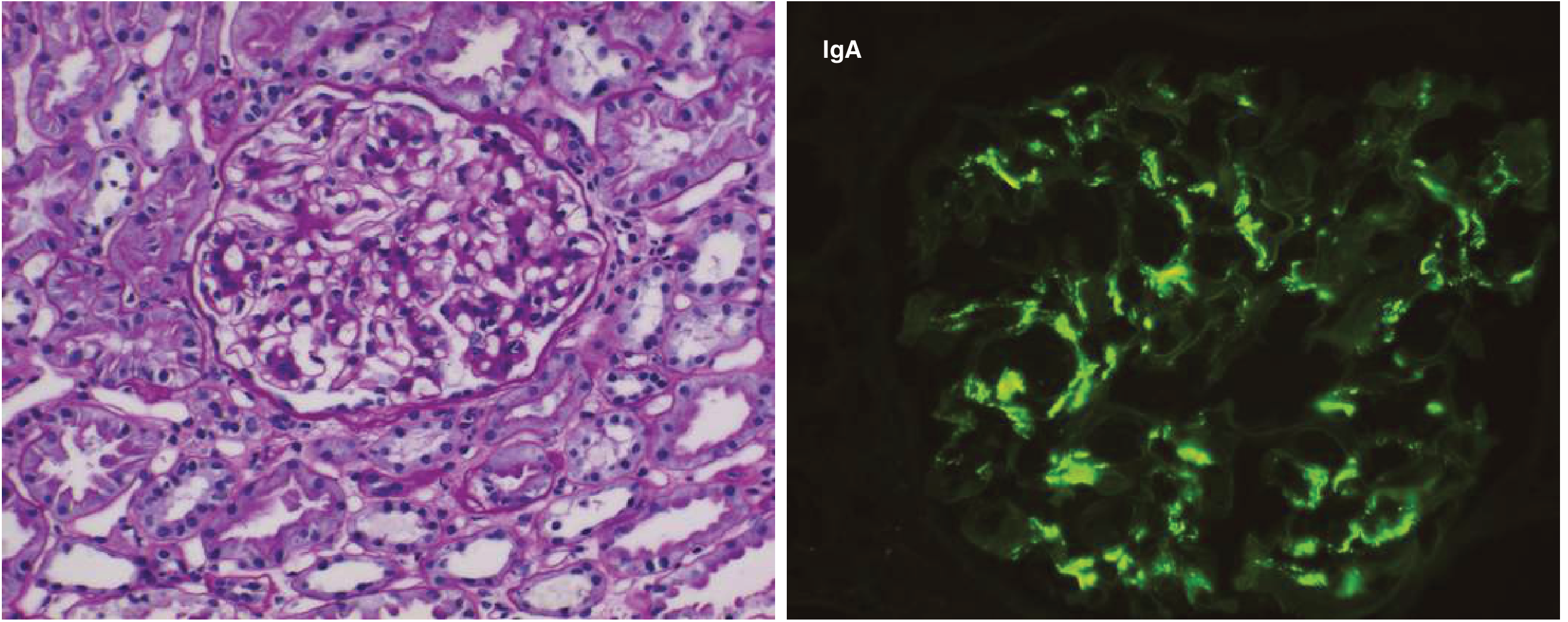
The right panel (green fluorescence) shows IgA lighting up the mesangium in a granular/mesangial pattern.
Full IF Composition:
| Immunoreactant | Presence |
|---|---|
| IgA | Dominant / codominant (MUST be present for diagnosis) |
| C3 | Often present (alternative pathway activation) |
| Properdin | Often present (confirms alternative pathway) |
| IgG or IgM | Smaller amounts, may be present |
| C1q / C4 (classical pathway) | Usually ABSENT |
"The characteristic immunofluorescence picture is of mesangial deposition of IgA, often with C3 and the alternative pathway protein properdin and smaller amounts of IgG or IgM. Early components of the classical complement pathway are usually absent."
- Robbins & Kumar Basic Pathology, p. 2405
The 3 Key IF Points to Remember (what your note probably cut off):
- Pattern: Mesangial/paramesangial (granular) - NOT linear, NOT subepithelial
- Dominant immunoglobulin: IgA (this is what makes the diagnosis - "dominant or codominant IgA")
- Complement pathway: Alternative pathway (C3 + properdin present; C1q ABSENT - no classical pathway activation)
Why Alternative Pathway?
IgA normally activates complement via the lectin or alternative pathway, NOT the classical pathway (which requires IgG/IgM + C1q). This is why C1q and C4 are absent in IgA nephropathy - a useful exam point to distinguish it from lupus nephritis (which shows C1q strongly) or PSGN (which shows granular IgG + C3).
Comparing the 3 Granular IF Patterns (exam favourite):
| Disease | IF Pattern | Location of deposits |
|---|---|---|
| IgA nephropathy | IgA dominant + C3 (alternative pathway) | Mesangium |
| PSGN | IgG + C3 (granular "starry sky") | Subepithelial + mesangial |
| Lupus nephritis | "Full house" (IgG, IgA, IgM, C3, C1q) | Mesangial + subendothelial + subepithelial |
I cant get anything
Asking for Preferences
Got it. Let me break this down as simply as possible with the actual image.
IgA Nephropathy - IF Pattern, Explained Simply
First, understand what IF actually IS
Immunofluorescence (IF) is a lab technique where you take the kidney biopsy, apply fluorescent antibodies that glow green when they bind to specific proteins (IgA, IgG, C3, etc.), then look under UV light.
Whatever glows green = that protein is deposited there.
What glows in IgA nephropathy?
Look at this image again:
- Left panel = Light microscopy (H&E stain) - shows mesangial cell proliferation
- Right panel = Immunofluorescence - the bright green spots = IgA deposits
Notice the green is clumped/patchy in the CENTER of the glomerular tuft - that is the mesangium.
The 3 things to know about where it lights up:
Normal glomerulus cross-section:
Capillary wall (GBM)
/
[Bowman's space] -- [Capillary loops] -- [Mesangium in the middle]
↑
THIS is where IgA deposits sit
Mesangium = the "scaffolding" tissue between the capillary loops, right in the center of the glomerulus.
So on IF, you see:
- Green fluorescence in the CENTER of the glomerular tuft
- NOT along the outer capillary walls (that would be GBM/subepithelial pattern like in PSGN or membranous)
- NOT a linear line (that is Goodpasture's)
- Patchy/granular clusters in the mesangial zones
Visual comparison - WHERE the glow sits:
| Disease | Where it glows on IF | Pattern |
|---|---|---|
| IgA nephropathy | Mesangium (center of tuft) | Granular, central |
| PSGN | Capillary walls + mesangium | "Starry sky" all over |
| Goodpasture | Along entire GBM | Smooth linear line |
| Membranous GN | Outer capillary wall (subepithelial) | Granular, peripheral |
Simple memory trick:
IgA = "I go to the mesAngium"
The IgA complexes are too big to cross the GBM, so they get trapped in the mesangium where they are filtered out. They pile up there, activate complement (alternative pathway - so C3 lights up too, but NO C1q), and cause inflammation.
What exactly lights up on the stain panel:
| Stain | Result |
|---|---|
| Anti-IgA | Bright green (dominant) |
| Anti-C3 | Often positive |
| Anti-IgG | Faint / minor |
| Anti-C1q | NEGATIVE (important!) |
The fact that C1q is absent tells you the classical complement pathway is NOT activated - IgA uses the alternative/lectin pathway instead. This is a key exam point.
Does this make it clearer? Or would you like me to draw out the structure of the glomerulus and show exactly where each type of deposit sits?
This is a shared conversation. Sign in to Orris to start your own chat.